


Flávia Trevisan1; Nataly Portilla Maya2; Guilherme Canho Bittner3; Bruno de Carvalho Fantini4; Felipe Bochnia Cerci5,6
Submitted on: 14/02/2021
Approved on: 04/04/2021
Financial support: None.
Conflict of interest: None.
How to cite this article: Trevisan F, Maya NP, Bittner GC, Fantini BC, Cerci FB. Perioral reconstruction after Mohs micrographic surgery: analysis of 108 cases. Surg Cosmet Dermatol. 2021;13:e20210022.
INTRODUCTION: The perioral region is commonly affected by non-melanoma skin cancer. Mohs micrographic surgery is the treatment of choice in this area because it has the highest cure rate and preserves healthy tissue. Several methods are available for restoring the perioral region, and their selection is influenced by the surgical wound characteristics and the surgeon's preference.
OBJECTIVE: Describe the authors’ experience in perioral reconstruction after Mohs micrographic surgery and analyze the repair methods most frequently performed.
METHODS: Retrospective study of consecutive cases submitted to Mohs surgery and perioral reconstruction.
RESULTS: The study included 108 cases from 103 patients. The mean number of Mohs surgery stages was 1.4, and the mean defect size was 16 mm. Primary closure was the most used technique for reconstruction, followed by flaps (mainly V-Y, single advancement, and rotation). The association of repair methods was used in 28.7% of cases, mostly combined with flaps. Four patients had complications (necrosis and graft infection, trapdoor effect, and partial wound dehiscence).
CONCLUSION: Primary closure was the most frequent repair method, followed by flaps. Knowing reconstruction strategies and possibilities of associations is essential for proper restoration of the perioral region, maintaining its functionality, sensitivity and aesthetics.
Keywords: Lip; Lip neoplasms; Mohs surgery; Skin neoplasms
The perioral region is commonly affected by non-melanoma skin cancer. While basal cell carcinoma (BCC) often affects the cutaneous portion, squamous cell carcinoma (SCC) is more prevalent in the vermilion (mucosa).1 Surgical removal, either by wide local excision or micrographic surgery is the treatment of choice for malignant skin tumors in the perioral region.2
Mohs micrographic surgery (MMS) is preferable in the perioral region, as it has the advantages of a higher cure rate and preservation of healthy tissue.3 The highest cure rate comes from the complete examination of the surgical margins during the procedure.4 Wide local excision on the other hand assesses approximately 1% of the margins.5 The preservation of healthy tissue in the MMS can save the patient from more complex reconstructions. However, challenging reconstructions may be necessary even with MMS, and a thorough margins examination is essential to perform them safely.2
When choosing the repair method for this area the size of the surgical wound, its location (subunit affected), and its depth should be considered, among other factors. A satisfactory surgical outcome is achieved when the site’s functionality, mobility, sensitivity, and esthetics are maintained.2
This study aims to describe the authors’ experience in perioral reconstruction after MMS and to analyze the most used reconstruction methods.
This is a retrospective study of consecutive cases submitted to MMS and perioral reconstruction performed by the authors between January 2017 and August 2020. The cases are from the authors’ private clinics and from a university hospital where one of the authors works. The ethics committee approved the study, protocol 30743520.2.0000.0103.
Except for one surgery performed under local anesthesia and sedation, all procedures were performed under local anesthesia. Postoperatively, antibiotics (cephalexin 500 mg 6/6 hours for seven days, cefadroxil 500 mg 12/12 hours for four days, or amoxicillin 500 mg 8/8 hours for seven days) were used in more complex, long duration surgeries or when a significant portion of mucosa was removed.
For data analysis, we reviewed photographic documentation and data such as age, gender, Fitzpatrick skin phototype, tumor characteristics, size of the wound and anatomical subunits involved, number of MMS stages, reconstruction performed, antiplatelet or anticoagulants use, and postoperative complications.
