


Marina Landau1; Erica M Lin2; Carlos Wambier2
Receipt date: 28/03/2020
Approval date: 29/05/2020
Financial Support: None
Conflict of Interest: None
Institution: Arena Dermatology, Herzliya, Tel Aviv, Israel
Filler-induced arterial obstruction can mimic other dermatological conditions. In this case series, the authors describe four patients with filler-induced arterial obstruction presenting with pustular rash that was misdiagnosed as a herpetic infection. Since correct and timely diagnosis is crucial for scar prevention, pustular rash has to be recognized by injectors as a clinical expression of vascular obstruction induced by dermal filler injection.
Keywords: Hyaluronic acid; Herpes simplex; Ischemia; Injections, intra-arterial
Hyaluronic acid (HA) filler injections are popular minimally invasive procedures performed on healthy individuals looking for cosmetic enhancement.1 Vascular compromise followed by skin necrosis is a devastating potential complication.2-6 Early recognition of vascular occlusion and proper treatment, including hyaluronidase injection, are required to avoid irreversible changes such as scarring.6-11 However, symptoms of vascular occlusion are occasionally misinterpreted. In such circumstances, treatment is delayed, significantly reducing the chances of full recovery.
Clinical presentation of dermal ischemia includes skin blanching, livedo reticularis, redness, skin sloughing, crusting, and scars. Pustules are only rarely mentioned as a manifestation of impending skin necrosis.3,12 In the past year, we evaluated four cases in which patients presented with a pustular eruption 3-4 days after HA-based dermal filler injection. In all cases, the injecting/treating physician made the diagnosis of a herpetic outbreak. Detailed medical history indicated that the pustules resulted from impending skin necrosis due to filler-induced vascular occlusion rather than viral infection.
Case 1
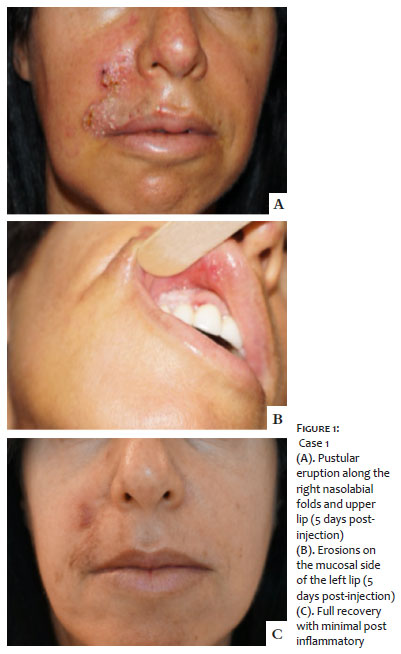
A 44-year-old woman presented for a consultation five days after being injected for upper lips wrinkles with HA-based filler elsewhere. Twenty-four hours after injection, she complained of pain accompanied by skin discoloration along the right nasolabial fold and upper lip. Her complaint was dismissed as a simple bruise. On the third day after the injection, a pustular eruption developed in the same area. The injecting physician examined the patient and clinically diagnosed the eruption as a herpetic outbreak, initiating the systemic anti-herpetic treatment. When we examined the patient in our office, a confluent pustular eruption along the right nasolabial with focal crusts was present (Figure 1a). Widespread erosions were evident on the mucosal side of the left lip (Figure 1b).
Based on the patient’s history and clinical findings, diagnosis of impending skin necrosis due to intraarterial injection of HA was made. Bacterial and viral cultures were taken and came back negative. The patient was treated with 300 units hyaluronidase in the affected area, topical 2% Nitroglycerin cream, 100 mg Aspirin, and antibiotic ointment. After re-epithelization, we performed three sessions of vascular laser treatment (VBeam by Syneron Candella). Following the treatment, full skin recovery was achieved with minimal post-inflammatory hyperpigmentation at the site (Figure 1c).
