


Julia Silva Marra1; Kioshe Rodrigues Siracava1; Leonardo Teodoro Duarte Alves1; Talissa Gomes Silva de Souza1; Mabel Duarte Alves Gomides2
Submitted on: 15/04/2021
Approved on: 12/07/2021
How to cite this article: Marra JS, Siracava KR, Alves LTD, Souza TGS, Gomides MDA. Hot asphalt burns: an epidemiological and therapeutic review. Surg Cosmet Dermatol. 2021;13:e20210030
Hot asphalt burns are a health threat due to the risk of death and adhesion to tissues.
A 40-year-old man suffered first and second-degree burns by hot asphalt on 20% of the body surface area. The asphalt adhered to the skin was removed on the 4th day of the ICU stay with liquid petroleum jelly, and the burns were treated with healing gel.
Burns caused by hot asphalt are serious and represent 1.4% of hospitalized cases. They affect young people in the skin and airways by inhaling the vapors.
Removing asphalt from the skin is a major therapeutic challenge.
Keywords: Burns. Burns, Chemical. Petroleum. Accidents. Accidents, Occupational
Burns result from the direct or indirect action of chemical or physical agents capable of producing large amounts of heat and causing damage to body tissues,1-3 which characterizes them as one of the most serious traumas among the types of accidents.2,4
Many victims are affected by burns worldwide,4 representing a serious public health problem,3,4 with high rates of morbidity resulting from physical and psychological sequelae,1-3 and mortality,1-3,5- 7 including in Brazil.4 The causes of death are mainly due to infections and systemic repercussions in extensive cases.1,8-10
Burns caused by hot asphalt are rare, accounting for about 1.8% of hospitalized cases.7,11 However, they represent a threat to the health of road pavers and roofers.7 This is because this product is composed of hundreds of harmful chemical substances, and its handling in construction occurs at high temperatures (approximately 140 °C to 250 °C), producing hot and toxic vapors and fumes and a viscous liquid that adheres to the skin.6,10,12,13
Occupational injuries and accidents at the workplace involving hot asphalt are peculiar because they comprise gas inhalation poisoning and severe mucosal and skin burn6 with adhesion of the asphalt mass,6,10,12,13 with the risk of infection and total or partial tissue destruction.10-12
The initial measures in the care of individuals burned by hot asphalt should be immediate, at the accident site, with the cooling of the asphalt followed by its removal with appropriate substances to avoid worsening the burn damage and its complications.9,10,14
This study aims to briefly review the literature on the topic and illustrate its importance with a case report and subsequent discussion.
A 40-year-old man was a victim of burns on the face, neck, and hands after an asphalt mixture pipe explosion during a work activity in road construction. His co-workers quickly assisted him with a continuous jet of water to cool the asphalt mixture. The patient was admitted to the emergency room conscious, hypothermic, with low oxygen saturation (85%) on room air, and hemodynamically stable. He presented burns to the airways caused by inhaling the hot gases released in the explosion. He also had burns on the skin, with superficial (first degree) and partial (second degree) thickness in 17% of the body surface (8% in the head, 1% in the cervical region, 5% in the anterior trunk, and 3% in the hands), with bitumen adhered to most of these areas (Figure 1).
The patient evolved with the need for orotracheal intubation, sedation, analgesia, mechanical ventilation, parenteral hydration, according to the Parkland formula, and was referred to the intensive care unit (ICU). He presented a significant improvement in respiratory condition with progression of ventilatory parameters within four days of ICU stay. However, due to the presence of adhered bitumen, mainly on the face, sedation and analgesia interruption was suspended. As this is an unusual situation, a team doctor researched the best treatment and then, together with the nursing staff, used liquid petroleum jelly to remove the bitumen from almost 90% of the compromised surface for approximately three hours (Figure 2). The burns were then treated with a healing ointment.