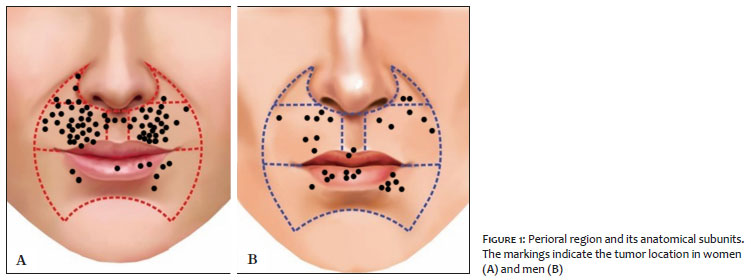
The perioral subunits were divided into upper cutaneous lip (UCL), lower cutaneous lip (LCL), philtrum, apical triangle, superior vermilion, and inferior vermilion (Figure 1).6 The reconstruction methods were divided into secondary intention healing, primary closure, flaps, or graft. When more than one method was used, it was called combined reconstruction. For analysis of repair methods, only those that repaired perioral subunits were considered.
Complications were divided into two groups, short or long-term. Bleeding that required re-intervention, hematoma, infection, dehiscence, and necrosis of the flap/graft (partial or total) were considered short-term. Considerable anatomical distortion and functional impairment (difficulty speaking and impaired mobility) were defined as long-term.
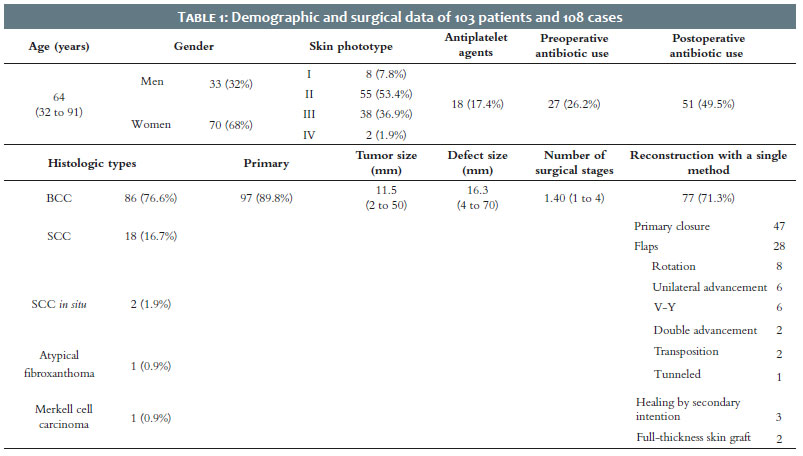
The study included 108 cases from 103 patients. Table 1 describes the demographic and surgical data. BCC was the most prevalent tumor in all perioral subunits, except in the lower vermilion, where only SCCs were found (ten invasive and one in situ).
Figure 1 shows the perioral subunits. The upper cutaneous lip (n=83) was the subunit mostly affected, followed by the lower vermilion (12), apical triangle (5), philtrum (4), lower cutaneous lip (3), and upper vermilion (1). In 35 cases, the tumor extended over more than one perioral subunit, and in 12, the extension reached another facial unit (mainly malar, in eight cases). Only three cases had full-thickness lip defects.
Seventy-seven cases underwent reconstruction with a single method, and 31 cases underwent combined methods. The most used procedure was flaps combined with other methods. Flaps were used in 50 cases, half as a single technique and half associated with other methods. The following flaps were used: V-Y (n=15), single advancement (n=14), rotation (n=11), transposition (n=4), double advancement (n=3), hinge (n=2), and tunneled island flap (n=1).
