


Carlos Augusto Zanardini Pereira1; Ivo Acir Chermicoski2; Valéria Zanela Franzon3; Karina Hubner4; Miguel Olímpio Anastácio Junior5; Ionam Carlos Benazzi5
Introduction: Cryosurgery is a safe and effective treatment modality that uses liquid nitrogen for tissue destruction.
Objective: To demonstrate the effectiveness of cryosurgery in the treatment of hypertrophic granulation tissue in cutaneous wounds.
Methods: Cutaneous wounds with hypertrophic granulation tissue were treated with the nitrogen spray applied from a distance of 5cm from the area to be treated, at a 90º angle. The freezing time was two 5-second cycles and the number of sessions ranged from 1 to 3. The assessments of results were based on weekly clinical and photographic comparisons, as well on the measurement of the wound's and hypertrophic granulation tissue's areas using a planimeter, up until the healing process was completed. The results were statistically analyzed.
Results: Twenty patients with cutaneous wounds located on the head, trunk and limbs were treated. The average weekly percentage reduction compared to the baseline area was 32.5%. The results were statistically significant.
Conclusions: Cryosurgery is a practical, cost effective and non-invasive method and can be indicated for the treatment of hypertrophic granulation tissue in cutaneous wounds.
Keywords: GRANULATION TISSUE; CRYOSURGERY; THERAPEUTICS
The presence of granulation tissue and reepithelialization are necessary for the healing of a cutaneous wound. The granulation tissue replaces cells that have lost their function. It occurs in physiological situations or due to multiple pathological conditions in the body. However, in some cases, the production of hypertrophic granulation tissue (HGT), which develops beyond the surface of the wound, resulting in an elevated mass, or peduncle, hampers healing in several ways, for instance preventing the migration of epithelial cells on the surface of the wound, increasing the risk of infection or causing pain, discomfort and difficulty in healing.1 Cryosurgery is a treatment modality that uses liquid nitrogen, which became commercially available in 1940. Since then it has been commonly used in the freezing of cutaneous neoplasms due to its safety and effectiveness.2 The objective of the present article is to demonstrate the efficiency of cryosurgery in the treatment of HGT in cutaneous wounds.
A retrospective study was carried out with the data contained in the medical records of 20 patients originated at the Dermatology Ambulatory of the Fundação Pró-Hansen in the Brazilian southern city of Curitiba (PR), Brazil, bearing cutaneous wounds with HGT, due to ulceration of the lower limbs and surgical wounds left to heal by second intention, from 2012 to 2014. The patients who accepted to take part in the study signed a Term of Free and Informed Consent, also allowing use of photographs related to their conditions. Exclusion criteria were: presence of severe coagulopathies, local infection, decompensated diabetes, cryofibrinogenemia, cryoglobulinemia, thrombophlebitis, deep venous thrombosis and wounds with malignant neoplasia.
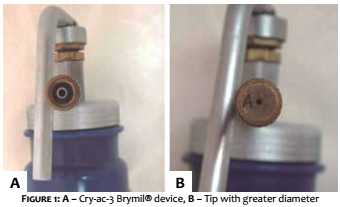
In the study, the Cry-ac 3® (Brymil Corporation, USA for Alcon Pharmaceuticals Cham, Switzerland) was used with the spray technique employing the largest diameter tip (A) (Figure 1).
Nitrogen was applied at a distance of approximately 5cm from the HGT area, at a 90º angle. The freezing time corresponded to approximately 2 cycles of 5 seconds, slightly varying according to the area to be frozen, with the number of sessions varying from 1 to 3. Large lesions were divided into quadrants for the application of liquid nitrogen – always limited to HGT - thus avoiding interfering with the migration of keratinocytes to the center of the wound. In the presence of fibrous borders, surgical debridement was performed.
The procedures were always performed by the same dermatologist physician.
In the postoperative period, the patients received dressings with neomycin and bacitracin ointment, which were replaced twice a day after the wound had been cleansed with saline solution. For wounds located in the lower limbs, the patient was instructed to prepare the crepe bandage with aimed at containing exudate and occasional small bleedings.
Clinical observation, photographic documentation and measurement of the areas of the wounds and the HGT were performed weekly for the assessment of results. The measurement of the areas were carried out using a decal that was later analyzed by a polar planimeter (Fa.OTT, type 16, Kempten, Germany). The device is comprised of two hinged metallic rods that are joined by a disk equipped with a counter. The free end of one of the rods is held fixed, while the free end of the second rod is moved over the perimeter of the flat surface to be measured – in this case the decal – allowing the calculation of the area of each lesion.
