


Carlos Gabriel Sánchez Urresta; Vivian Nunes Arruda; Ana Cristina Fortes Alves; Nelson Marcos Ferrari; Maria Victória Quaresma
Funding source: None.
Conflict of interest: None.
Submission date: 11/18/2024
Final decision: 01/16/2025
How to cite this article: Urresta CGS, Arruda VN, Alves ACF, Ferrari NM, Quaresma MV. Autologous melanocyte grafting by micropunch technique in patients with stable vitiligo: a pilot study in a tertiary hospital in Brazil. Surg Cosmet Dermatol. 2025;17:e20250424.
INTRODUCTION: Vitiligo is a dermatological condition that causes loss of skin pigmentation, significantly affecting patients' quality of life due to social stigma. Despite various therapeutic approaches, including topical treatments, systemic therapies, and phototherapy, many cases remain refractory.
OBJECTIVE: To report a series of cases to evaluate the effectiveness of autologous melanocyte grafting using the micropunch technique.
METHODS AND RESULTS: We selected 9 patients with stable and refractory vitiligo, totaling 15 surgeries. Of these, 93.3% showed some degree of repigmentation in the treated area, with the formation of a pigmentation halo around the grafts, as observed in post-surgical photographic follow-up. The inner arm was the most frequently used donor area (60%). The complications were minimal: 1 patient (6.7%) developed hypertrophic scarring in the donor area; 3 patients (20%) developed the "cobblestone appearance" in the recipient area, with 1 case resolving spontaneously after 6 months. There was also partial graft loss in 1 patient (6.7% of surgeries).
CONCLUSION: The results indicate that the micropunch technique is a viable and safe alternative for managing stable vitiligo, offering a new therapeutic option for cases refractory to conventional treatments.
Keywords: Vitiligo; Transplantation, Autologous; Skin Pigmentation.
Vitiligo is an autoimmune pigmentation disorder characterized by selective destruction of melanocytes, resulting in achromic patches on the skin that can affect any region of the body, including mucous membranes.1,2 Global prevalence of vitiligo ranges from 0.5% to 2.3%, and the condition is known to significantly impact the quality of life of individuals due to the social stigma associated with visible lesions.3,4 Vitiligo is classified into 2 main variants: segmental vitiligo (SV), which affects a single area or follows a dermatome, and nonsegmental vitiligo (NSV), which presents with scattered lesions in various regions.5,6 Studies indicate that SV tends to respond more favorably to surgical interventions due to its restricted distribution, whereas NSV tends to have a more unpredictable course.7 Treatments for vitiligo include drug therapies (topical and systemic), physical therapies (laser and phototherapy), and surgical interventions, each with its own limitations and specific indications.8,9 However, many patients achieve unsatisfactory results with these conventional approaches, especially those with SV and stable lesions. Given this limitation, punch micrografting has been explored as a viable alternative for skin repigmentation, offering an easy-to-perform option with the potential for good aesthetic results.1,10 This study aims to assess the degree of repigmentation of autologous melanocyte transplantation using punch micrografting in the treatment of achromic areas in patients with SV who are refractory to conventional clinical approaches.
This research was approved by the Research Ethics Committee (CAPPesq) of the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP) on February 9, 2024, Opinion No. 6,644,970 and CAAE No. 76811824.6.0000. 0068. A pilot study was conducted in a series of cases to assess the degree of repigmentation in areas treated with punch micrografting in adult patients aged 18 years or older diagnosed with SV. Patients were seen at the Inaesthetics Outpatient Clinic of the Dermatology Division of the HCFMUSP from November 2023 to December 2024. The inclusion criteria were: patients aged 18 years or older; clinical diagnosis of SV; patches with an area equal to or greater than 2 cm2, previously measured with a millimeter ruler; disease stability for at least 1 year, with no new lesions, increased depigmentation in existing lesions, or Koebner phenomenon; and cases that were refractory to conventional therapies, including topical and systemic medications and phototherapy, for at least 6 months. The exclusion criteria were: patients currently using physical therapies or topical or systemic corticosteroid therapy, and those who had used these therapies in the past 3 months; pregnant women; individuals with a history of hypertrophic scars and/or keloids; and patients who declined to sign the informed consent form.