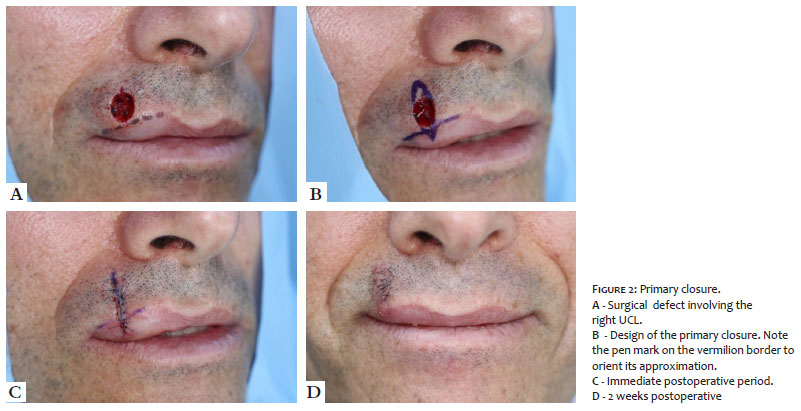
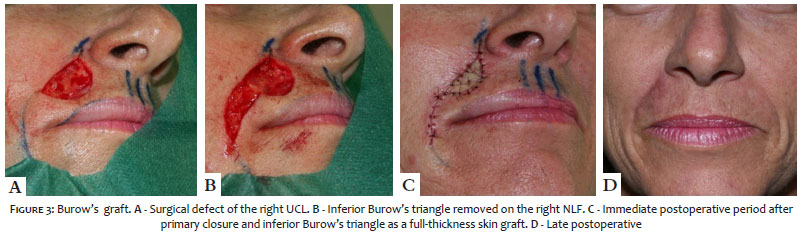
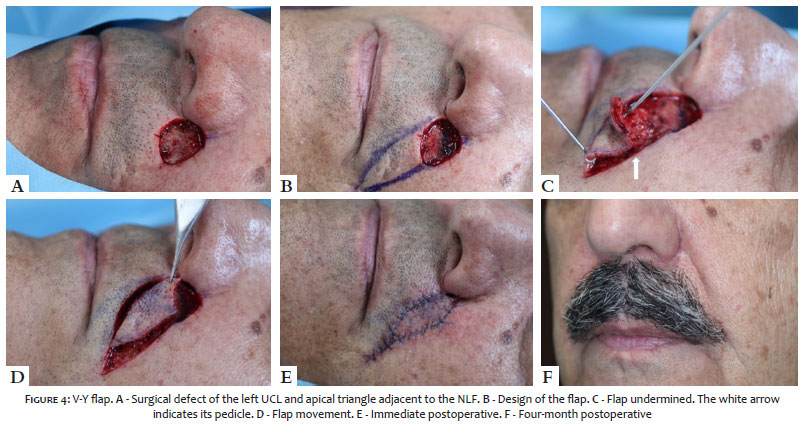
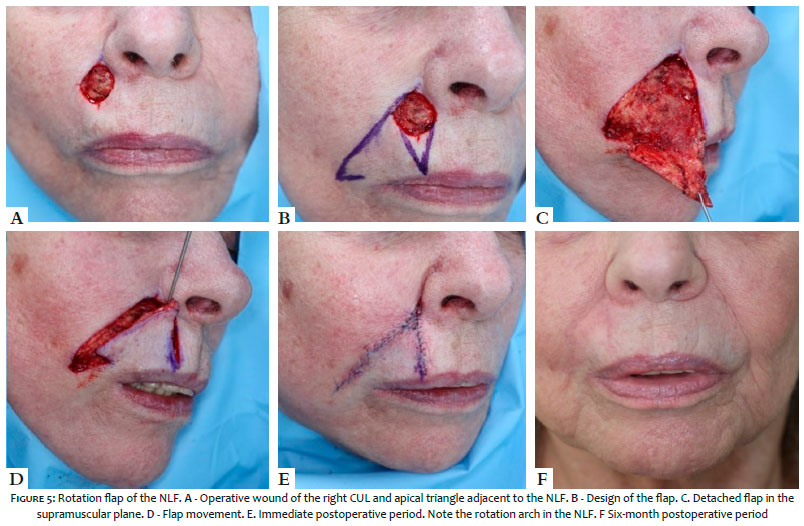
For tumors primarily involving the UCL, 47 cases were restored primarily (Figure 2). In nine cases, primary closure was combined with a full-thickness skin graft (Figure 3), and one with graft and advancement flap. Flaps were the second most common technique in this cosmetic subunit (Figure 4), 33 cases, and rotation was the most used type (n=10) (Figure 5). Two patients were referred by plastic surgery to perform MMS and, after its completion, returned for reconstruction with the plastic surgeon. Both were restored with primary closure.
In the lower vermilion, ten cases were repaired with primary closure. Among them three were combined with an advancement flap and two with secondary intention healing. An extensive but superficial case was left to heal by secondary intention. The most used method was also the primary closure in the apical triangle, philtrum, superior vermilion, and lower cutaneous lip.