Case 2
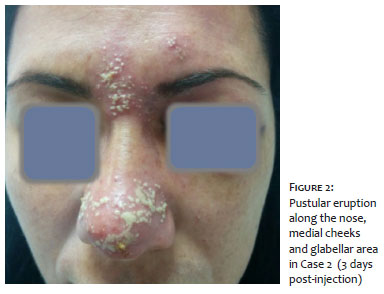
A 32-year-old woman was injected elsewhere with HA-based filler for nose enhancement. Twenty-four hours after the injection, the patient experienced severe pain accompanied by skin discoloration. The treating physician’s office staff dismissed these complaints as a normal post-procedural effect. On the third day after the injection, the patient was seen in a hospital emergency room with a pustular eruption, and we were tele-consulted. At this stage, erythema and swelling of the nose, medial cheeks, and glabellar area, along with pustules on the distal and proximal parts of the nose, were observed (Figure 2). The diagnosis of impending skin necrosis due to intravascular obstruction was made. Nevertheless, the patient was admitted to the hospital, and intravenous antibiotic and antiherpetic treatment were initiated. The patient was lost to follow-up.
Case 3
A 53-year-old woman was examined in our office three days after a HA-based filler injection for upper lip wrinkles elsewhere. Skin discoloration was noted 24 hours post-injection and photographed by the patient (Figure 3a). On the third day post-injection, a pustular eruption appeared, and the patient contacted the treating physician’s office. A diagnosis of Herpes simplex was made, and treatment with systemic antiherpetic was initiated.
At this stage, we examined the patient in our office. On examination, we observed erythema and swelling of the upper lip and left lower nasolabial areas. Pustules were seen in two distinct foci on the upper lip (Figure 3b). Painful erosion was found on the upper left lip mucosa (Figure 3c). The diagnosis of impending skin necrosis due to intravascular filler injection was made. The patient was treated with 300 units of hyaluronidase, topical 2% Nitroglycerin cream, and topical anesthetic gel on the mucosal aspect to alleviate the pain. After an additional seven days, the mucosal erosions had healed completely, but residual crusting of the upper lip skin was still visible (Figure 3d).
Case 4
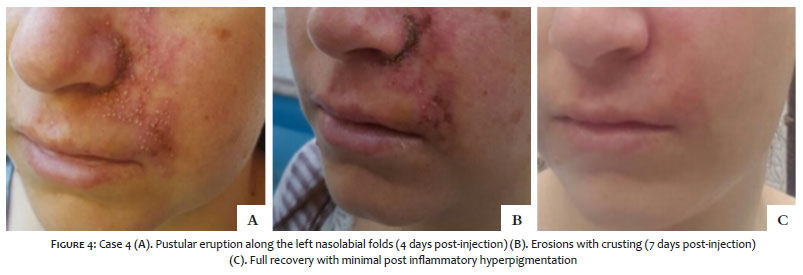
A 23-year-old woman was injected with HA-based filler into the nasolabial folds elsewhere. On the fourth day post-injection, the patient developed a pustular rash along the left nasolabial fold, nostril, and medial cheek (Figure 4a). After an additional three days, some of the pustules began to crust (Figure 4b). At this stage, the treating physician contacted our office for advice regarding systemic antiherpetic treatment. A diagnosis of intravascular HA injection was made. The patient was treated with a hyaluronidase injection into the affected area. Two weeks later, the treating physician reported that the skin had completely healed (Figure 4c).
Intra-arterial injection of dermal filler is rare, but not completely preventable. Slow injection of small boluses, thorough knowledge of regional anatomy, use of blunt cannulas instead of sharp needles, and pre-injection aspiration can all reduce the risk of arterial obstruction, but not completely eliminate its occurrence.12-15 Therefore, diagnosing this condition based on clinical manifestations and providing timely treatment are crucial in preventing devastating outcomes, such as scarring, and skin and soft tissue necrosis.12,16
While increasing pain and cutaneous discoloration are well known clinical signs, the pustular rash is a less well-recognized manifestation of vascular obstruction. As a result, misdiagnosis of pustular rash as herpes simplex infection delays proper management. The mechanism of pustular rash is potentially related to polymorphonuclear cell attraction to the site via complement activation during ischemic or thrombotic events, as reported in other tissues.17-19
The “golden time” for the first intervention is classically limited to the first three days after an ischemic event.20 According to our experience and the cases presented, the pustular phase is included within this “tissue saving” time frame.
Every injector should recognize the pustular phase as a part of the full clinical spectrum of filler-induced arterial obstruction to provide timely treatment.
