


Cintyadewi Wignjosoesastro; Diah Adriani Malik; Puguh Riyanto
Funding: None
Conflict of interest: None
Submitted on: 09/25/2025
Final decision: 10/15/2025
How to cite this article: Wignjosoesastro C, Malik CA, Riyanto P. Effectiveness of 1% Centella asiatica ointment in women with melasma: A study on the Melasma Area and Severity Index (MASI) and patient scores. Surg Cosmet Dermatol. 2025;17:e20250517.
INTRODUCTION: Melasma is a chronic dermatosis characterized by irregular hyperpigmented patches.
OBJECTIVES: To evaluate the effectiveness of topical Centella asiatica (CA) in treating melasma using the Melasma Area and Severity Index (MASI) Score and patient satisfaction.
METHODS: This single-blind randomized clinical trial (RCT) compared 1% CA ointment with 4% hydroquinone cream for 8 weeks, alongside daily sunscreen use. MASI score and patient satisfaction were measured before and after treatment, with adverse effects monitored throughout.
RESULTS: The CA group had a greater decrease in MASI scores but the difference between groups was not statistically significant. Patient satisfaction was similar between the two groups, with a slightly lower improvement in the CA group.
CONCLUSION: Both CA and hydroquinone significantly reduced MASI scores after 8 weeks, with no significant difference in effectiveness or patient satisfaction. CA may be considered a viable alternative for patients seeking comparable therapeutic outcomes with a lower risk of irritation.
Keywords: Skin Cream; Melanosis; Patient Satisfaction
Melasma is a chronic dermatosis characterized by irregular hyperpigmented patches, typically occurring symmetrically in the centrofacial, malar, and mandibular regions. The condition affects approximately 33% of the global population, particularly women of reproductive age in tropical regions. Its pathogenesis is multifactorial and involves sun exposure, hormonal influences, genetic predisposition, and various external factors.1 Severity is often evaluated using the Melasma Area and Severity Index (MASI) score and patient satisfaction with instruments like the Visual Analog Scale (VAS).2,3
First-line treatments for melasma include photoprotection and topical therapies, with hydroquinone the long-standing gold standard despite significant adverse effects. Consequently, alternatives such as tranexamic acid, azelaic acid, and metformin have been explored. Centella asiatica (CA), a plant known for its wound-healing, anti-inflammatory, and antioxidant properties, has shown potential as a natural depigmenting agent due to active compounds (eg, asiaticoside) that inhibit melanogenesis. However, to date, no experimental study has evaluated the effectiveness of topical CA for melasma using MASI scores and patient satisfaction.
This study uses MASI scores and patient satisfaction to assess the effectiveness of topical CA in treating melasma.
This single-blind (subject-blinded) randomized clinical trial (RCT) employed a two-group pre- and post-test treatment and control design. The study was conducted at the Dermatology and Venereology Clinic of Diponegoro National Hospital, in Semarang, Indonesia, and was approved by the hospital’s Ethical Review Board. A total of 40 participants aged 18 years or older, with melasma and Fitzpatrick skin types III-IV, as determined by clinical presentation and Wood’s lamp examination, were enrolled. Participants with a history of hypersensitivity to hydroquinone, plants from the Apiaceae family, or sunscreen, or lesions with active infection on the face were excluded. The study also excluded participants with a history of using topical medication for facial melasma within the previous 14 days, cosmetic facial procedures (eg, laser, dermabrasion, or chemical peeling) within the past 3 months, pregnancy or lactation, or current contraceptive use. All participants provided written informed consent. Using a lottery method, participants were assigned to either of two groups, A and B, each with 20 participants. Convenience sampling with non-probability selection was used to recruit participants. In Group A, participants were instructed to apply 1% CA ointment, while in Group B, they were instructed to apply 4% hydroquinone cream.
All products used in this study are registered with the Indonesian Food and Drug Authority (BPOM), thereby ensuring patient safety and compliance with ethical standards.