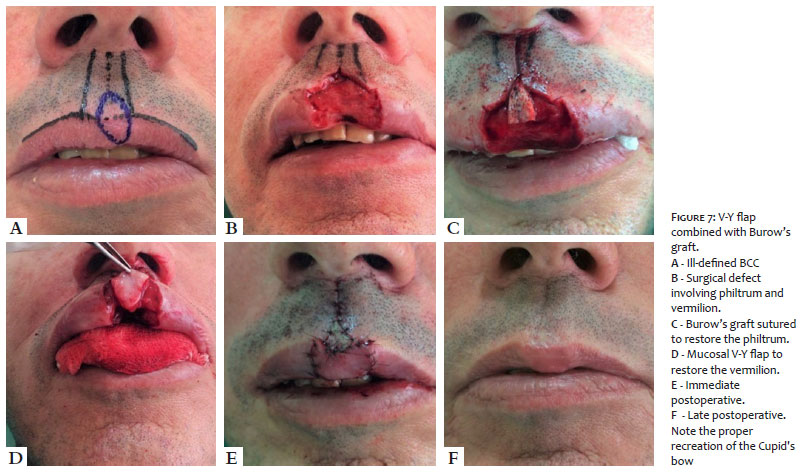
In wounds involving more than one perioral subunit (n=35), the method most used for reconstruction was flaps (n=17) (Figure 6), followed by primary closure (n=15), and grafts (n= 2). Among these 35 cases, four required the association of more than two methods (Figure 7).
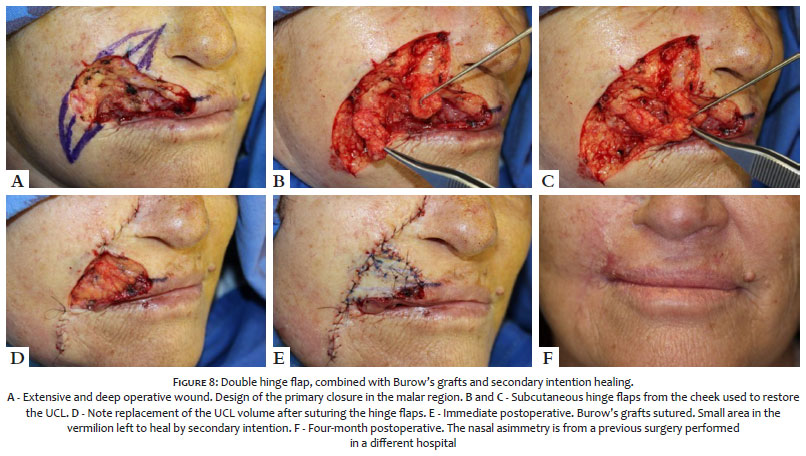
Preoperative prophylactic antibiotics were used in 27 patients and postoperatively in 51. Complications occurred in four cases: two trapdoors treated with intralesional steroids, one partial dehiscence, and one infection with graft necrosis (Figure 8). The latter case culminated in a partial loss of suction capacity due to partial removal of the orbicularis muscle. The other complications evolved with a satisfactory resolution.
Surgical reconstruction of the perioral region can influence mouth function, aesthetics and impact patients’ social interactions.2 Tumors treated with wide local excision can lead to unnecessary defects of considerable size and thickness when “sacrificing healthy skin”. They may require complex flaps and sometimes a multidisciplinary approach. Furthermore, wide local excision can cause significant morbidity.6,7 Conversely, MMS preserves the healthy skin, allowing the complete examination of surgical margins during the intraoperative period, leading to reconstructions with less morbidity and lower risk of complications. Also, MMS enables complex reconstruction methods by assuring that the tumor has been completely removed.2 The present study demonstrated the variety of reconstruction options for the perioral region.
Like previous publications, BCC was the most prevalent malignant tumor in the cutaneous portion of the lip, while SCC was the most common (and the only one) in the vermilion.1 In 32% of cases (n=35), the tumor extended through more than one perioral subunit, and in 11%, the extension reached another facial unit (mainly the malar). This demonstrates the complexity of repairs in the perioral region. The involvement of sites beyond the nasolabial fold (NLF) is important because, in some cases, it is preferable to combine reconstruction methods for better results.
