


Marina Riedi Guilherme1; Bruna Cristina Mendes dos Santos1; Osvaldo Szenczuk1; Ligia Márcia Mário Martin1,2; Cássio Rafael Moreira1,2
Submitted on: 26/07/2021
Approved on: 19/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Guilherme MR, Santos BCM, Szenczuk O, Martin LMM, Moreira CR. Acral amelanotic melanoma. Surg Cosmet Dermatol. 2022;14:e20220081.
Acral amelanotic melanoma is rare and can mimic many entities, such as eccrine poroma, squamous cell carcinoma, plantar wart, and chronic ulcers. Due to the variety of possible differential diagnoses, it is a challenging and frequently late diagnosis. Dermoscopy features can help in early diagnosis. The dermatologist should keep this diagnosis in mind when faced with a pink, progressively growing, irregularly shaped lesion, mainly if located on the hands and feet.
Keywords: Dermoscopy; Melanoma amelanotic; Skin neoplasms; Oncology; Foot ulcer
Amelanotic melanoma is a subtype of cutaneous melanoma that shows no or little amount of pigment at macroscopy, dermoscopy, and histology.
Approximately 2-8% of melanomas are amelanotic. The final diagnosis is usually late due to the delay in identifying signs of malignancy.1 Dermoscopy is an essential tool for anticipating these findings, allowing early suspicion, biopsy, and treatment. We present a case of acral amelanotic melanoma with typical dermoscopic findings, and we highlight the importance of the diagnostic suspicion.
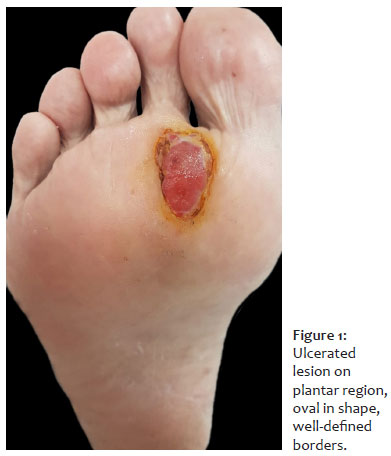
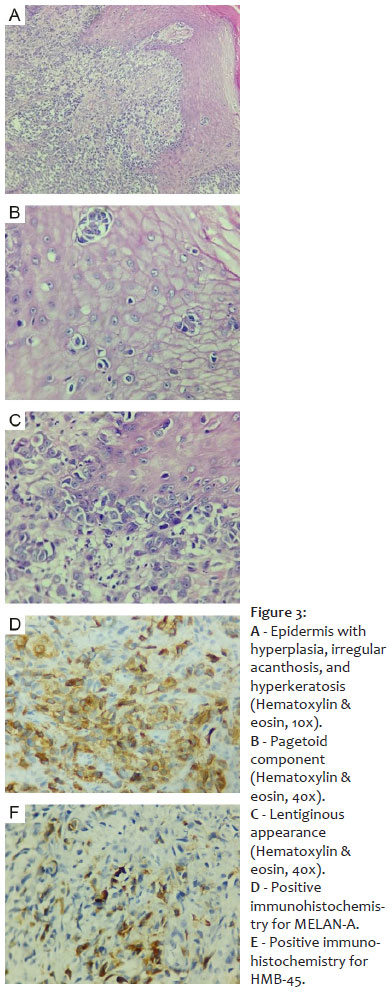
A 74-year-old man came to the Dermatology Outpatient Clinic complaining of a tumor in the right plantar region with five months of evolution. He was being followed up at the Basic Health Unit due to the hypothesis of chronic vascular ulcer. However, as the lesion showed growth and local pain, he was referred to the Dermatology Specialty Center. Dermatological examination revealed an oval-shaped ulcerated tumor in the right plantar region, with well-defined and elevated edges, and no signs of secondary infection (Figure 1). Dermoscopic examination showed a milky-red background, with vascular polymorphism combining dotted vessels and irregular linear vessels, and the presence of textile fibers (Figure 2). We referred the patient for an excisional biopsy of the lesion. The histopathology revealed the epidermis with hyperplasia, irregular acanthosis, and hyperkeratosis (Figure 3A), in addition to the presence of the pagetoid component (Figure 3B), mitoses, and lentiginous aspect of the lesion (Figure 3C). Immunohistochemistry was positive for MELAN-A (Figure 3D) and HMB-45 (Figure 3E), concluding that it was an amelanotic malignant melanoma, with a Breslow index of 8.6 mm.
The patient was referred to the Oncology Service of the municipality for staging and margin expansion. The investigation evidenced the presence of pulmonary and inguinal lymph node metastases. Clinical treatment with carbo-taxol was started, but the patient did not tolerate it and died seven months after the diagnosis of the lesion.
