


Gabriel A. de A. Sampaio1, Ada Regina Trindade de Almeida1, Ana Flávia Nogueira Saliba1, Natássia Pinheiro de Lavor Queiroz1
Keywords: HYPERHIDROSIS, GRAVIMETRY, SWEATING
Hyperhidrosis is a condition characterized by excessive, generalized, or focal sweating. Generalized hyperhidrosis involves the entire body and is usually associated with systemic problems such as endocrine or neurological disorders, or infections. -The primary or idiopathic focal form affects healthy people, being more frequent in the palmoplantar region, axillae, and face.1 The pathophysiology is not completely known, and is attributed to a dysfunction of the sympathetic nervous system.2
The diagnosis is carried out clinically, based on history and physical examination. The severity of hyperhidrosis is evaluated through objective (quantitative) or subjective measurements.1 Among the objective measurements, gravimetry-which quantifies the sweating weight (milligrams) per time unit (minutes)-is the more frequently described in the literature.3
Subjective evaluations are used to estimate the impact of the condition on the quality of life of patients, as well as the degree of severity. Since this condition can result in substantial hardship to the patient, subjective assessments of severity are important, including limitations to work, social interaction, physical activities and leisure, as well as psychological and social relationship disorders. The Hyperhidrosis Disease Severity Scale (HDSS) is specific for hyperhidrosis and measures its interference in individual patient's daily activities.4
The prevalence of focal hyperhidrosis is variable. In Brazil, epidemiological studies found a prevalence of 9% in the city of Blumenau, in the Southern State of Santa Catarina5 and 5. 5% among medical students in the city of Manaus, in the Northern State of Amazonas.6 Yet there are few reports of cases in the inframammary region, with references in two previous studies, serving only to exemplify this body site as a region of unusual focal sweating.7,8
The present study was aimed at characterizing inframammary hyperhidrosis in regards to its prevalence, associated factors, impact on quality of life, and gravimetry in patients treated at the Dermatology Clinic of the Hospital do Servidor Público Municipal de São Paulo.
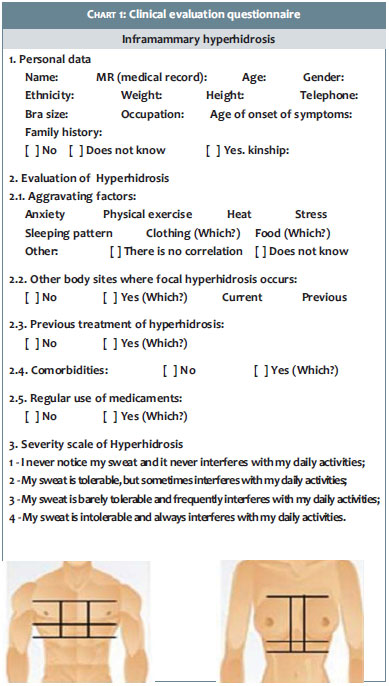
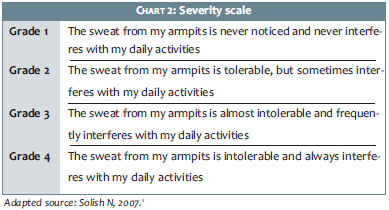
A cross-sectional, observational descriptive study was carried out. All patients were treated at the Dermatology Clinic of the Hospital do Servidor Público Municipal de São Paulo (SP), Brazil. During the course of a week they were questioned about the presence of excessive inframammary sweating. Those who answered positively were asked to complete a clinical questionnaire (Chart 1) and fill in an adapted severity scale based on the HDSS (Chart 2).
The criteria for inclusion of patients in the study were: 14 years of age or older, complaints of excessive inframammary sweating, and signing of the Free and Informed Term of Consent (FITC). Patients under 18 years of age who met the inclusion criteria could only take part in the study when accompanied by their legal representatives, who signed the FITC.
Exclusion criteria were the following: pregnancy, breast-feeding, children under the age of 14, and the refusal to take part in the study. All patients were properly informed about the voluntary nature of their participation, and the absence of any financial cost or incentive arising from their participation.
A questionnaire about personal data was applied (ID information, family history, improvement and/or worsening factors, comorbidities, use of medication, age when symptoms arose, and other areas of focal hyperhidrosis, which is part of the clinical evaluation of hyperhidrosis already standardized in other studies).9
The subjective evaluation of the impact of inframammary hyperhidrosis on the quality of life was carried out by the patients themselves, based on the graduation used in the HDSS scale.4
During the gravimetry analysis (Figure 2) all tests were performed in the same room under the same temperature range (25 to 29ºC), gauged with a model Cool23CTA40 thermometer (Incoterm®, PortoAlegre (RS), Brazil).
