


Eduardo de Oliveira Vieira1,2; Carlos Baptista Barcaui1,2; Elisa de Oliveira Barcaui1,2
Financial support: None
Conflict of interest: None
Submitted on: 28/04/2021
Approved on: 20/05/2021
How to cite this article: Vieira EO, Barcaui CB, Barcaui EO. Divided nevus in the genital region: report of six cases. Surg Cosmet Dermatol. 2021;13:20210038.
The divided nevi occur in contiguous areas of the skin that are mostly benign lesions. We report six cases of nevus divided on the penis and its dermoscopic patterns. Clinical follow-up was the best therapeutic option for this group of patients, considering the location of these lesions.
Keywords: Dermoscopy; Nevus; Intradermal nevus; Pigmented nevus; Penis
Divided nevus, also known as “kissing nevus”, result from opposite migrations of contiguous areas that that undergo embryonic cleavage, which can occur in the penis, labia minora or majora, and upper and lower eyelids – the latter is the most common location.1,2,3 Despite presenting different dermoscopic patterns, they are usually nevi with a benign evolution, and clinical follow-up is one of the possibilities for follow-up.4,5
We report six cases of divided nevus or “kissing nevus” located on the penis glans and foreskin in male patients, aged between 5 and 26 years, asymptomatic, and without prior treatment. We used clinical examination and dermoscopy with a DL3 3GEN dermatoscope with polarized light and ultrasonography gel as the interface liquid for diagnosis. Images were obtained with a Nikon Coolpix P6000 camera.
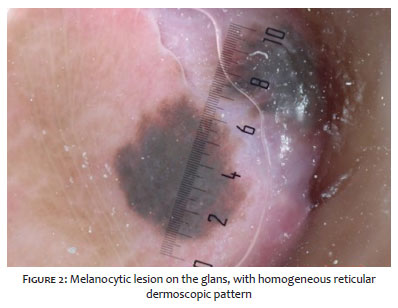
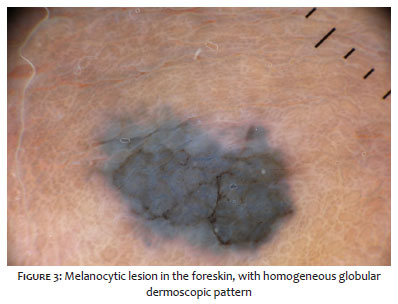
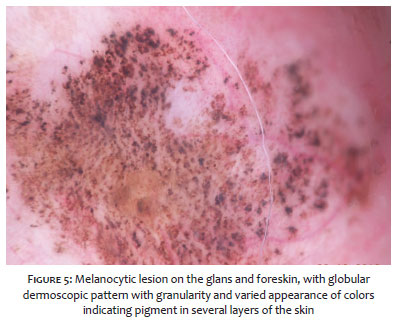
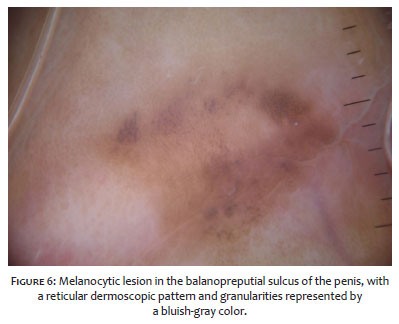
We observed the following dermoscopic patterns: homogeneous reticular (Figures 1 and 2), homogeneous globular (Figures 3 and 4), mixed (reticular-globular, with peripheral pigment network and central globules), and some cases presented granularity (Figures 5 and 6). Guided by the clinical examination and dermoscopy, we chose not to biopsy any patient and perform the follow-up every three months in the first semester, every six months in the second semester, and every year after that.
The migration of divided nevi occurs at different times during embryogenesis, depending on the site of origin. For the penis, the division occurs between the 11th and 14th gestational week, the external genitalia maturation period, and for the eyelid, around the 24th week.4,6 Some dermoscopic patterns have already been reported both in pediatric and in adults patients. Among them are the globular and reticular-globular, which presents a pigmented network in the periphery and globules in the center, in addition to the homogeneous pattern, which has some globules in the center – all suggestive of benignity.4,5
The low risk of malignant evolution is known. As far as we are aware, only three cases involving eyelids and penis have been reported to date.6,7,8
Considering that we found kissing nevus in glabrous and non-glabrous skin, as well as in mucosal and semi-mucosal areas, signs that lead to a clinical suspicion for malignancy should be sought. However, they are sometimes difficult to be assessed in these areas due to their multi-component pattern, containing different colors and structures, absence of structures, and blue-whitish veil.4,5 None of the patients presented signs suggestive of melanoma.
Among the therapeutic options available in the literature, the most indicated one given the benign lesions is the expectant management (watchful waiting), with clinical and dermoscopic follow-up. Surgical excision with mucosal and/or flap grafts, postectomy, and laser therapy (Nd:YAG, alexandrite, CO2) should be chosen, considering the patient’s functional and psychological aspects.4,5, 9,10 All patients are under clinical follow-up.
The follow-up of these lesions varies in the literature. There are reports of follow-ups every three, six, and 12 months. Some authors suggest a follow-up similar to that of congenital nevi, always considering the dermoscopic pattern of the lesion.4,5
Knowledge of the dermoscopic patterns of the divided nevus is essential for the proper follow-up of the patient and the biopsy indication, as the sites of onset of this lesion are not so simple to approach and can lead to esthetic, functional, and, mainly, psychological impairment.
Eduardo de Oliveira Vieira 0000-0001-6765-2474
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Carlos Baptista Barcaui 0000-0002-3303-3656
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Elisa de Oliveira Barcaui 0000-0002-9487-7860
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Jiang S, Chen Y, Hinchliffe TE, Wu T, Stephen T. Kissing nevus of the penis. J Coll Physicians Surg Pak. 2018;28(3):S19-S20.
2. Vora RV, Shah AJ, Patel TB. Congenital melanocytic kissing nevus on right eyelid: a rare phenomenon. Indian Dermatol Online J. 2020;11(4):627-8.
3. Lysebo DE, Krohn J. Kissing naevus. Tidsskr Nor Laegeforen. 2021;7(1):141.
4. Armengot-Carbó M, Rodrigo-Nicolás B, Botella-Estrada R. Divided or kissing nevus of the penis: a new case with dermoscopic findings. Pediatr Dermatol. 2018;35(5):e321-e4.
5. Godinho N, Nai GA, Schaefer ALF, Schaefer LV. Kissing nevus of the penis: a case report and dermatoscopic findings. An Bras Dermatol. 2017;92(5 Suppl 1):95-7.
6. Kharel Sitaula R, Batta S, Shrestha GB, Shrestha JK. Malignant transformation of kissing nevus- a rare entity. Nepal J Ophthalmol. 2012;4(2):329-32.
7. Fuchs A. Divided nevi of the eyelids. Urol Cutaneous Rev. 1950;54(2):88-90.
8. Lemaître S, Gardrat S, Vincent-Salomon A, Galatoire O, Lévy-Gabriel C, Desjardins L. Malignant transformation of a multi-operated divided nevus of the eyelids. Ocul Oncol Pathol. 2018;4(2):112-5.
9. Correia B, Duarte AF, Haneke E, Correia O. CO2 laser treatment of a kissing nevus of the penis: an alternative solution for a rare condition. J Dermatolog Treat. 2021;32(1):120-3.
10. Bray FN, Shah V, Nouri K. Laser treatment of congenital melanocytic nevi: a review of the literature. Lasers Med Sci. 2016;31(1):197-204.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}