


Douglas Haddad Filho1; Flávia Fenólio Nigro Marcelino2; Paola Assunção Mendes2; Marcela Haddad Parada3; Carolina Soutto Mayor Mangini3
Submitted on: 04/03/2021
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
How to cite this article: Haddad Filho D, Marcelino FFN, Mendes PA, Parada MH, Mangini CSM. Retroauricular flap: case report. Surg Cosmet Dermatol. 2021;13:e20210012 p. 1-5
Basal cell carcinoma (BCC) can affect the auricular region in several locations and sizes, with or without cartilage involvement. Sometimes resections are small and reconstructions are simple. Other times, when the lesions are more extensive, reconstructions are more complex, considering the limited amount of skin in the area and the peculiarity of the structures involved. We report a case of a retroauricular flap staged in two stages, after the excision of a BCC on the posterior face of the auricle, with partial involvement of the cartilage, showing a great aesthetic and functional result both in the recipient and donor area.
Keywords: Carcinoma, basal cell; Surgical flaps; Skin neoplasms; Ear neoplasms; Rotation
Basal cell carcinoma (BCC) is a malignant neoplasm that mostly affects fair-skinned individuals, accounting for 70% of skin tumors.1,2 It occurs mainly on skin exposed to sunlight and is characterized by a high potential for local invasion and low metastatic risk.3,4,5
The auricle can be affected by this neoplastic lesion, which must be surgically removed, especially considering its local destructive potential. The reconstruction is proportional to the size of the lesion and the structures involved, ranging from a simple skin fusiform excision or a skin and cartilage wedge resection to the reconstruction of the entire auricle from cartilage grafting and various operative steps.5,6
The anatomy of the ear is quite complex, requiring detailed anatomical knowledge for a good surgical result. Its outer region comprises the auditory meatus and auricle, formed by elastic cartilage and covered by thin skin. They present scarce vascularization and are connected to the perichondrium.1,6
A 67-year-old man presented an ulcerated and bleeding lesion with raised edges on the posterior face of the right auricle, starting two years ago and increasing progressively. Upon examination, the lesion presented 5 cm in the craniocaudal and 2 cm in the latero-lateral direction, and hardening of the auricle’s consistency, suggesting the possibility of cartilage involvement.
The first surgery was performed under general anesthesia to excise the lesion. We conduct the removal with 0.5 cm safety margins on the sides, for the entire thickness of the skin with perichondrium, and partially for the full cartilage length. The frozen section pathology showed all margins free of neoplasia (Figure 1).
We proposed a skin flap in the retroauricular region to cover the defect, measuring approximately 4 cm x 2 cm, with the longest horizontal axis. It was elevated and sutured in the recipient area, respecting a skin island where the retroauricular sulcus resided. Its edges were sutured together, forming a tunnel. The flap remained in this condition for 21 days (Figures 2 and 3).
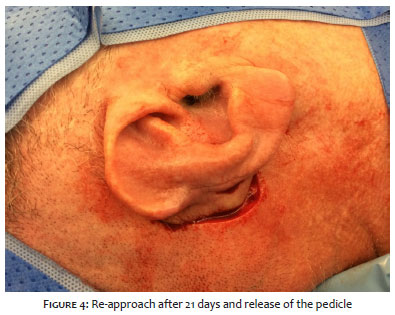
After this period, the flap was released from its pedicle, and the skin tunnel of the retroauricular sulcus was undone (Figure 4). Thus, the flap was wholly sutured in the recipient area, completing the defect closure (Figure 5). The donor area was closed using a rotation flap, 5 cm in length (Figures 6 and 7). Both flaps evolved with excellent perfusion (Figure 8).