Moisture in the inframmamary region was removed with absorbent paper prior to performing the gravimetry test in order to avoid interference with the measurement of sweating. Paper filters (medium 102 paper filter, Melitta®, São Paulo (SP), Brazil) were previously weighed on a precision balance (Ohaus Precision Standard®, model TS 2KS, Metrohom, São Paulo (SP), Brazil) and then placed in the dried inframammary region. The filters were weighed again after five minutes with the difference between the two weight measurements being considered as the amount of sweat produced, in milligrams, during five minutes.
The data were analyzed through descriptive statistics and chi-square tests (X2 tests). A greater than 95% confidence interval and a significance level less than or equal to 5% were used.
The study was approved by the Ethics Committee of the Hospital do Servidor Público Municipal de São Paulo (Protocolo 227/2011, Parecer. 15/2011).
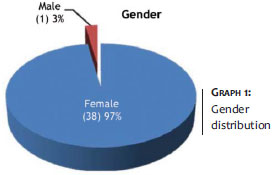
During the study period, 678 patients were treated. Thirty-nine (5.7%) answered positively about excessive sweating in the inframammary region (38 women and 1 man) (Graph 1).
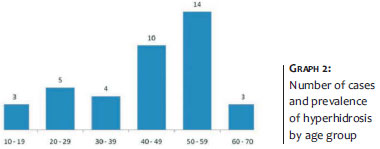
The most affected age group was that of 50-59 years-old (Graph 2), with an age of onset ranging 15-63 years.
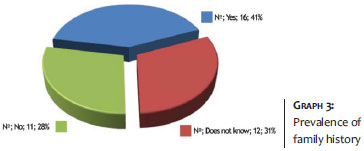
Positive family history for hyperhidrosis (Graph 3) was observed in 41% of patients (31% uncertain, 28% denied).
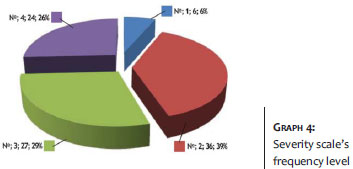
The following results were observed regarding the qualitative evaluation of severity, according to the HDSS adapted scale: Level 1:"I never notice my sweat and it never interferes with my daily activities." 6. 6% of cases; Level 2:"My sweating is tolerable but sometimes interferes with my daily activities." 36. 39%; Level 3: "My sweating is barely tolerable and frequently interferes with my daily activities." 27.29%; and Level 4: "My sweating is intolerable and always interferes with my daily activities." 24. 26% (Graph 4).
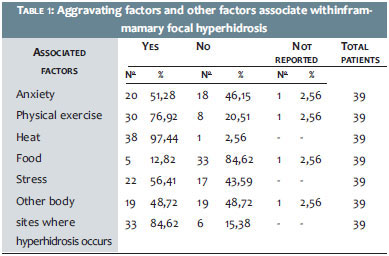
Aggravating associated factors were, in descending order: heat, physical exercise, mental stress, anxiety, clothing, and food. Association among hyperidrosis factors was observed in 84. 62% of cases (Table 1).
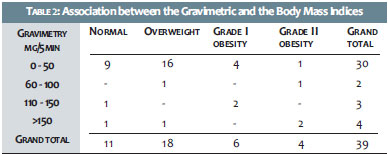
Gravimetry values ranged from zero (nil) to 330mg/5minutes. Attempts to correlate these values with other independent variables suggested no significant association between gravimetry and family history (X2 = 31. 754, p = 0. 2014), bra size (X2 = 120,078, p = 0. 7224), or severity scale (x2 = 9. 497, p = 0. 3927). There was statistically significant association between body mass index and gravimetric results (Table 2), both for isolated results (X2 = 56,456, p = 0. 0349) and for weight range group (X2 = 19,838, p = 0. 0189).
Although previous studies carried out in Brazil have estimated the frequency of focal hyperhidrosis according to the body site where it occurs, the prevalence and characterization of inframammary hyperhidrosis was first described in the present study.
The age group10 and positive family history11 were in line with the literature's data for other focal hiperidroses-in the U. S. population there was a higher prevalence in the 45-55 year-old age group and 47. 5% frequency in patients with a family history.