After tumor removal from the perioral region, surgical wounds can be divided according to thickness, size, and location. These factors help to guide the choice of the reconstruction method.8 According to a 2009 literature review, the most common method for reconstructing the perioral region was primary closure.9 In the present study, 77 reconstructions used a single repair method, mainly primary closure (n=47) (Figure 2), followed by flaps (n=25). In reconstructions using combined techniques (n=31), the most associated secondary method was grafts (n=14) (Figure 3), followed by flaps (n=9), secondary intention healing (n=7), and primary closure (n=1). These data demonstrate the importance of knowing several surgical techniques for proper restoration of the perioral region. It is vital to keep in mind that wounds in the mucosa without the involvement of the orbicularis muscle can be left to heal by secondary intention, obtaining excellent results as described in the literature.10-12 Also, it is noteworthy that this option is usually only possible when performing MMS since wide local excision removes deeper margins due to postoperative margin examination of 1-2% of the margins.5
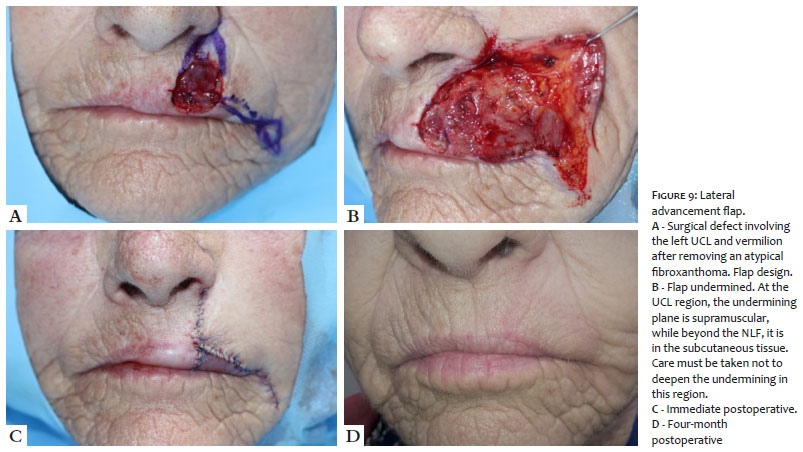
In the UCL, the most affected subunit, 37 cases were restored by primary closure. Thirty-three cases by flaps, mainly V-Y (Figure 4), advancement (Figure 9), and rotation (Figure 5). When adequately performed advancement and rotation flaps yield good results in the perioral region, allowing maintenance of function, sensitivity, and symmetry of the lips, in addition to avoiding microstomy.13 These flaps aesthetic result is satisfactory as they maintain the color and texture of the tissues around the surgical defect, and camouflage the scars in between the boundaries of the facial anatomical units.14,15 For the advancement flap, it is essential to position the incisions between the anatomical subunits (vermilion/UCL, UCL/alar base) whenever possible.16 For the rotation flap, the arch should be positioned in the NLF, thus remaining hidden after the healing. Cases requiring greater mobility of the rotation flap can receive a back cut in the distal portion of the arch.15
The V-Y island pedicle flap is better indicated when one of the incisions can be camouflaged in the NLF. For extensive cases, adjacent to the philtrum and affecting almost the entire area between the nasal vestibule and vermilion, one should consider removing the remaining skin to camouflage both incisions: one between vermilion and UCL, the other between nose and UCL.17 In addition to the oblique/lateral design, the V-Y island pedicle flap can be performed vertically for wounds in the philtrum or adjacent to it. The island flap can also recruit tissue beyond the NLF. However, blunting of the NLF can cause visible asymmetry. Few options do not lead to some NLF asymmetry degree in these cases. As with all island flaps, its proximal portion must be “thinned’ according to the surgical wound thickness to reduce the risk of the trapdoor effect.17
With the preservation of healthy tissue due to MMS, the defects are smaller and thinner than those from wide local excision, often reducing the need for more complex reconstruction.18 In addition to V-Y, advancement, and rotation flaps, transposition (Figure 6) and tunneled flaps were used. We did not need to perform flaps indicated for extensive full-thickness wounds, such as the Abbé or Karapandzic flap, as the three full-thickness cases were relatively small and managed with less complex reconstructions.7
It is important to emphasize that the National Comprehensive Cancer Network (NCCN) does not recommend the use of flaps in cases that the surgical margins were not completely assessed. 19 This limits the reconstructive options, affecting the functional and esthetic restoration. Therefore, MMS, in addition to having the highest cure rates to treat cutaneous carcinomas, allows the Mohs surgeon to safely restore the wound using flaps, often necessary for better outcomes.5
