


Leticia Dupont; Daniele Damares Rodrigues de Souza; Ana Paula Dornelles Manzoni
Financial support: None
Conflict of interest: None
How to cite this article: Dupont L, Souza DDR, Manzoni APD. Myomodulation with hyaluronic acid for correction of gummy smile. Surg Cosmetic Dermatol. 2021;13:e20210032.
The "gummy smile" occurs when more than 3-4 mm of gingiva appears during the act of smiling. It is considered unattractive and causes aesthetic disharmony. It has a multifactorial etiology, with several techniques described for its correction. Myomodulation with hyaluronic acid is a non-surgical alternative with immediate and lasting results. In this article, we present a case of myomodulation with hyaluronic acid to correct "gummy smile" in a 31-year-old patient.
Keywords: Hyaluronic acid; Gingiva; Smile
The discomfort caused by the excessive gingival display, or a “gummy smile”, is an increasingly common complaint in dermatology practice. The choice of therapeutic approach must rely on a detailed analysis of the underlying factors.1 Botulinum toxin is the most popular intervention. However, in some cases, the limitations on the natural movement of the facial muscles cause patient discomfort.2 In these situations, myomodulation with hyaluronic acid (HA) is an effective alternative that yields immediate and longer-lasting results.2,3
This article presents a detailed video analysis of the case of a 31-year-old woman with a gummy smile treated with myomodulation of the involved muscles.
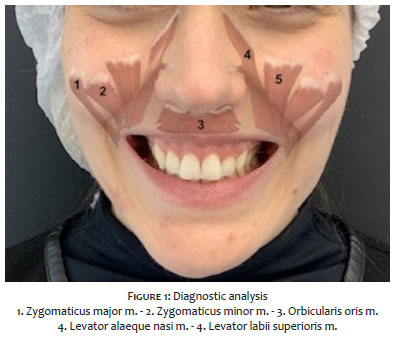
Diagnostic assessment: (Figure 1)
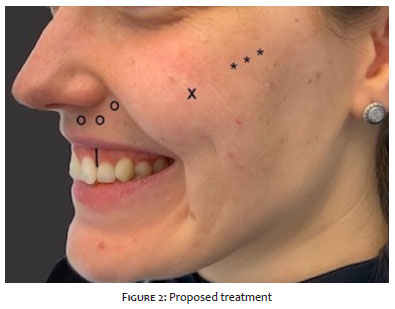
Figure 1 analysis shows a gummy smile with an anterior pattern due to hyperactivity of the levator labii superioris/alaeque nasi muscles.3 Conversely, when the facial muscles are at rest, the corner of the mouth is projected downwards, creating a sullen expression (“sad mouth”). The descended mouth corner causes in this patient are a hyperactive depressor anguli oris muscle, ptosis of the zygomatic retaining ligaments (the attachment points of the main elevation muscles of the mouth, i.e., the zygomaticus major and minor), and deflation of the lateral suborbicularis orbiculi fat (SOOF), which acts as a pulley to facilitate the lifting action of these muscles.4 There is also some hyperactivity of the depressor septi nasi muscle, as seen in Figure 2.
1. Supraperiosteal and infrazygomatic lifting and anchoring (using the lift technique5) and replacement of SOOF volume to increase the contractile power of the zygomatic muscles and facilitate mouth corner elevation.
2. Reduction of muscle hyperactivity through deposition of hyaluronic acid over the levator labii superioris alaeque nasi and levator labii superioris muscles. We used the same technique to decrease hyperactivity of the depressor septi nasi and correct ptosis of the nasal tip while smiling.
3. Myomodulation of the depressor anguli oris muscles will be performed at a later date.

1. Lidocaine 2% with vasoconstrictor is infiltrated into the infrazygomatic region with subsequent puncture using a 21G needle to introduce the cannula;
2. Lifting and anchoring of the zygomatic retaining ligament (using the lift technique5) with a 22G rigid cannula and supraperiosteal deposition of three 0.1 mL boluses of high G prime HA on each side. Then, the cannula is placed in the SOOF, and 0.2 mL of HA is deposited on each side, totaling 1 ml of filler.
3. The cannula is oriented toward the ala nasi through the superficial fat pads into the same puncture site.
4. The cannula traverses the nasolabial ligament and reaches the pyriform aperture.
5. Intermediate G prime HA was deposited over the levator labii superioris and depressor septi nasi to create a mechanical barrier to their hyperactivity. The volume deposited was 0.3 mL on each side. The filler was infiltrated slowly in microbolus increments of no more than 0.05 mL, to reduce the risk of extrinsic vascular compression. Aspiration of the cannula was always performed before HA deposition.
CAUTION: It is of paramount importance to note that the region of the pyriform aperture is considered to be at high risk of arterial occlusion due to its proximity to the angular artery. We suggest that applications in this region be performed with a 22G cannula, with 8 seconds of aspiration before each slow infiltration of a microbolus (maximum volume 0.05 mL).
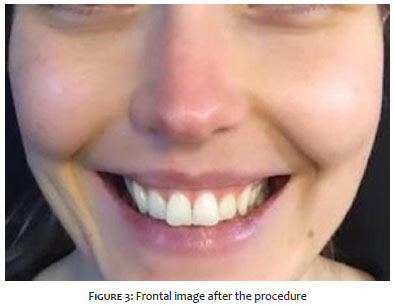
6. Immediately after the procedure, there is a noticeable reduction of the gingival display, the elevation of the mouth corners, and improvement of ptosis of the nasal tip while smiling (Figures 3 and 4).
Knowledge of anatomical structures and the development of hyaluronic acid-based myomodulation techniques have increased the precision and optimized the outcomes of dermal filler procedures. We believe HA should be considered for correcting the gummy smile in cases where botulinum toxin has yielded unsatisfactory results and when the patient is searching for an immediate, longer-lasting effect.
Leticia Dupont 0000-0002-8150-1055
Study design and planning; preparation and writing of the manuscript; critical literature review.
Daniele Damares Rodrigues de Souza 0000-0003-0610-4807
Data collection, analysis and interpretation; preparation and writing of the manuscript; critical literature review.
Ana Paula Dornelles Manzoni 0000-0001-6184-4440
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Dym H, Pierre R 2nd. Diagnosis and treatment aproaches to a "Gummy Smile". Dent Clin N Am. 2019;64(2):341-9.
2. Diaspro A, Cavallini M, Sito G, Patrizia P. Gummy smile treatment: proposal for a novel corrective technique and a review of the literature. Aesthet Surg J. 2018;38(12):1330-8.
3. Hsien-Li Peng P, Peng JH. Treating the gummy smile with hyaluronic acid filler injection. Dermatol Surg. 2019;45(3):478-80.
4. Maio M. Myomodulation with injectable fillers: an innovative approach to addressing facial muscle movement. Aesth Plast Surg. 2018;42(3):798-814.
5. Manzoni APD, Sena D. Lift technique with hyaluronic acid. Dermatol Surg. 2021;47(5):741-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}