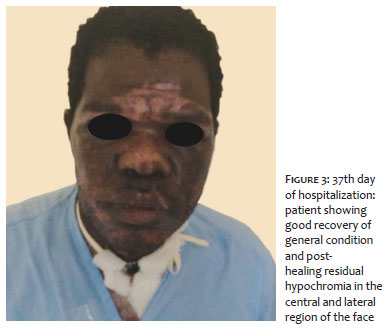
Due to the delay in extubation, the patient developed ventilator-associated pneumonia (VAP), septicemia, and acute renal failure (ARF). A sepsis protocol with broad-spectrum antibiotics, volume expansion, metabolic acidosis correction, and vasoactive drugs was instituted, in addition to conservative treatment with diuretics for ARF. On the 37th day of admission, the patient was discharged from the ICU in good general condition and excellent skin healing (Figure 3).
Burns are major health threats, with approximately one million cases a year in Brazil and six million victims annually worldwide, according to a 2015 estimate.3,4 Mortality from burns occurs in a more significant proportion in developing compared with developed countries.3 Among the relevant causes of burns, the civil construction environment stands out, as they result in highly complex cases.15
Occupational injuries and accidents at the workplace in civil construction represent about 10% to 15% of all work-related accidents in Brazil, with approximately 25% of severe cases, and they are relevant causes of morbidity and mortality.15,16 The professionals most affected in fatal cases are bricklayers ( 28%) and construction workers (14%), who are probably subjected to more stressful tasks due to the low level of professional qualification.17 The leading causes of these accidents are falls (37.3%) and contact with machines and tools (16%).16 Events associated with explosions or contact with heat sources, as in the present case, are responsible for only 1% to 2% of occupational injuries in civil construction. However, in general, they are serious cases.16,17 The profile of accidents victims at the workplace in civil construction in Brazil has a significant predominance of men (almost 100%), generally affecting young people aged between 21 and 40 years, with a mean age of 29.6 years (61.4%).16
Accidents caused by hot asphalt have a much higher lethality (approximately 7%) than that found in other accidents at the workplace (1% to 4%).7,18 Among them, 91% occur due to falls or spills, 4% because of hot asphalt pipes rupture (as the case reported), and 2% for traffic accidents.10 The most frequently affected areas are the upper limbs, followed by the head and/or face (44%), and cornea (11%), showing an average affected body surface of 13.1%.10 The average length of hospital stay is directly related to the extent of burned body surface, age, comorbidities, inhalation injuries, and associated trauma.4,10
It is important to emphasize that, despite bitumen, asphalt, and tar are different substances, the literature often mixes them, and they present a difficult differentiation with similar properties.10 They’re all nonpolar polycyclic aromatic hydrocarbons (PAH), with high volatility and high handling temperature.20 Understanding this spectrum of information allows similar approaches in emergency care situations,10 as in the clinical case presented.