Although ointments and creams differ in their physical properties and occlusivity, these variations do not necessarily affect therapeutic effectiveness. The 1% concentration of CA was chosen based on published data showing topical effectiveness within the 0.5–1% range. At this concentration, CA has been shown to promote wound healing, stimulate fibroblast proliferation, and enhance collagen synthesis while maintaining a favorable safety profile.
The active ingredient is derived from a standardized CA extract containing bioactive triterpenoids such as asiaticoside, madecassoside, asiatic acid, and madecassic acid, well-known in dermatology for their regenerative and reparative properties.
All participants were instructed to apply their respective medications over the affected area on the face at night and SPF 30 sunscreen in the morning every day for 8 weeks. Participants were observed before treatment and 8 weeks after. Participants were photographed before and after treatment, and their MASI score and patient satisfaction recorded at each visit. During treatment, adverse effects were noted and treated following standard protocols. SPSS version 27 was used for data entry and statistical analysis.
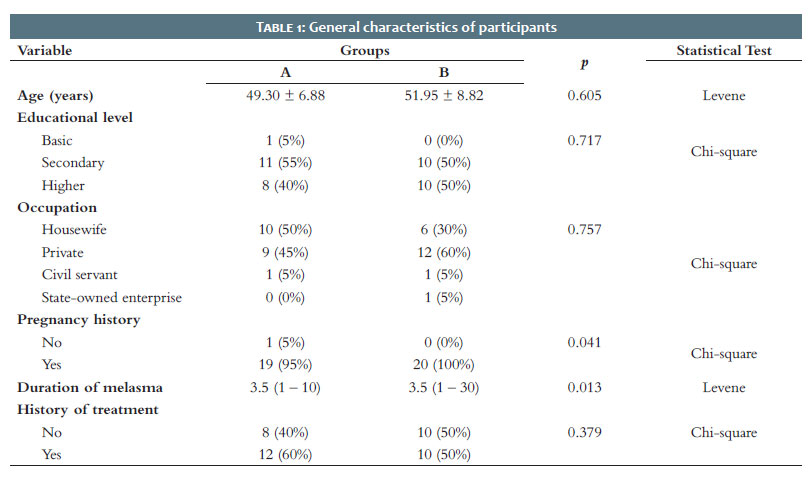
The general characteristics of the study population are shown in Table 1. The mean (SD) age in Groups A and B was 49.3 (6.88) and 51.95 (8.82) years, respectively. In Group A, educational attainment was basic education in 1 participant (5%), secondary education in 11 (55%), and higher education in 8 (40%). Meanwhile, in Group B, there were no participants with only basic education, while 10 (50%) had secondary education and 10 (50%) had higher education. In Group A, 50% of participants were housewives, 45% worked in the private sector, and 5% were civil servants. In Group B, 30% were housewives, 60% worked in the private sector, 5% were civil servants, and 5% were employees of a state-owned enterprise.
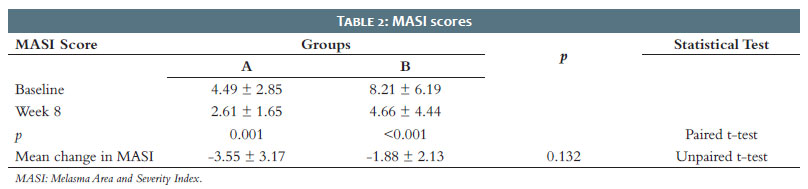
MASI scores at baseline (week 0) and at week 8, as well as the difference in MASI scores between the two groups, can be found in Table 2. The baseline MASI score in Group B was 4.49 (2.85), decreasing to 2.61 (1.65) at week 8. In Group A, the baseline MASI score was 8.21 (6.19), decreasing to 4.66 (4.44) at week 8. Both groups experienced a significant reduction in MASI scores after 8 weeks (p < 0.05), indicating that both treatments were effective (Figures 1 and 2). Although Group A showed a greater decrease in MASI scores compared to Group A (-3.55 vs. -1.88), the difference was not statistically significant (p = 0.132).