The use of pre and postoperative antibiotics is a controversial topic in dermatologic surgery.20-23 Cutaneous surgeries are considered clean, but the proximity to the oral cavity makes the perioral region a site with a significant chance of potentially contaminated surgeries.24 This study used preoperative prophylactic antibiotic therapy in 26.2% of cases and postoperative in 49.5%, reflecting the difficulty in anticipating the wound size and the reconstruction method to be performed. With a low mean of surgical stages (which reduces the surgical time) and appropriate indication for antibiotic therapy, there was only one case of postoperative infection of a recurrent morpheaform BCC (treated by wide local excision eight years earlier). The tumor extended from the UCL to the upper vermilion and philtrum, leading to a 48 mm surgical defect repaired with a hinge flap combined with full-thickness skin graft and secondary intention. In this case, despite the use of pre and postoperative antibiotics, there was infection and graft necrosis. However, post-operative care and additional antibiotics led to a satisfactory outcome, except for the slight functional impairment (suction) secondary to a significant loss of orbicularis muscle due to tumor’s aggressiveness (Figure 8).
Other complications were two cases of trapdoor, one after a V-Y flap and the other secondary to a tunneled flap both in the UCL. Both had a good response with intralesional steroids (triamcinolone acetonide 20 mg/ml). There was one case of partial dehiscence in the apical triangle following primary closure.
Preserving the function and volume of the perioral region is challenging because even minor defects can impair the lips’ movement, competence, and symmetry. The surgeons must invest all their efforts in resolving the disease with a satisfactory aesthetic-functional surgical outcome. As recommended by the NCCN, reconstructions, especially in cosmetic sensitive areas, should ideally be performed after complete tumor resection confirmed by histological analysis of 100% of the surgical margins perioperatively as in MMS.19 The Mohs surgeon should be able to perform complex and straightforward reconstructions in the perioral region. More challenging cases may require a multidisciplinary approach.
Primary closure was the most used technique for reconstruction, followed by flaps (mainly V-Y, unilateral advancement, and rotation). Combined methods were performed in 28.7% of cases. A combined approach is better indicated for wounds involving cutaneous and mucosal subunit, such as UCL and vermilion.
Knowing the reconstruction strategies and possibilities of associations is essential for the proper reconstruction of the perioral region, maintaining its functionality, sensation and aesthetics.
Flávia Trevisan 0000-0001-5855-3685
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Nataly Portilla Maya 0000-0002-0325-7640
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
Guilherme Canho Bittner 0000-0002-5892-4391
Statistical analysis; approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation.
Bruno de Carvalho Fantini 0000-0003-1192-8376
Statistical analysis; approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Felipe Bochnia Cerci 0000-0001-9605-0798
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Queen D, Knackstedt T, Polacco MA, Collins LK, Lee K, Samie FH. Characteristics of Nonmelanoma SkinCancers of Cutaneous Perioral and Vermilion Lip Treated by Mohs Micrographic Surgery. J Eur Acad Dermatol Venereol. 2019;33(2):305-11.
2. Hafiji J, Hussain W, Salmon P. Reconstruction of perioral defects post-Mohs micrographic surgery: a dermatological surgeon's approach. Br J Dermatol. 2015;172(1):145-50.
3. Hafiji J, Hussain W, Salmon P. Mohs surgery spares the orbicularis oris muscle, optimizing cosmetic and functional outcomes for tumours in the perioral region: a series of 407 cases and reconstructions by dermatological surgeons. Br J Dermatol. 2015;172(1):294-6.
