


Paula Hitomi Sakiyama; Thiago Augusto Ferrari; Raíssa Rigo Garbin; Alexandre Luiz Weber
Submitted on: 10/09/2020
Final decision: 04/03/2021
Financial support: none
Conflit of interest: none
How to cite this article: Sakiyama PH, Ferrari TA, Garbin RR, Weber AL. Reconstruction of a full-thickness alar defect using a nasolabial flap combined with hinge flap. Surg Cosmet Dermatol. 2021;13:e20210004.
The nasal region is a frequent site of keratinocyte carcinomas. Its peculiar anatomy, contour, and three-dimensionality make surgical repair challenging. Eventually, in situations of greater complexity, a single technique may not be sufficient to restore the original anatomy, requiring the association of methods. This article describes a strategy for reconstructing a full-thickness alar defect, including the nasal margin, based on the combination of a nasolabial transposition flap with a hinge flap. It is a safe procedure, dependent on the mobilization of local tissue and performed in a single surgical procedure.
Keywords: Surgical flaps. Nose neoplasms. Skin neoplasms. Mohs surgery. Carcinoma, basal cell
The nasal region is a frequent site of keratinocyte carcinomas. The nose’s peculiar anatomy, contour, and three-dimensionality make surgical repair a challenge. The treatment aims to achieve the oncological cure with maximum functional preservation and good aesthetic result since unsightly scars and post-operative deformities can cause psychological impact. The choice of the method for closing the surgical defect will depend on its size and location. Occasionally, in complex scenarios, associating techniques may be necessary to restore the original anatomy.1,2 In this article, we report the single-stage reconstruction of a full-thickness nasal alar defect, including the nasal margin, combining two techniques: the nasolabial transposition flap and the hinge flap.
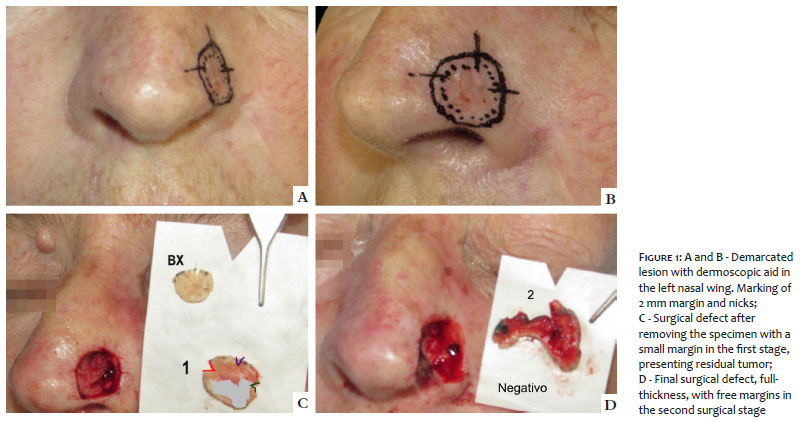
A 61-year-old woman presented an erythematous plaque, depressed, poorly defined, and infiltrated in the left nasal wing, measuring 0.5 cm x 0.5 cm. The lesion was adjacent to a scar resulting from surgery to remove basal cell carcinoma (BCC), unspecified subtype, in the nasal wing 14 years earlier, approached by conventional technique with bilobed flap closure. Histopathological examination, obtained by incisional biopsy, showed infiltrative BCC with associated perineural invasion. Considering the possibility it was a recurrence, in addition to the aggressive histological subtype, perineural invasion, and high-risk location, we chose the treatment according to the Mohs micrographic surgery (MMS) technique.
The lesion was submitted to MMS, under local anesthesia, with free surgical margins in the second stage, resulting in a full-thickness surgical defect in the left nasal wing, including the nasal margin (Figure 1). Given the complexity and dimensions of the defect, we repaired the lesion combining two techniques: the nasolabial transposition flap, to recompose the nasal roof, and the hinge flap, to reconstruct the nasal floor. For the hinge flap, the Burow triangle provided the “dog ear”, formed during the execution of the nasolabial transposition flap. This triangle was incised superiorly to the defect, preserving a deep pedicle in its distal portion. The area that would be neglected was de-epithelialized, and the pedicle was folded back to form the nasal lining. Then, the nasolabial transposition flap was incised according to the usual technique and positioned over the hinge flap, creating the external coverage of the nasal wing. On the nasal margin, both flaps were sutured edge-to-edge (Figure 2).
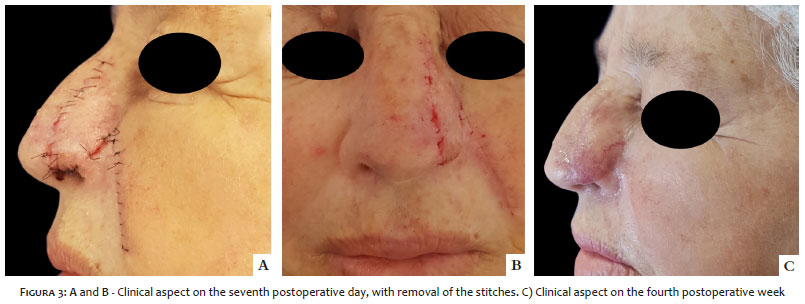
The patient presented a good postoperative evolution, with satisfactory outcomes from the functional and aesthetic perspectives (Figure 3).