In the statistical analysis, the results of quantitative variables were described by mean values, medians, minimum and maximum values, and standard deviations. Qualitative variables were described by frequencies and percentages. The comparison of two groups regarding quantitative variables was performed using the non-parametric Mann-Whitney test. The association between quantitative variables was evaluated by estimating the Spearman correlation coefficient. Values of p <0.05 indicated statistical significance. The data were analyzed using the software IBM SPSS v.20.0.
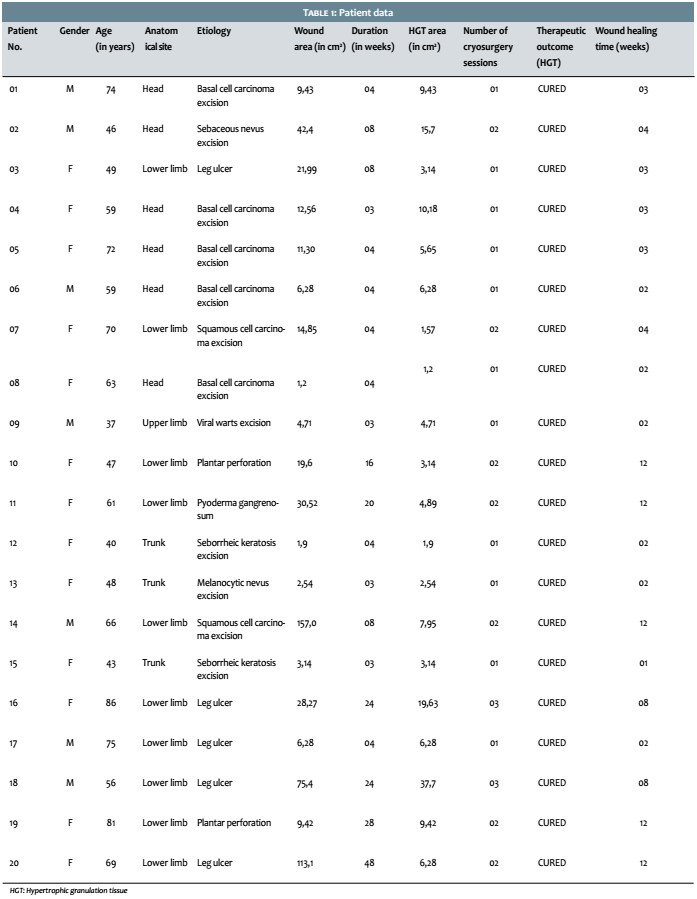
This study describes outcomes in 20 individuals bearers of cutaneous wounds with HGT (7 men and 13 women), with a mean age of 60.1 years (min = 37 years, max = 86). (Table 1)
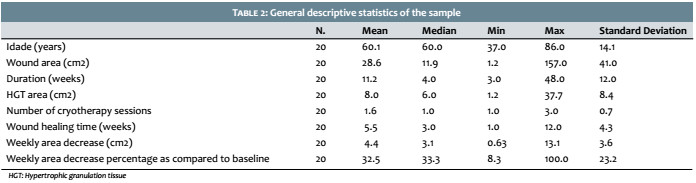
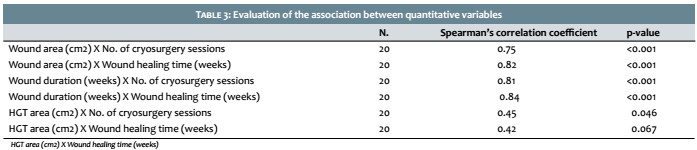
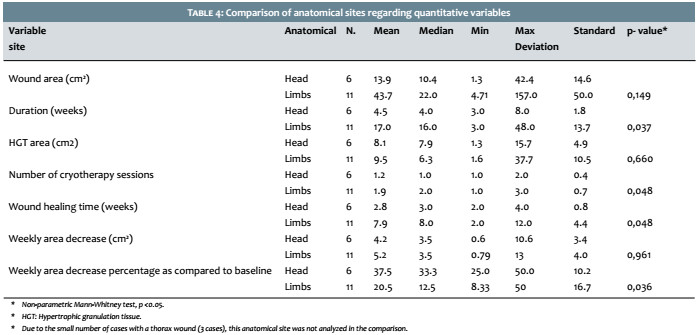
The mean area of the wounds was 28.6 cm2, with the largest being 157.1 cm2 (lower limbs), and the smallest 1.2 cm2 (head). The mean area of the HGT was 8 cm2, with the largest being 37.7 cm2 (lower limbs) and the smallest 1.2 cm2 (head). The fastest healing occurred in 7 days, in a lumbar lesion, probably due to the fact that the triggering factor was removed (contact eczema caused by the adhesive plaster). The longest healing time occurred in lesions in the lower limbs. The number of sessions ranged from 1 to 3. The average area reduction per week was 4.4 cm2, with a minimum of 0.63 cm2 and a maximum of 13.1 cm2. The weekly mean reduction percentage as compared to the baseline area was 32.5%, and ranged from 8.3% to 100% (Tables 1 and 2). The results suggest that there was statistical significance for these associations, in turn lending significance to the paired comparisons between the wounds’ areas and the number of cryosurgery sessions (p <0.001), the wounds’ areas and the healing time (p <0.001), the wounds’ durations and the healing time (p <0.001), and the HGT areas with the number of cryosurgery sessions (0.046). However, the values of the correlation coefficients (0.45) suggest that these associations are not strong, despite being statistically significant. The correlation between the HGT area and the wounds’ healing times was not statistically significant (P = 0.067) (Table 3). The results suggest the presence of statistical significance in the associations of the wound duration with the anatomic site (p = 0.037), the number of cryosurgery sessions with the anatomic site (p = 0.048), the wounds’ healing times with the anatomic sites (P = 0.048), and the weekly area reduction percentage regarding the initial area with the anatomical site (p = 0.036). There was absence of statistical significance for the association between the wounds’ areas and the anatomical site (p = 0.149), the HGT areas with the anatomical site (p = 0.660), and also the association between the weekly wound area reductions with the anatomical site (P = 0.961) (Table 4).
In 1913, the American neurosurgeon Dr. Irving S. Cooper was the first used cryosurgery with liquid nitrogen in brain tumors. In 1967, Dr. Setrag A. Zacarian developed a handheld device termed Kryospray, which popularized the use of this device.3
It is characterized by being cost effective and offering a fast recovery for the patient, who can return to his professional activities in a shorter time, as compared to other therapeutic methods. Cryosurgery produces selective destruction of compromised tissue, while the stroma promotes the subsequent repair of the wound. The collagen’s and cartilage fibers’ resistance to the damage caused by freezing favors the healing of the lesion.4