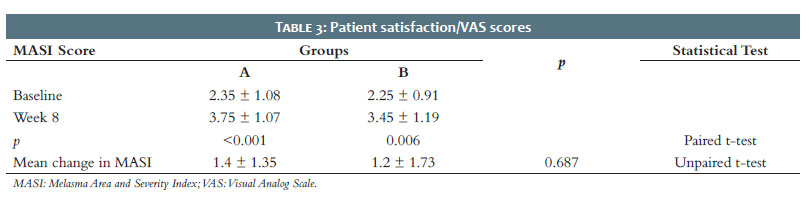
In Group A, the VAS score increased from 2.35 (1.08) to 3.75 (1.07), and the improvement was highly significant (p < 0.001). In Group B, the mean (SD) VAS score increased from 2.25 (0.91) at baseline to 3.45 (1.19) at week 8, a statistically significant improvement (p = 0.006). The mean (SD) change in VAS scores was 1.4 (1.35) in Group A and 1.2 (1.73) in Group B. However, this difference was not statistically significant (p = 0.687) in Table 3.
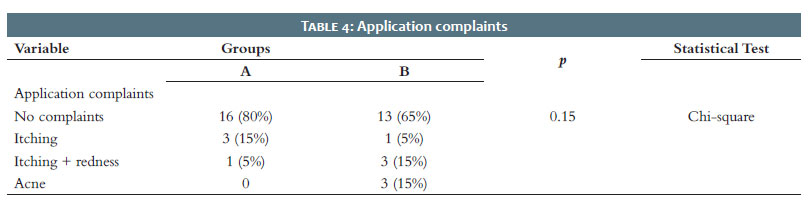
Complaints associated with hydroquinone and CA are shown in Table 4. Overall, 80% of Group A and 65% of Group B reported no complaints. Itching and redness were more frequent in Group B (15%) compared with Group A (5%). Acne was reported only in Group B (15%).
Mean (SD) age in the CA group was 49.3 (6.88) years, and 51.95 (8.82) years in the hydroquinone group, ranging from 33 to 68 years. This is similar to the populations in previous studies by Viorizka et al. and Hussain et al., in which age ranged from the second to the sixth decade of life.4 The most common age range was 46-55 years (49.4%).5
There were no significant differences between groups in terms of education. Low educational attainment is linked to a lack of knowledge about sun protection, an important risk factor for melasma. One study reported that African populations are less likely to use sunscreen despite a higher predisposition to pigmentary disorders.6
Regarding occupation, participants had similar characteristics to the study population in Seetan et al., in which more than half of the participants were housewives (59.3%).6 Viorizka et al. also reported that the majority of participants in their study were housewives (40.7% or 33 participants).5
CA can stimulate fibroblast proliferation and increase the synthesis of collagen and intracellular fibronectin, contributing to improve skin tension.7 Kwon et al. demonstrated the anti-melanogenic activity of CA.8 An in vitro study using human dermal fibroblasts found that CA significantly affected extracellular matrix protein deposition, stimulated fibroblast proliferation, increased collagen synthesis, and reduced metalloproteinase activity, thereby enhancing collagen deposition.9
Measuring treatment response and clinical improvement in melasma is important. The MASI score consists of three indicators: lesion area (A), lesion darkness (D), and hyperpigmentation homogeneity (H).2 This study found that in the CA group, the baseline MASI score was 8.21 (6.19), and 4.66 (4.44) at week 8. The mean (SD) reduction in MASI scores was greater in the CA group (-3.55 [3.17]) compared to the control group (-1.88 [2.13]). However, this difference was not statistically significant.
This study found a significant difference in VAS scores before and after treatment in the CA group (p = 0.002, p < 0.05), indicating increased patient satisfaction following the intervention. This suggests that topical CA significantly improves patient satisfaction in the treatment group (p < 0.001). Clinically, there was a positive trend in patient satisfaction after 8 weeks of treatment. The mean (SD) change in VAS in the hydroquinone group was 1.2 (1.73), compared with 1.4 (1.35) in the CA group; this difference was not statistically significant (p = 0.68).