Amelanotic melanoma can be divided into two subtypes according to the clinic and dermoscopy of the lesions: “true” and hypomelanotic. True amelanotic melanoma does not show pigment either clinically or on dermoscopy. Some authors even add histology, with less than 5% of tumor cells with melanin. Hypomelanotic melanoma has no pigment in the clinic but shows small pigmented areas on dermoscopy.2
Any subtype of cutaneous melanoma can be amelanotic, but it is more common in subungual (25%) and desmoplastic melanoma. The literature suggests three primary clinical forms of amelanotic melanoma: erythematous macula with epidermal changes, which occurs more commonly in photoexposed areas; normochromic dermal plaque without epidermal changes; and papular-nodular form, responsible for 58% of cases of amelanotic melanoma.3
In the absence of pigment, vascularization helps in the dermoscopic examination of amelanotic melanoma. Dermoscopy is difficult because the vessels may disappear depending on the pressure placed between the dermoscope and the lesion.4 In general, there are six vascular patterns: dotted vessels, comma vessels, regular or irregular linear vessels, glomerular vessels, hairpin-like vessels, and arboriform vessels.5
The literature considers as dermoscopic features with the highest positive predictive value for suspected melanoma the presence of brown spots or globules of irregular size or distribution, multiple blue-grey spots, irregular depigmentation, blue-white veil, more than one shade of pink, milky-red areas, vessels mainly in the central region of the lesion, vascular polymorphism combining mainly dotted, irregular linear, and hairpin-like vessels. Some additional criteria are white areas of regression, ulceration, white structures, and inverted network.
On the other hand, characteristics with the highest negative predictive value for melanoma are more than three milia-like cysts, the predominance of comma-shaped vessels in the lesion, and arboriform vessels only.6,7,8
In the case reported, the initial diagnostic hypothesis of the primary care physician was a chronic ulcer with a probable vascular origin, which is one of the differential diagnoses of plantar ulcers, as well as plantar warts, eccrine poroma, plantar perforating ulcer, squamous cell carcinoma (SCC), and acral melanoma. The dermoscopic examination allowed assessing the characteristics suggestive of amelanotic melanoma and provided the best possible follow-up for the case, which emphasizes the importance of the dermatologist in the evaluation of skin lesions for the early diagnosis of potential malignancies, as well as the relevance of dermoscopic examination knowledge to increase the specialist’s diagnostic accuracy.
Amelanotic melanoma is a rare condition; however, it has a high mortality rate, mainly due to late diagnosis. The dermoscopic examination has become an essential ally to anticipate the diagnosis of these lesions and improve the prognosis. The presence of vascular polymorphism and milky-red background in a pink lesion should raise suspicion of malignancy and prompt biopsy.
Marina Riedi Guilherme 0000-0003-4765-2180
Study design and planning; preparation and writing of the manuscript; critical literature review.
Bruna Cristina Mendes dos Santos 0000-0002-6789-5836
Preparation and writing of the manuscript.
Osvaldo Szenczuk 0000-0002-2002-2990
Critical revision of the manuscript.
Ligia Márcia Mário Martin 0000-0002-4293-9580
Approval of the final version of the manuscript; critical revision of the manuscript.
Cássio Rafael Moreira 0000-0002-8781-1505
Approval of the final version of the manuscript; active participation in research orientation.
1. Giorgi V, Gori A, Savarese I, D'Errico A, Papi F, Grazzini M, et al. Clinical and dermoscopic features of truly amelanotic plantar melanoma. Melanoma Res. 2017;27(3):224-30.
2. Gong HZ, Zheng HY, Li J. Amelanotic melanoma. Melanoma Res. 2019;29(3):221-30.
3. Stojkovic-Filipovic J, Kittler H. Dermatoscopy of amelanotic and hypomelanotic melanoma. J Dtsch Dermatol Ges. 2014;12(6):467-72.
4. Menzies SW, Kreusch J, Byth K, Pizzichetta MA, Marghoob A, Braun R, et al. Dermoscopic evaluation of amelanotic and hypomelanotic melanoma. Arch Dermatol. 2008;144(9):1120-7.
5. Zalaudek I, Kreusch J, Giacomel J, Ferrara G, Catricalà C, Argenziano G. How to diagnose nonpigmented skin tumors: a review of vascular structures seen with dermoscopy: part I. Melanocytic skin tumors. J Am Acad Dermatol. 2010;63(3):361-74.
6. Argenziano G. Dermoscopedia [Internet]. Amelanotic/hypomelanotic melanoma [Acessed 17 jul 2021]. Available from: https:dermoscopedia.org.
7. Rezze GG, Paschoal FM, Hirata SH. 2nd ed. Atlas de Dermatoscopia Aplicada. São Paulo: Lemar; 2014.
8. Giacomel J, Zalaudek I. Pink lesions. Dermatol Clin. 2013;31(4):649-78.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}