4. Tolkachiov SN, Brodland DG, Coldiron BM, Fazio MJ, Hruza GJ, Roenigk RK, et al. Understanding Mohs Micrographic Surgery: a review and practical guide for the nondermatologist. Mayo Clin Proc. 2017; 92(8):1261-71.
5. Kimyai-Asadi A, Goldberg LH, Jih MH. Accuracy of serial transverse cross-sections in detecting residual basal cell carcinoma at the surgical margins of an elliptical excision specimen. J Am Acad Dermatol. 2005;53(3):469-74.
6. Gaylon S W, Frodel JL. Lip and perioral defects. Otolaryngol Clin North Am. 2001;34(3):647-66.
7. Wollina U. Reconstructive surgery in advanced perioral non-melanoma skin cancer. Results in elderly patientes. J Dermatol Case Rep. 2014;8(4):103-7.
8. Johnson AR, Egeler SA, Wu WW, Bucknor A, Ibrhim AMS, Lin SJ. Facial reconstruction after Mohs Surgery: a critical review os defects involving cheek, forehead and perioral region. J Craniofac Surg. 2019;30(2):400-7.
9. Faulhaber J, Geraud C, Goerdt S, Koenen W. Functional and aesthetic reconstruction of full-thickness defects of the lower lip after tumor resection: analysis of 59 cases and discussion of a surgical approach. Dermatol Surg. 2010;36(6):859-67.
10. Gloster J, Hugh M. The use of second-intention healing for partial-thickness Mohs defects involving the vermilion and/or mucosal surfaces of the lip. J Am Acad Dermatol. 2002;47(6):893-7.
11. Aimee LL, Hanke CW. Second intention healing for intermediate and large postsurgical defects of the lip. J Am Acad Dermatol. 2007;57(5):832-5.
12. Donigan JM, Millican EA. Cosmetic and Functional Outcomes of Second Intention Healing for Mohs Defects of the Lips. Dermatol Surg. 2019;45(1):26-35.
13. Ergün SS. Reconstruction of the labiomental region with local flaps. Dermatol Surg. 2002;28(9):863-5.
14. Joo-Hak K, Ahn CH, Kim S, Lee WS, Oh S. Effective method for reconstruction of remaining lower lip vermilion defect after a mental V-Y advancement flap. Arch Craniofac Surg. 2019; 20(2):76-83.
15. Cerci, FB. Rotation flap for the reconstruction of the cutaneous upper lip after Mohs micrographic surgery. Surg Cosmet Dermatol. 2017;9(2):83-6.
16. Tolkachjov SN. Reconstruction for a large central upper mucosal lip defect. Dermatol Surg. Epub March 2020.
17. Griffin GR, Weber S, Baker, Shan R. Outcomes following V-Y advancement flap reconstruction of large upper lip defects. Arch Facial Plast Surg. 2012;14(3):193-7.
18. Touma DJ. Mohs' surgery to reduce the size of facial defects and necessity for complex repairs. Plast Reconstr Surg. 2002;110(6):1601.
19. Bichakjian CK, Olencki T, Aasi SZ, Alam M, Andersen JS, Berg D, et al. Basal cell skin cancer, version 1.2016, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2016;14(5):574-97.
20. Levin EC, Chow C, Makhzoumi Z, Jin C, Shiboski SC, Arron ST. Association of postoperative antibiotics with surgical site infection in Mohs Micrographic Surgery. Dermatol Surg. 2019;45(1):52-7.
21. Ahmed M, Gniadecki R, Taher, M. Oral and intraincisional antibiotic prophylaxis in Mohs Surgery: a systematic review and meta-analysis. Dermatol Surg. 2020;46(4):558-60.
22. Taylor O, Li JN, Carr C, Garcia A, Tran S, Srivastava D, et al. The effect of antibiotic prophylaxis on infection rates in mohs micrographic surgery: a single institution retrospective study. 2021 Oct;313(8):663-667.
23. Lin MJ, Dubin DP, Giordano CN, Kriegel DA, Hooman K. Antibiotic practices in Mohs Micrographic Surgery. J Drugs Dermatol. 2020;19(5):493-7.
24. Center for Disease Control and Prevention (CDC). "Patient Safety Protocol." Em The National Healthcare Safety Network (NHSN) Manual. 2008.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}