High-risk keratinocyte tumors, as described in the case, are ideally addressed by MMS. The method allows an assessment of the surgical margins close to 100%, showing higher cure rates and lower recurrence rates when compared to the conventional technique, which uses sample analysis. Also, it provides the preservation of healthy tissue, an essential factor in approaching noble areas.3,4 However, even when achieving maximum tissue conservation, reconstruction of the nasal region remains challenging. It becomes even more complicated in extensive or complex cases, such as the one reported, where the tumor excision resulted in a full-thickness defect in the nasal wing involving the nasal margin.
Repair of full-thickness nasal defects should include remaking of skin coverage, inner lining, and structural support as needed.5,6 Failure to provide adequate mucosal support in more significant defects can lead to scar contraction and/or flaws in overlapping flaps or grafts structure, making this step the most critical of the procedure.
Currently, the literature describes several techniques to repair minor defects involving the mucosa, such as the hinge flap, frontal paramedian flap (FPF), full-thickness skin graft (FTSG), and bipedicled vestibular advancement flap. In cases of more extensive involvement, FPF, FTSG with an overlapping FPF, or intranasal flaps (septal mucoperichondrial hinge flap, composite septal chondromucosal flap) are alternatives. Intranasal flaps must be performed under sedation or general anesthesia. However, the other options mentioned can be successfully implemented under local anesthesia in selected cases.7
Most procedures include cartilage graft to allow tissue support and prevent nasal valve movement during inspiration. Nevertheless, its use is not mandatory, as in the case used in this report. The hinge flap, with its distal portion sutured to the remaining tissues and folded against the transposition flap to make the nasal fold, promotes an adequate tent effect, allowing free air passage through the nostrils. The tissue layout, forming a “sandwich” by combining the hinge flap with the nasolabial transposition flap to cover the skin, promoted adequate structural rigidity, preventing its collapse during inspiration.8,9
Spear et al. described a flap option in 1987, and more recently, Cook published it in detail, which allows reconstruction without cartilage graft. Although it was initially described as a one-time reconstruction, it may require a second surgery for refinement due to tissue thickness that compromises aesthetics and also affects functionality, as narrowing of the nostril impairs breathing.8,1
It is essential to emphasize that the hinge flap technique requires a meticulous examination of the donor area. The region must have the least possible actinic damage to avoid neoplasm development in the future since, when being hit to form the nasal floor, it will occupy a complex place to assess and follow-up. Also, it is fundamental to ensure that the margins do not present residual neoplasia not to transfer tumor tissue into the nasal cavity.5 The approach using the MMS technique, as in the case described, is more likely to achieve this result.
We believe that the reported flap combination offers advantages over other available surgical techniques, including execution in a single surgical procedure, performance under local anesthesia, lower risk of necrosis than skin graft, less bleeding than flaps from the nasal cavity, and relative skin preservation. It saves the tissue reservoir of the forehead, which would be used in the FPF.
The combination of the nasolabial transposition flap and the hinge flap represents a good option for reconstructing full-thickness alar defects, including those affecting the nasal margin, with satisfactory aesthetic and functional outcomes. It is a safe method, dependent on the mobilization of local tissue for its execution, and performed in a single surgical time, thus reducing the costs and morbidity inherent to additional procedures.
Paula Hitomi Sakiyama | 0000-0001-7813-8294
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Thiago Augusto Ferrari | 0000-0003-4874-4837
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Raíssa Rigo Garbin | 0000-0002-9771-1209
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Alexandre Luiz Weber | 0000-0002-4862-5777
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Joseph AW, Truesdale C, Baker SR. Reconstruction of the Nose. Clin North Am. 2020;27(1):43-54.
2. Cerci FB, Kubo E. Reconstrução nasal após cirurgia micrográfica de Mohs: análise de 208 casos. Surg Cosmet Dermatol. 2020;12(1):42-50.
3. Cernea SS, Gontijo G, Pimentel ERA, Tarlé RG, Tassara G, Ferreira JASLB, et al. Diretrizes de indicações de cirurgia micrográfica de Mohs nos tumores da pele. An Bras Dermatol. 2016;91(5):621-7.
4. Tolkachjov SN, Brodland DG, Coldiron BM, Fazio MJ, Hruza GJ, Roenigk RK, et al. Understanding Mohs micrographic surgery: a review and practical guide for the nondermatologist. Mayo Clin Proc. 2017;92(8):1261-71.
5. Taeda A, Akimoto M, Park K, Kounoike N, Shimakura Y, Nemoto M, et al. Single- stage reconstruction of a full-thickness alar defect using a folded nasolabial flap combined with a redundant skin turnover flap. J Craniofac Surg. 2014;25(6):2144-6.
6. Bedwani NH, Rizkalla M. Single-stage reconstruction of full-thickness nasal alar defect using bilobed and turnover flaps. J Craniofac Sugr. 2020;31(2):e169-71.
7. Cerci FB, Dellatorre G. Retalho paramediano frontal associado a retalho em dobradiça para reparo de defeito em ponta nasal. An Bras Dermatol. 2016;91(5 Supl 1):S140-3.
8. Sanchez FH, Estefan JL, Fernandez ID. Reconstrução completa de asa nasal com retalho de Spear após cirurgia micrográfica de Mohs no tratamento de carcinoma basocelular. Surg Cosmet Dermatol 2013;5(4):3559.
9. Sanchez FH, Estefan JL, Fernandez ID. Reconstrução nasal complexa com combinação de retalhos bilaterais em dobradiça e retalho paramediano frontal, após cirurgia de Mohs. Surg Cosmet Dermatol 2013;5(4):355-9.
10. Lane JE, Hsia LB, Merritt BG. Reconstruction of large transmural nasal defects with a nasolabial turnover interpolation flap. Dermatol Surg. 2020;46(7):899-903.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}