Liquid nitrogen based cryosurgery has been widely used given it is safe, offers good effectiveness, is easy to handle, yields good therapeutic and cosmetic results, and does not need anesthesia. The rapid loss of heat promotes the freezing of the skin’s nerve endings, causing a pre-anesthetic effect. This freezing creates a momentary, uncomfortable burning sensation, which is however self-limited. Cryosurgery has been used for the treatment of a wide spectrum of diseases, encompassing benign, premalignant and malignant cutaneous lesions. Liquid nitrogen also stimulates the immune response and is currently deemed as the best cryogen.5
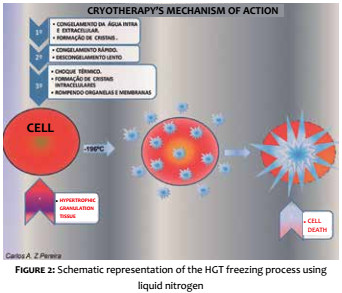
Freezing promotes crystallization of intracellular and extracellular water, culminating in cell death. Vascular stasis also occurs, contributing to the tissue’s necrosis. It is important to note that this tissue destruction is selective. (Figure 2)
The pathophysiology of HGT formation is still unclear, however probable etiologies can be grouped into: inflammatory nature (type 1), causes linked to the wound’s occlusive environment (type 2), and causes linked to some type of cellular imbalance (type 3). Regardless of the cause, it is important to rule out the possibility of malignancy. Type 1 is treated with the removal of the inflammatory or irritating factor. In cases of infection, it is important that the treatment includes systemic antibiotic therapy. Type 2 responds well to dressing changes – usually a permeable film that favors gas exchange at the interface of wound and dressing. In type 3 there may be internal or external causes of cellular imbalance. If external, they should be treated according to signs and symptoms using the same strategies used for types 1 and 2. If internal, the treatment is still unknown.1
Other treatment options described in the literature include mechanical, curettage or shaving debridement; chemical cauterization, laser therapy, topical silver nitrate, phenol, copper sulphate and aluminum chloride.6-9
Mechanical removal of hypergranulation may cause a return to the inflammatory phase, resulting in a new wound, while the application of caustic agents may cause pain.6 In turn, silver nitrate, if used frequently in large areas, can cause methemoglobinemia and hyponatraemia.10,11
The use of imiquimod has also been reported in the treatment of HGT in plantar perforation, with complete healing occurring after a 18-week period.12
The fact that there are several therapeutic options based on different methods demonstrates that HGT is a therapeutic problem, with lack of scientific reports on the advances in the area.6
In the present study, it was possible to observe that HGT interferes in the wound healing process, making reepithelialization difficult, due to the relief produced in the center of the wound, which interferes with the migration of keratinocytes. When left untreated, HGT can hinder healing for several weeks, producing a large volume of yellowish exudate. After treatment with cryosurgery the authors of the present article observed improvement of healing in the first week due to the flattening of the wound bed, which facilitates reepithelialization. (Figure 3)
Patients with extensive wounds with HGT in the lower limbs describe intense local pain. After the onset of reepithelialization and at the point which the skin has covered the wound, there is a reduction of the exudate and pain sensation (Figure 4A-4B-4C). In the present study, these signs were observed in 3 patients who had presence of HGT in the surgical wound, when dressing was performed in the postoperative period with antibiotic and clostebol cream, which has healing action.
