


Khairuddin Djawad; Idrianti Idrus; Airin Nurdin Mappewali
Submitted on: 12/01/2021
Approved on: 14/02/2021
Financial support: None
Conflict of interest: None
How to cite this article: Djawad K, Idrus I, Mappewali NA. Closure of a large nasal dorsum defect using a bilateral crescent advancement flap from the malar region to the nose. Surg Cosmet Dermatol. 2021;13:e20210017
The closure of large defects on the nasal dorsum is a challenge for dermatologic surgeons. The alternatives to repair the defect are a skin graft and some forms of skin flaps. One particular defect closure technique is the crescentic advancement flap, which uses crescent incisions at the nasolabial fold to accommodate the excess tissue. This flap is best used if the defect is in the lateral nose, alar, and nasolabial fold. We report a large defect of the nasal dorsum in a 65-year-old woman that was successfully reconstructed using bilateral cheek-to-nose crescentic advancement flap. The patient showed excellent cosmetic and outcome.
Keywords: Dermatology; Nasal Bone; Surgical Flaps
The crescentic perialar flap was firstly introduced in 1955 to repair defects of the upper lip. The principle of this flap is to remove redundant tissue in a crescentic form to allow lateral movement that is then followed by the advancement flap to cover the defect. It is a variation of a unilateral advancement flap.1 The benefit of this flap is facilitating defect closure with minimal tissue distortion and, when properly executed, facial symmetry, superior cosmetic results, and a minimal scar can be achieved.2 The use of a crescentic flap is useful for defects on the lip, nasal ala, nasolabial fold, nasal dorsum, sidewall, nasofacial fold, and along the lateral forehead.2,3 Although the skin contour of the nasal sidewall and cheek are similar, the nasofacial fold that unites these two cosmetic subunits needs to be maintained to achieve optimal aesthetic consideration.
We report a case of a large BCC defect on the dorsal nasal that extended to the sidewall.
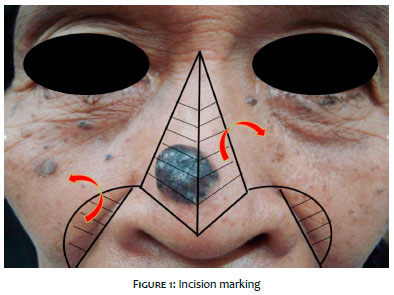
A 65-year-old woman presented with a 2.5 cm defect on the nasal dorsum, which extended to the lateral sidewalls resulting from BCC removal. Histopathological examination confirmed that all margins had been free of tumor. The design of the flap was done before local anesthesia with bilevel anesthesia based on the technique by Prof. Lawrence Field.4 After complete local anesthesia was achieved, an incision was conducted in a juxtaposed triangle-like incision according to the previously drawn marks (Figure 1). Marking was critical to avoid distorting the anatomical landmarks resulting from anesthesia infiltration. Removal of the skin superior to the defect was required to avoid dog-ear formation.
The incision was done bilaterally from the inferomedial sides of the triangle base with a length three times the distance between the medial edge to the midline and extended inferiorly along the alar crease and sulcus to the nasolabial fold (Figure 2).5 The length of the incision was three times the length from the medial edge to the midline.6 Subcutaneous blunt dissection at the superficial muscular aponeurotic level was done on the lateral cheek to facilitate approximation and reduce stress on the medial edge. We performed a trial advancement flap to estimate the amount of tissue needed to be incised to make the crescentic incision (Figure 3).2 A crescentic excision was then carefully done to ensure symmetry of the nasolabial fold. Excessive excision may cause elevation of alar, whereas too little excision may cause depression. Both flaps were elevated above the nose and medially advanced from cheeks to the nose, forming a bilateral cheek-to-nose crescentic advancement flap.3 The primary defect was suture with the largest diameter suture.6 The defect was sutured on both sides along the midline, alar crease, and nasolabial fold (Figure 4). Each flap was sutured to the periosteum at the nasofascial sulcus which functioned to maintain the contour of the alar crease sulcus and nasal sidewall.7 Hemostasis was maintained throughout the procedure to aid intraoperative visualization and avoid post-operative bleeding. Wound edges were closed with a 5.0 monofilament suture.
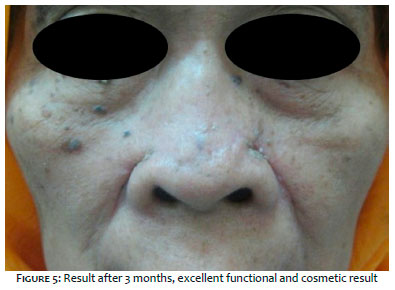
The patient showed excellent cosmetic and functional recovery after three months (Figure 5).