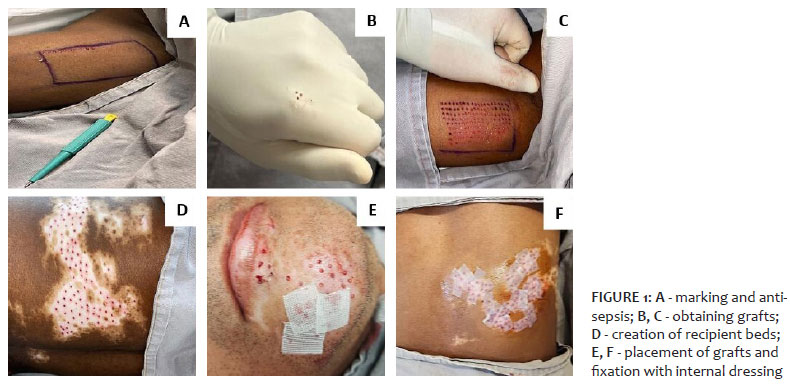
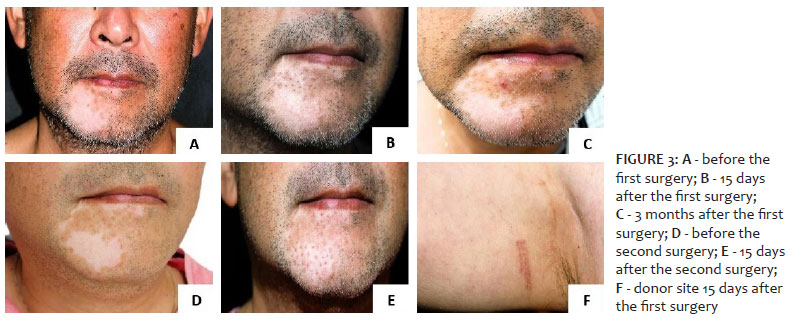
The donor and recipient sites were marked prior to surgery, followed by antisepsis with 2% alcoholic chlorhexidine solution (Figure 1 - A). Local anesthesia was administered with 2% lidocaine and adrenaline diluted 1:200,000. Punch micrografting, a technique first described by Falabella in 1978,1 involves transplanting epidermal and dermal tissue from a donor site to a recipient site using small-diameter punches (1 to 2 mm).1,7,10 In this study, a 2-mm punch was used to obtain the micrografts (Figure 1 - B, C). Following collection, the grafts were stored in a 0.9% saline solution. In the recipient site, a smaller diameter punch (1 mm) was used to create the recipient beds for the grafts (Figure 1 - D). The donor sites were protected with petrolatum and gauze and micropore® dressings (Figure 1- E, F). The number of grafts removed and beds created varied according to the extent of the area to be repigmented, and beds were spaced approximately 0.5 to 1.0 cm apart, allowing the pigment halos generated by each graft to merge (Figure 1 - D). The grafts were gently placed into position using curved Adson forceps, always ensuring that the dermal side of the graft was in contact with the bed (Figure 1 - E). After placing all the grafts, a 2-layer dressing was applied: the internal dressing, just above the grafts, made with petrolatum and micropore®, and the external dressing, with gauze and surgical tape (Figure 1 - F). Immediately after the completion of the surgical procedure, patients were instructed to keep the external dressing on the recipient site and the dressing on the donor site for 48 hours. Patients were also instructed to perform daily hygiene, removal of blood crusts, and dressing changes at home. The internal dressing in the recipient site was kept in place and removed 14 days postoperatively (Figures 2 and 3), when the results were assessed according to the protocol, monitoring the evolution and degree of repigmentation through photographic records on postoperative day 14, and subsequently on a monthly basis (Figures 2 and 3).
A total of 9 patients were included in the study, 6 women (66.7%) and 3 men (33.3%), with a mean age of 33.6 years. SV was predominant in the sample, present in 8 patients (88.9%), while only 1 patient (11.1%) had NSV. All participants had a history of disease stability, with a mean duration of 5.5 years, ranging from 2 to 11 years. In addition, all had received previous treatments, such as topical corticosteroids, calcineurin inhibitors, phototherapy, and systemic corticosteroid therapy for more than 3 years prior to surgery. However, these treatments failed to result in satisfactory repigmentation, which qualified them as candidates for autologous melanocyte transplantation. A total of 15 surgeries (100%) were performed among the 9 patients. Of these, 1 patient underwent 3 surgeries, 4 patients underwent 2 surgeries each, and 4 patients underwent only 1 surgery. Among the 15 interventions performed, 14 (93.3%) showed some degree of repigmentation in the treated site, evidenced by the formation of a pigmented halo around the grafts, as recorded during photographic follow-up. The inner arm was the most frequently used donor site, chosen in 9 surgeries (60%), followed by the gluteal region on 2 occasions (13.3%), the lumbosacral region in 1 (6.7%), the retroauricular region in 1 (6.7%), and the inner thigh in 1 (6.7%). Few complications were recorded in the donor and recipient sites. Only 1 patient (6.7% of surgeries) developed hypertrophic scarring in the donor site (Figure 4 - A), which demonstrates that the procedure is safe in most cases. In the recipient site, 3 patients (20% of surgeries) presented with a "cobblestone appearance" (Figure 4 - C), which is when the skin graft has an uneven texture with small bumps that look like stones. In 1 case (6.7% of surgeries), the condition resolved spontaneously after 6 months of follow-up. In addition, 1 patient (6.7% of surgeries) had grafts that failed to repigment (Figure 4 - B), a complication known as static grafts. Finally, 1 patient (6.7% of surgeries) had significant graft loss, with more than 50% in the first surgery (Figure 4 - D) and less than 50% in the second.