Statistical association found between gravimetry and body mass index corroborates the hypothesis that the degree of obesity is reflected in the body surface area and density of sweat glands, being also observed in other areas of focal hyperhidrosis.
Body mass index was recently evaluated in patients in Brazil with facial hyperhidrosis, with an absence of results that indicated correlation.12 Though not based on statistical data, a positive relationship between obesity and primary hyperhidrosis was nonetheless observed in a Brazilian study carried out with medical students in the city of Manaus, in the northern State of Amazonas.
Other features of inframammary hyperhidrosis were similar to those observed in studies focusing on diverse body sites. The frequency observed in the severity scale was similar to that observed in the pioneering study that standardized such a scale,13 with a higher prevalence in Level 2:" My sweating is tolerable, but sometimes interferes with my daily activities.", and Level 3:"My sweating is barely tolerable and frequently interferes with my daily activities.".
Aggravating and/or other factors associated with inframammary hyperhidrosis were similar to those found in previous studies that focused on other body sites where focal hyperhidrosis typically occurs, and where a greater association with heat, stress, anxiety, and physical exercise was observed in epidemiological surveys in the U. S. and Canadian populations.11
The coexistence of inframammary hyperhidrosis with other affected body sites was also reported by the patients (84. 62%), and is consistent with the association between different areas of focal hyperhidrosis already described in the literature.10
The prevalence of inframammary hyperhidrosis-a condition that has been little studied to date-demonstrates its importance as a primary and focal variant of hyperhidrosis.
The use of gravimetry and a severity scale were instrumental in evaluating inframammary sudoresis. The degrees of severity showed that sudoresis exerts a frequent and important impact on the quality of life of patients and can be approached therapeutically. Therefore, there is consensus that it should be seen as an abnormality.
The methodology used in this study was similar to that employed in studies aimed at characterizing other forms of focal hyperhidrosis 5,6,13 and can serve as a base for future studies on therapeutic options that can be used to improve patients' quality of life.
1. Solish N, Bertucci V, Dansereau A, Hong HC, Lynde C, Lupin M, et al. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: Recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol Surg. 2007;33(8):908-923.
2. Almeida ART, Hexsel DM. Hiperidrose e Toxina Botulínica. São Paulo: Edição das autoras; 2003.
3. Hund M, Kinkelin I, Naumann m, Hamm H. Definition of axillary hyperhidrosis by gravimetric assessment. Arch Dermatol. 2002;138(4):53-41.
4. Solish N, Benohanian A, Kowalski JW; Canadian Dermatology Study Group on Health-Related Quality of Life in Primary AxillaryHyperhidrosis. Prospective open-label study of botulinum toxin type A in patients with axillary hyperhidrosis: effects on functional impairment and quality of life. Dermatol Surg. 2005;31(4):405-13.
5. Fenili R, Demarchi AR, Fistarol ED, Matiello M, Delorenze LM. Prevalência de hiperidrose em uma amostra populacional de Blumenau - SC, Brasil. An Bras Dermatol. 2009;84(4):361-6.
6. Westphal FL, de Carvalho MA, Lima LC. Prevalence of hyperhidrosis among medical students. Rev Col Bras Cir. 2011;38(6):392-7.
7. Walling HW. Primary hyperhidrosis increases the risk of cutaneous infection: a case-control study of 387 patients. J Am Acad Dermatol. 2009;61(2):242-6.
8. Walling HW. Clinical differentiation of primary from secondary Hyperhidrosis. J Am Acad Dermatol. 2011;64(4):691-5.
9. Leung AK, Chan PYH, Choi MCK. Hyperhidrosis. Int J Dermatol. 1999;38(8):561-7.
10. Cohen JL, Cohen G, Solish N, Murray CA. Diagnosis, impact and management of focal hyperhidrosis: Treatment review including botulinum toxin therapy. Facial Plast Surg Clin North Am. 2007;15(1):17-30.
11. Lear W, Kessler E, Solish N, Glaser DA. An epidemiologic study of hyperhidrosis. Dermatol Surg. 2007;33(1 Spec No):S69-S75.
12. Wolosker N, Campos JR, Kauffman P, Munia MA, Neves S, Jatene FB, et al. The use of oxybutynin for treating facial hyperhidrosis. An Bras Dermatol. 2011;86(3):451-6.
13. Strutton DR, Kowalski JW, Glaser DA, Stang PE. US prevalence of hyperhidrosis and impact on individuals with axillary hyperhidrosis: results from a national survey. J Am Acad Dermatol. 2004;51(2):241-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}