Marina Landau | 0000-0001-9016-6394
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Erica M Lin | 0000-0002-7641-6040
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Carlos Wambier2 | 0000-0002-4636-4489
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. The American Society for Aesthetic Plastic Surgery. 2016 Cosmetic Surgery National Data Bank Statistics. [Internet]. New York: ASAPS Communications Office; [updated 2016; cited December 2019]. Available from: https://www.surgery.org/sites/default/files/ASAPS-Stats2016.pdf.
2. Kassir R, Kolluru A, Kassir M. Extensive necrosis after injection of hyaluronic acid filler: case report and review of the literature. J Cosmet Dermatol. 2011;10(3):224-231.
3. Beleznay K, Humphrey S, Carruthers JSA, Carruthers A. Vascular compromise from soft tissue augmentation. experience with 12 cases and recommendations for optimal outcomes. J Clin Aesth Dermatol. 2014;7(9):37-43.
4. Sun ZS, Zhu GZ, Wang HB, Xu X, Cai B, Zeng L, et al. Clinical outcomes of impending nasal skin necrosis related to nose and nasolabial fold augmentation with hyaluronic acid fillers. Plast Reconstr Surg. 2015;136(4):434e-441e.
5. Bravo BSF, Balassiano LKDA, Da Rocha CRM, Padilha CBDS, Torrado CM, Da Silva RT, et al. Delayed-type necrosis after soft-tissue augmentation with hyaluronic acid complication. J Clin Aesthet Dermatol. 2015;8(12):42-7.
6. Chen Q, Liu Y, Fan D. Serious vascular complications after nonsurgical rhinoplasty: a case report. Plast Reconstr Surg Glob Open. 2016;4(4):e683.
7. Glaich AS, Cohen JL, Goldberg LH. Injection necrosis of the glabella: Protocol for prevention and treatment after use of dermal fillers. Dermatol Surg. 2006;32(2):276-81.
8. Beer K, Downie J, Beer J. A treatment protocol for vascular occlusion from particulate soft tissue augmentation. J Clin Aesthet Dermatol. 2012;5(5):44-7.
9. Dayan H, Arkins JP, Mathison CC. Management of impending necrosis associated with soft tissue filler injections. J Drugs Dermatol. 2011;10(9):1007-12.
10. Abduljabbar MH, Basendwh MA. Complications of hyaluronic acid fillers and their managements. J Dermatol and Dermatol Surg. 2016;20(2):100-6.
11. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G, et al. Global Aesthetics Consensus: Avoidance and Management of Complications from Hyaluronic Acid Fillers-Evidence- and Opinion-Based Review and Consensus Recommendations. Plast Reconstr Surg. 2016;137(6):961e-71e.
12. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600.
13. Breithaupt AD, Jones DH, Braz A, Narins R, Weinkle S. Anatomical basis for safe and effective volumization of the temple. Dermatol Surg. 2015;41(Suppl 1):S278-83.
14. Sundaram H, Weinkle S, Pozner J, Dewandre L. Blunt-tipped microcannulas for the injection of soft tissue fillers: a consensus panel assessment and recommendations. J Drugs Dermatol. 2012;11(8):s33-39.
15. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Invest Dermatol. 2013;6:295-316.
16. Gilbert E, Hui A, Meehan S, Waldorf HA. The basic science of dermal fillers: past and present Part II: adverse effects. J. Drugs Dermatol. 2012;11(9):1069-77.
17. Tuttolomondo A, Di Sciacca R, Di Raimondo D, Renda C, Pinto A, Licata G. Inflammation as a therapeutic target in acute ischemic stroke treatment. Curr Top Med Chem. 2009;9(14):1240-60.
18. Distelmaier K, Adlbrecht C, Jakowitsch J, Winkler S, Dunkler D, Gerner C, et al. Local complement activation triggers neutrophil recruitment to the site of thrombus formation in acute myocardial infarction. Thromb Haemost. 2009;102(3):564-72.
19. Behm CZ, Kaufmann BA, Carr C, Lankford M, Sanders JM, Rose CE, et al. Molecular imaging of endothelial vascular cell adhesion molecule-1 expression and inflammatory cell recruitment during vasculogenesis and ischemia-mediated arteriogenesis. Circulation. 2008;117(22):2902-11.
20. Hong JY, Seok J, Ahn GR, Jang YJ, Li K, Kim BJ. Impending skin necrosis after dermal filler injection: A "golden time" for first-aid intervention. Dermatol Ther. 2017;30(2):e12440.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}