Basal cell and squamous cell carcinoma are malignant neoplasms formed from keratinocytes, called “non-melanoma skin cancer”. They are the most incident neoplasms, with values still on the rise. Male gender and older age are independent risk factors for developing BCC. Intense and intermittent exposure to solar radiation is associated with BCC development due to mutagenesis caused by ultraviolet radiation, which is exacerbated in individuals with fair skin, red or blond hair, and light eyes.3,7,8,17,18,19
The most common clinical presentation of BCC is a pearly papule or nodule with telangiectasias and raised borders. In some cases, crusts or central ulceration may appear. Patients may complain of a non-healing, sometimes bleeding, asymptomatic, or itchy wound. Biopsy of the site is the standard procedure for diagnosing BCC. Some lesions may exhibit more than one histopathological pattern, and the nodular and micronodular forms are the most common. Morpheaform and infiltrative subtypes and lesions with micronodular or basosquamous histopathological changes are more aggressive variants.3,7,17,18
While most BCCs grow indolently concerning local invasion, a small portion progresses to locally advanced and metastatic tumors, usually due to neglect.7,17,18
Defects related to skin cancer represent one of the most common reasons for ear reconstruction surgery. The rotation flap is an alternative to the primary closure since the latter can deform the auricle. 6,9,20,21
The option of reconstructing the auricle with the staged retroauricular flap (SRF) is based, above all, on the abundant blood supply at this site, coming from the posterior auricular, superficial temporal, and occipital arteries. We agree with this hypothesis because there is an extensive vascular distribution in the scalp. Irrigation of the retroauricular flap can come from the posterior auricular artery or superficial temporal artery, depending on how the flap is used. Even though staged rotation is necessary, as in the case reported, the quality of the retroauricular skin is beneficial for facial reconstructions, considering the tissue’s color, texture, and thickness. Also, the donor area in the posterior region of the ear is hidden and presents, for the most part, good healing.11,12,22,24,25
The first surgical stage performs an interpolation flap when an intact skin island between the donor and recipient area is responsible for maintaining as much of the original anatomy of the site as possible. The procedure keeps a healthy skin island in the auricular sulcus between the donor and recipient area.1,13,23,24 This procedure is performed because, after 21 days, the flap no longer depends on its pedicle, with the new recipient area being responsible for the irrigation of this tissue.
The second surgical stage establishes the rotation flap, consisting of the curvilinear displacement of tissue adjacent to the surgical defect, originating from the scalp. Also, the flap can stretch the elastic tissues to cover the defect, redirecting the closing tension, as its points of greater tension run along its distal edge instead of its length.14,15,16,26,27
The need for scalp rotation flap to close the donor area of the retroauricular flap is commonly criticized. However, this procedure easily closes the area simultaneously by releasing the pedicle of the retroauricular flap. Also, the flap could be expanded in its dimension in cases of even more extensive defects.23,24,26,27
Other flap options could be used for reconstruction. Still, it is necessary to pay attention to the possibility of compromising the retroauricular sulcus or using skin with very different characteristics from the auricle tissue.10,20,21,24
Another way to use this flap is vertical, being pedicled in the lower region. Nevertheless, it is believed that it is more vulnerable regarding vascularization and, in addition, the donor site would not close primarily, requiring a hair flap in the glabrous skin area. Note that the release of the pedicle would also be necessary, therefore, requiring two surgical stages.
Analyzing the anatomy of the perforating arteries in this region, we could prepare a flap that could be transposed in a single stage. However, in practice, we do not believe that any scalp flap would reach the recipient area, even using helix rotation.
The two-stage interpolation flap, followed by a rotation flap, is an effective method for reestablishing the auricle. This procedure is capable of maintaining the anatomy of the donor and the recipient area of the flap.
Douglas Haddad Filho 0000-0001-9304-4739
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Flávia Fenólio Nigro Marcelino 0000-0003-4057-5143
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Paola Assunção Mendes 0000-0002-1116-9819
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marcela Haddad Parada 0000-0001-5616-829X
Study design and planning; preparation and writing of the manuscript critical; literature review; critical revision of the manuscript.
Carolina Soutto Mayor Mangini 0000-0002-4354-1347
Study design and planning; preparation and writing of the manuscript critical; literature review; critical revision of the manuscript.
1. Pavezzi PD, Kondo RN, Pontello Júnior R, Lena CP, Kippert JP. Retalho de interpolação para fechamento de defeito cirúrgico na cauda da hélice da orelha. Surg Cosmet Dermatol. 2017;9(4):334-7.
2. Chinem VP, Miot HA. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
3. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med. 2005;353(21):2262-9.
4. Alexandre L, Silva RP, Tacani RE, Liebano RE. A importância da fisioterapia nas técnicas de reconstrução cutânea - enxertos e retalhos. Fisioterapia Ser. 2007;2(3):183-7.