The results of this pilot study suggest that punch micrografting may be a viable alternative for the treatment of stable, refractory vitiligo. The predominance of SV in the sample (88.9%) is in line with other studies that indicate a more favorable response of this subtype of vitiligo to surgical interventions due to the smaller extent and distribution of lesions.1,7 The average duration of disease stability (5.5 years in our study) reinforces the importance of careful selection of candidates for surgery. Patients with stable vitiligo for a long period have a lower risk of developing new lesions after the intervention, an essential factor for the success of the treatment.3,6 In relation to complications, hypertrophic scarring in the donor site in only 1 patient reinforces the safety of the technique in most cases. Complications in the recipient site, such as "cobblestone appearance" and partial loss of grafts, are consistent with the findings of other studies, which indicate that these events are relatively common in punch micrografting. However, these issues can be minimized by improving graft placement techniques, such as using micropunches with a diameter smaller than 2 mm, creating thin grafts composed only of the epidermis and superficial dermis, using appropriate instruments, and performing rigorous postoperative follow-up.8,9 The predominant use of the inner arm as the donor site (60%) demonstrates its sufficiency for the procedure, considering its accessibility and compatibility with the characteristics of the recipient site. Other sites, such as the gluteal and retroauricular region, were chosen for patients with specific needs, suggesting that the selection of the donor site should be customized according to the anatomical and aesthetic characteristics of each case.4,5 This study has limitations, including the small sample size and the absence of a control group, which hinders the generalization of the results. However, the data obtained provide an important basis for future studies and reinforce the potential of the punch micrografting as a therapeutic option for stable and refractory SV.
Vitiligo is a dermatological condition with significant prevalence, especially in a country like Brazil. Although it is not physically disabling, its lesions are highly stigmatizing, having a great impact on the quality of life of individuals. Despite the various clinical treatments available, many cases remain refractory to conventional therapies. In this context, melanocyte micrografting using a micropunch emerges as a promising alternative, combining efficacy and ease of execution. This procedure can bring substantial benefits to the quality of life of patients with stable vitiligo, providing a therapeutic option for those refractory to traditional treatments.
Carlos Gabriel Sánchez Urresta
ORCID: 0000-0002-7332-9435
Conception and design of the study, preparation and writing of the manuscript, acquisition, analysis and interpretation of data, critical review of the literature, critical revision of the manuscript
Vivian Nunes Arruda
ORCID: 0000-0002-7114-1869
Approval of the final version of the manuscript, effective participation in the conduct of the study, critical revision of the manuscript
Ana Cristina Fortes Alves
ORCID: 0009-0009-0485-6205
Author's contribution: Approval of the final version of the manuscript, effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied
Nelson Marcos Ferrari
ORCID: 0009-0008-3556-4611
Effective participation in the conduct of the study, intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Maria Victória Quaresma
ORCID: 0000-0003-2891-1650
Approval of the final version of the manuscript, conception and design of the study, preparation and writing of the manuscript, effective participation in the conduct of the study, critical review of the literature, critical revision of the manuscript.
1. Falabella R, Barona MI. Surgical approaches for stable vitiligo: an overview. J Am Acad Dermatol. 2009;60(3):474-91.
2. Alghamdi KM, Kumar A, Taïeb A, Ezzedine K. What patients with vitiligo have to say about their condition: a qualitative study. Br J Dermatol. 2019;180(3):564-70.
3. Sehgal VN, Srivastava G, Aggarwal AK. Vitiligo: prevalence, distribution and related aspects in rural community of Haryana. Indian J Dermatol Venereol Leprol. 2019;70(3):187-90.
4. Passeron T, Ortonne JP. Physiopathology and genetics of vitiligo. J Autoimmun. 2005;25(Supplement):63–8.
5. Desai S, Dhamanaskar D, Gohil A. Segmental vitiligo and its surgical treatment. Int J Dermatol. 2020;59(5):593-600.
6. Kumar R, Mehta R, Sharma N. Advances in vitiligo surgical techniques. J Cutan Aesthet Surg. 2021;14(1):55-63.
7. Lahiri K. Vitiligo management update: a consensus view from expert vitiligo academicians in India. Indian J Dermatol. 2012;57(6):383-90.
8. Mehta NR, Shah KC. Long-term outcome of various surgical modalities in the management of stable vitiligo. J Cutan Aesthet Surg. 2017;10(3):140-6.
9. Nath SK, Majumder PP, Nordlund JJ. Genetic epidemiology of vitiligo: multilocus recessivity cross-validation. Clin Dermatol. 2018;36(5):637-43.
10. Grochocka M, Welniak A, Bialczyk A, Marek-Jozefowicz L, Tadrowski T, Czajkowski R. Management of stable vitiligo—a review of the surgical approach. J Clin Med. 2023;12(5):1984.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}