Also, occupational injuries involving hot asphalt are peculiar because they comprise gas inhalation poisoning of asphalt fumes and severe skin burns.6 Intoxication occurs mainly due to the presence of carbon monoxide, hydrogen sulfide, and aliphatic hydrocarbons present in the substance, which can cause serious cardiovascular, respiratory, gastrointestinal, neurological, and ocular consequences.6
Regarding burns, which were the most prominent aspect in our report, hot asphalt presents very high temperatures at the time of accidents (approximately 140 ºC to 250 ºC).6,12 Inhaling fumes and volatile gases at this temperature burns the mucous membranes of the airways Also, in extensive burns, there is a high pulmonary impairment and high risk of death,2 in addition to complications caused by the hemodynamic repercussions of the fumes toxic effects6 and the burn extension.1
Despite cooling quickly, the heat retained by the hot asphalt can promote burns with varying depths in contact with the skin. It undergoes a solidification process with great adhesion to the skin when cooled, making its removal challenging.7,10,19 Therefore, it is often impossible to properly visualize the dimension of burns until entirely removing the substance.6 Furthermore, one of the most frequent complications of this type of burn is infections resulting from loss of continuity of intact skin.10
Another relevant consideration to burns from hot asphalt is the long-term risk of developing subsequent neoplastic diseases since the oxidative damage alters the genetic material of the affected tissues.12,19 Thus, the burn, through direct contact with these hydrocarbons, is a relevant carcinogen marker.13,20
This type of burn treatment requires a specialized and early approach to lesions to minimize the risk of complications and reduce morbidity and mortality.14 The most relevant initial approach is the immediate cooling of the chemical through immersion in water at the time of the accident, still at the site.6,14 This procedure is recommended as essential to prevent the hot asphalt heat from causing tissue destruction in greater depth and adjacent regions.6,14
Sequentially, the patient must be taken to the hospital emergency room with advanced life support for fluid resuscitation and airway management according to the extent and location of the burn.7 The clinical case addressed in this article required this care because it presented a burn in 17% of body surface and involvement of the face and airways. In the past, bitumen removal was performed through mechanical debridement, with undesirable results due to the healthy tissue removal and an increase in tissue exposure.12 Currently, the chemical principle of “like dissolves like”19 is applied, therefore, using nonpolar solvents to remove through micelle formation effectively.7,19 Despite the few comparative studies in the literature, the most indicated solvents are vaseline, vegetable oils, butter, and antibiotic ointments.6,10,19 Other types of chemical solvents, such as alcohol, acetone, kerosene, and gasoline, have been contraindicated in these cases because they are ineffective, irritating, and toxic.12 The surgical approaches have been necessary in about 42% of cases.6
The average time of emulsification to remove the substance adhered to the skin ranged from 20 minutes to a few hours.6,10,11 Some authors report experiences of clinical cases in which, one hour after the accident, they emulsified the asphalt mixture with an appropriate solvent for 20 minutes. Then, they could remove it without damaging the skin, followed by extubation and treatment completion.11 Thus, it is essential to emphasize the long period during which our patient was exposed to the substance until its removal, which probably contributed to the infectious disease’s complications and consequently prolonged hospitalization. It reflects the challenge of health services in dealing with this type of cases, especially due to the lack of scientific information in the literature.
The prognosis of these patients depends on age, the burn extension, and inhalation injuries. It’s worse in individuals over 60 years of age, with severe burns (more than 40% of body surface) and the presence of burns in the airways.3 To obtain a good quality of life after the accident, optimized and multidisciplinary care is necessary for the acute and late phases of the burn, thus avoiding emotional sequelae and unsightly scars.1-4,21 The improvement of healing results after removal of asphalt depends a lot on the care with the wound, such as debridement, grafts, and healing therapies.10
Even with a vast road network in the country, burns caused by hot asphalt mixture are still little discussed in Brazilian and world literature, and its treatment remains undefined. This situation promotes therapeutic challenges in the healthcare system and leads in harm to patients resulting from late management, which prolongs the length of hospital stay and increases treatment costs.
Given the current scenario of increasing road paving and technology evolution, we concluded that there is an emerging need for more discussions on the subject to be fostered and published in the literature. Hot asphalt burns are a condition that is easy to diagnose, simple and inexpensive to treat, but that requires prior and specific learning from the assistant physician. Therefore, the elucidation of cases with clinical presentation, management, and evolution becomes essential for disseminating knowledge on the subject.
Julia Silva Marra | 0000-0003-0422-1997
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Kioshe Rodrigues Siracava | 0000-0002-2859-9903
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Leonardo Teodoro Duarte Alves | 0000-0003-2475-4002
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Talissa Gomes Silva de Souza | 0000-0002-0053-3590
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Mabel Duarte Alves Gomides | 0000-0003-1253-9428
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Vale ECS. Primeiro atendimento em queimaduras: a abordagem do dermatologista. An Bras Dermatol. 2005;80:9-19.