In surgical wounds resulting from the excision of malignant neoplasias left to heal by second intention and developing with HGT, it is necessary to evaluate the histological examination’s safety margins, in order to ensure the complete excision of the tumor.
In cases of leg ulcers that course with infection, it is important to request the culture and antibiogram before starting the antibiotic therapy.
Granulation tissue is important in the healing process of full thickness wounds, however when it becomes hypertrophic it should be diagnosed and treated as early as possible. Surgical wounds of partial thickness resulting from excision using the shaving technique can heal with the formation of HGT, as seen in patients who underwent excision of sebaceous and melanocytic nevi (Table 1).
No complications are observed in the cryosurgery technique, provided that the patients comply with the instructions, cleansing the wound and changing dressings using the recommended cream.
The treatment of ulcers with HGT in the lower limbs is difficult and prolonged, especially if the etiology is pyoderma gangrenosum or plantar perforation due to leprosy neuropathy. In these cases it is possible to make use of cryosurgery with antibiotic therapy, and treat the underlying disease. In the present study, the wounds that presented the longest cicatrization time were located in the lower limbs (Tables 1 and 4).
It is important to detect the formation of hypertrophic granulation tissue in the early stages in order to avoid long treatments that generate expenses and discomfort for the patient. Cryosurgery is a practical, cost effective, noninvasive method with a low incidence of complications and excellent therapeutic outcome, and can be indicated for the treatment of HGT in cutaneous wounds.
1. Vuolo J. Hypergranulation: exploring possible management options. Br J Nurs. 2010;19(6):S4, S6-8.
2. Zimmerman EE, Crawford P. Cutaneous Cryosurgery. Am Fam Physician. 2012; 86(12):1118-1124.
3. Cooper SM, Damber RPR . The history of cryosurgery . J R Soc Med. 2001;94(4):196-201.
4. Gage AA, Baust JM, Baust JG. Experimental cryosurgery investigations in vivo. Cryobiology. 2009;59(3):229-43.
5. Moraes AM, Velho PENF, Magalhães RF. Criocirurgia com nitrogênio líquido e as dermatoses infecciosas. An Bras Dermatol. 2008;83(4):285-298.
6. Harris A, Rolstad BS. Hypergranulation tissue: a nontraumatic method of management. Ostomy Wound Manage. 1994;40(5):20-30.
7. Hawkins-Bradley B, Walden M. Treatment of a nonhealing wound with hypergranulation tissue and rolled edges. J Wound Ostomy Continence Nur. 2002;29(6):320-4.
8. Semchyshyn NL. Dermatologic surgical complications. Medscape [Internet]. 2016 Sep [cited 2009 Sep 25]. Available from: http://emedicine. medscape.com/article/1128404-overview#a1
9. Stevens NM, Shultz T, Mizner RL. Gersh M. Treatment in an out-patient setting for a patient with an infected, surgical wound with hypergranulation tissue. Int J Low ExtremWounds. 2009;8(1):37-44.
10. Rollins H. Hypergranulation tissue at gastrostomy sites. J Wound Care. 2000;9(3):127-9.
11. Dealey C. The Care of Wounds: a guide for nurses. 3nd ed. Oxford:Wiley -Blackwell; 2008.
12. Krishnaprasad IN, Soumya V, Abdulgafoor S. Management of over-granulation in a diabetic foot ulcer . IJPMR 2013;24(1):19-22.
This study was carried out at the Fundação Pró-Hansen - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}