In the hydroquinone group, 65% of participants reported no complaints, compared to 80% in the CA group, indicating a lower rate in the latter. Itching and redness were more common in the hydroquinone group (15%) compared to the CA group (5%). Acne occurred only in the hydroquinone group (15%). On the other hand, itching was more frequent in the CA group (15% vs. 5%). Calapai et al. reported no evidence of systemic or local toxicity associated with CA, and no participants experienced adverse effects.10 Hydroquinone, however, is associated with several known adverse effects, including erythema, allergies or irritant contact dermatitis, skin atrophy, and telangiectasia.11 To minimize these, hydroquinone therapy should be stopped for several months before reinitiation. Hydroquinone may also be applied on weekends or three times a week before maintenance therapy to minimize complications.12,13
Both CA and hydroquinone significantly reduced MASI scores after 8 weeks of treatment. There was no statistically significant difference in effectiveness between the two groups. Patient satisfaction improved in both groups, with no significant differences between them. Given its comparable effectiveness and lower risk of irritation, Centella asiatica may represent a suitable alternative for patients who want to avoid the adverse effects often associated with hydroquinone therapy.
Cintyadewi Wignjosoesastro
ORCID: 0009-0004-8623-1404
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Diah Adriani Malik
ORCID: 0000-0003-0575-9510
Statistical analysis, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Puguh Riyanto
ORCID: 0000-0002-2019-8937
Statistical analysis, Conception and design of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
1. Liu W, Chen Q, Xia Y. New Mechanistic insights of melasma. Clin Cosmet Investig Dermatol. 2023;16:429–42.
2. Mahajan VK, Patil A, Blicharz L, Kassir M, Konnikov N, Gold MH, et al. Medical therapies for melasma. Vol. 21, Journal of Cosmetic Dermatology. John Wiley and Sons Inc; 2022. p. 3707–28.
3. Åström M, Thet Lwin ZM, Teni FS, Burström K, Berg J. Use of the visual analogue scale for health state valuation: a scoping review. Quality of Life Research [Internet]. 2023;32(10):2719–29. Available from: https://doi.org/10.1007/s11136-023-03411-3.
4. Hussain A, Shahbaz U, Shaheen E, Ghias A, Khalid A, Aman S. Comparison of effectiveness and safety of topical 30% metformin versus 4% hydroquinone in the treatment of epidermal melasma. Journal of Pakistan Association of Dermatologists. 2024;34(1):73–9.
5. Viorizka PBB, Setyaningrum T, Qurnianingsih E, Damayanti. The profile and triggering factors of melasma patients: a retrospective study. Berkala Ilmu Kesehatan Kulit dan Kelamin. 2023;35(2):142–7.
6. Seetan K, Shatanawi M, Ali A, Khamees A, Alsheikh A, Alawneh A, et al. Disease characteristics, determinants, and perception of use of sunscreen and sun-protective behaviors among patients of color with melasma: a cross- sectional study. Photodermatol Photoimmunol Photomed. 2022;38(5):495-500.
7. Bylka W, Znajdek-Awizeń P, Studzińska-Sroka E, Brzezińska M. Centella asiatica in cosmetology. V. 30. Postepy Dermatologii i Alergologii. 2013. p. 46–9.
8. Kwon KJ, Bae S, Kim K, An IS, Ahn KJ, An S, et al. Asiaticoside, a component of Centella asiatica, inhibits melanogenesis in B16F10 mouse melanoma. Mol Med Rep. 2014;10(1):503–7.
9. Fernenda L, Ramadhani AP, Syukri Y. Aktivitas pegagan (Centella asiatica) pada dermatologi. Jurnal Sains Farmasi & Klinis. 2023;9(3):237.
10. Calapai G. Assessment report on Centella asiatica (L.) Urban, herba. European Medicine Agency. 2012;44:4.
11. González-Molina V, Martí-Pineda A, González N. Topical treatments for melasma and their mechanism of action. J Clin Aesthet Dermatol [Internet].2022;15(5):19–28.
12. Hydroquinone. Schwartz C, Jan A, Zito PM. . In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
13. AboAlsoud ES, Eldahshan RM, AbouKhodair Mohammed H, Elsaie ML. Safety and efficacy of topical metformin 30% cream versus triple combination cream (Kligman’s formula) in treating melasma: a randomized controlled study. J Cosmet Dermatol. 2022;21(6):2508–15.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}