Closure of defects on the nasal dorsum or sidewall with a size of more than 2 cm often has only limited options; some
possible approaches include dorsal nasal rotation flap, birhombic flap, Rintala flap, Peng flap, a two-staged paramedian forehead flap, and fUll-thickness skin graft (FTSG). However, the cosmetic result of grafts will not be optimal if they are not placed within the same cosmetic subunits. A paramedian forehead flap required at least 2 stages and, given the different thicknesses of skin on the forehead and nasal dorsum or sidewall, has a potential risk of tissue mismatch.7
A bilateral crescentic advancement flap should be considered for large defects of the nose. The success of this flap depends on the laxity of the surrounding skin because tension on the wound edge may cause ischemia and necrosis. The crescentic flap is a modification of Burrow’s advancement flap,6 where a crescent-shaped excision, instead of a triangle, is used to correct any tissue redundancy that occurred. The sutures were then tacked on the alar crease or nasolabial line.5 The ideal defect locations for this technique are the nasofacial sulcus and lateral alar crease. Putting sutures in these natural anatomic lines allows optimal concealment of the scar. Defects that cross the nasolabial fold can cause aesthetic deformity of the natural nasolabial boundary; patients with prominent nasolabial fold can even develop bridging after the closure of the defect. Furthermore, defects located inferior to the nasolabial fold can potentially cause lip retraction and asymmetry of the nasolabial fold. Thus, both sides of the flap were sutured to periosteum at the nasofascial sulcus to maintain the contour of the alar crease sulcus and nasofacial sulcus.7 In addition, the medial suture was made directly on the nasal midline to camouflage the suture.
The bilateral crescentic advancement flap is a good option to repair larger defect of nasal dorsum with a large height-to-width ratio or defects with curved borders.1 Thus, this technique is suitable for defects above the nasal supratip with a relative midline location, nasal dorsum, and nasal sidewall. This single-stage bilateral cheek-to-nose crescentic advancement flap was advantageous in avoiding the morbidity often associated with multistage repairs and preserve facial symmetry.8 The use of bilateral cheek-to-nose crescentic advancement flap has been reported in a case of a large symmetric defect on the nasal dorsum.5 This technique was also successfully used in an asymmetric lesion above the nasal supratip by placing incision lines on the junction between the nasal supratip and alar crease cosmetic subunits.9
In this case, we successfully conducted reconstructed a large defect on the nasal dorsum with satisfying cosmetic, functional results, and without any significant complications. Factors that played a central role in the successful reconstruction of this case were dog-ear excision at the superior of the defect, properly executed crescentic incision on both nasolabial folds, key suture to the periosteum in the nasofascial sulcus, and placing the sutures on the nasal midline.
Khairuddin Djawad 0000-0002-4569-6385
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Idrianti Idrus 0000-0003-2868-6289
Study design and planning, intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Airin Nurdin Mappewali 0000-0001-6122-4866
approval of the final version of the manuscript; critical literature review.
1. Kruter L, Rohrer T. Advancement flaps. Dermatol Surg. 2015;41 (Suppl 10):S239-S46.
2. Mellette Jr JR, Harrington AC. Applications of the crescentic advancement flap. J Dermatol Surg Oncol. 1991;17(5):447-54.
3. Goldman G, Dzubow L, Yelverton C. Facial Flap Surgery. New York: Mc Graw Hill; 2012.
4. Howe NM, Chen DL, Holmes TE. Crescentic Modification to Island Pedicle Rotation Flaps for Defects of the Distal Nose. Dermatologic Surgery. 2019;45(9):1163-70.
5. Holmes TE. Crescentic apical triangle island pedicle flap for repair of the medial upper lip. Dermatologic Surgery. 2013;39(5):784-8.
6. Field LM. Bilevel anesthesia and blunt dissection: rapid and safe surgery. Dermatologic surgery. 2001;27(11):989-91.
7. Nakhla TN, Horowitz MK, Schwartz RM. Malar butterfly flap: Bilateral me-lolabial advancement for large dorsal nasal defects. Dermatologic surgery. 2009;35(2):253-6.
8. Yoo SS, Miller SJ. The crescentic advancement flap revisited. Dermatologic surgery. 2003;29(8):856-8.
9. mith JM, Orseth ML, Nijhawan RI. Reconstruction of Large Nasal Dorsum Defects. Dermatologic Surgery. 2018;44(12):1607-10.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}