5. Pereira CCA, Sousa VB, Silva SCMC, Lima Santana CNL, Carmo MCL, Macedo PRWC. Carcinoma basocelular de localização inusitada na orelha - reconstrução cirúrgica. Surg Cosmet Dermatol. 2016;8(4):362-5.
6. Smith RM, Byrne PJ. Reconstruction of the ear. Facial Plast Surg Clin North Am. 2019;27(1):95-104.
7. Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-17.
8. Waldman A, Schmults C. Cutaneous Squamous Cell Carcinoma. Hematol Oncol Clin North Am. 2019;33(1):1-12.
9. Tinklepaugh A, Husain Z, Libby TJ, Ciocon D. Reconstruction of a full-thickness auricular defect after Mohs micrographic surgery. Dermatol Surg. 2018;44(12):1595-8.
10. Hsueh Y, Shieh S. Two-stage retroauricular flap to reconstruct a helical rim defect. Dermatol Surg. 2009;35(11):1827-30.
11. Hénoux M, Espitalier F, Hamel A, Dréno B, Michel G, Malard O. Vascular supply of the auricle: anatomical study and applications to external ear reconstruction. Dermatol Surg. 2017;43(1):87-97.
12. Cerci FB. Retalho retroauricular estagiado para reconstrução de hélice após cirurgia micrográfica de Mohs. An Bras Dermatol. 2016;91(1):144-7.
13. Ramsey ML, Ellison CA, Al Aboud AM. Interpolated flaps. StatPearls. 2020[Internet]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470521/.
14. Pontes LT, Kimyai-Asadi A, Jih MH, Moraes AM, Stolf HO. Retalho de rotação para defeitos da asa. Surg Cosmet Dermatol. 2009;1(1):47-8.
15. Gadelha ADR, Costa IMC. Cirurgia dermatológica avançada: retalho de rotação. 3th ed. Rio de Janeiro: Atheneu; 2016.
16. Starkman SJ, Williams CT, Sherris DA. Flap basics I: rotation and transposition flaps. Facial Plast Surg Clin North Am. 2017;25(3):313-21.
17. Kim DP, Kus K, Ruiz E. Basal cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):13-24.
18. Tanese K. Diagnosis and management of basal cell carcinoma. Current Treat Opt Oncol. 2019;20(2):13.
19. Bariani RL, Nahas FX, Barbosa MVJ, Farah AB, Ferreira LM. Basal cell carcinoma: an updated epidemiological and therapeutically profile of an urban population. Acta Cir Bras. 2006;21(2):66-73.
20. 20-Aguilar EF. Ear reconstruction. Clin Plastic Surgery. 2004;31(1):87-91.
21. Iljin A, Antoszewski B, Durko M, Zieliński T, Pietruszewska W. External auditory meatus and/or conchal bowl reconstruction with postauricular island flap in patients with basal cell carcinoma or squamous cell carcinoma. Otolaryngol Pol. 2018;72 (3):4-10.
22. Li Y, Cui C, Zhang R, Zhang Q, Xu Z, Xu F, et al. Anatomical and histological evaluation of the retroauricular fascia flap for staged auricular reconstruction. Aesthet Plast Surg. 2018;42(3):625-32.
23. Johnson TM, Fader DJ. The staged retroauricular to auricular direct pedicle (interpolation) flap for helical ear reconstruction. J Am Acad Dermatol. 1997;37(6): 975-8.
24. Faleiros HRP. Retalho retroauricular em ilha a pedículo superior, estudo anatomico e novos conceitos. Botucatu: Faculdade de Medicina de Botucatu (UNESP). Dissertação de mestrado. 2003. Available from: https://repositorio.unesp.br/handle/11449/88965.
25. Cordova A, D'Arpa S, Pirrello R, Giambona C, Moschella F. Retroauricular skin: a flaps bank for ear reconstruction. J Plast Reconstr Aesthet Surg. 2008;61(1):S44-51.
26. Lo Piccolo MC. Rotation flaps-principles and locations. Dermatol Surg. 2015;41(10): S247-54.
27. Lo CH, Kimble FW. The ideal rotation flap: an experimental study. J Plast Reconstr Aesthet Surg. 2008;61(7):754-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}