2. Silva KP, Caparróz MR, Torquato JA. Prevalência de complicações respiratórias em pacientes com queimaduras internados num hospital público estadual de São Paulo. Rev Bras Queimaduras. 2010;9(4):130-5.
3. Hettiaratchy S, Dziewulski P. ABC of burns: Introduction. BMJ. 2004;328(7452):1366-8.
4. Dias LDF, Oliveira AF, Juliano Yara, Ferreira LM. Unidade de Tratamento de Queimaduras da Universidade Federal de São Paulo: estudo epidemiológico. Rev Bras Cir Plást. 2015;30(1):86-92.
5. Kilshaw AD, Chang C, Jivan S. Consistency an issue? – A review of UK burns service online information on burns first aid. Burns. 2019;45(1):258-60.
6. Yamazaki E, Shido K, Yamazaki K, Aiba S. Edible oil methods to remove asphalt on burns. J Dermatol. 2018;45(11):1331-36.
7. Burchardt T, Assmann T, Schulte KW, Ruzicka T, Eumann NJ. Management of dermatologic industrial accidents. Skin burns by bitumen as an example. Hautarzt. 2003;54(4):376–7.
8. Hettiaratchy S, Dziewulski P. ABC of burns: pathophysiology and types of burns. BMJ. 2004;329(7458):148.
9. D’Avignon LC, Hogan BK, Murray CK, Loo FL, Hospenthal DR, Cancio LC, et al. Contribution of bacterial and viral infections to attributable mortality in patients with severe burns: an autopsy series. Burns. 2010;36(6):773-9.
10. Bosse GM, Wadia SA, Padmanabhan P. Hot asphalt burns: a review of injuries and management options. Am J Emerg Med. 2014;32(7):820.e1-3.
11. Bozkurt A, O’Dey D, Pallua N. Treatment of hot bitumen-contact-burn injuries. Burns. 2008;34(7):1053–4.
12. Iuchi M, Sugiyama M, Oyatsu Y, Fukai T. The comparative study of solvents to expedite removal of bitumen. Burns. 2009;35(2):288-93.
13. Fustinoni S, Campo L, Cirla PE, Martinotti I, Buratti M, Longhi O, Foà V, et al. Dermal exposure to polycyclic aromatic hydrocarbons in asphalt workers. Occup Environ Med. 2010;67(7):456–63.
14. Pruitt BA, Edlich RF. Treatment of bitumen burns. Ann Emerg Med. 1982;11(12):697.
15. Scussiato LA, Sarquis LMM, Kirchhof ALC, Kalinke LP. Epidemiological profile of serious accidents at work in the State of Paraná, Brazil, 2007a 2010. Epidemiol Serv Saúde. 2013;22(4):621-30.
16. Silveira CA, Robazzi MLCC; Walter EV, Marziale MHP. Acidentes de trabalho na construção civil identificados através de prontuários hospitalares. Rev Esc Minas. 2005;58:39-44.
17. Mangas RMN, Gómez CM, Thedim-Costa SMF. Acidentes de trabalho fatais e desproteção social na indústria da construção civil do Rio de Janeiro. Rev Bras Saude Ocup. 2008;33:48-55.
18. Pafiadache C, Zanini RR, Souza AM. Estudo das taxas de letalidade por acidente de trabalho no Rio Grande do Sul. Brasil. Espacios. 2014;35(3):4.
19. Nawrocki PS, Thompson H. Using baby oil to remove asphalt from burn. CJEM. 2016;18(3):239-40.
20. Serdar B, Lee D, Dou Z. Biomarkers of exposure to polycyclic aromatic hydrocarbons (PAHs) and DNA damage: a cross-sectional pilot study among roofers in South Florida. BMJ Open. 2012 19;2(4):e001318.
21. Sheridan RL, Hinson MI, Liang MH, Nackel AF, Schoenfeld Da, Ryan CM, et al. Long-term outcome of children surviving massive burns. JAMA. 2000; 283(1):69-73.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}