


Priscila Neri Lacerda; Maria Estela Bellini Ribeiro; Izabelle Ferreira da Silva Mazeto; Vinícius de Souza; Hélio Amante Miot
Financial support: None
Conflict of interest: None
Submitted on: 30/04/2021
Approved on: 18/08/2021
How to cite this article: Lacerda PN, Ribeiro MEB, Mazeto IFS, Souza V, Miot HA. Infantile melanoma: early diagnosis by total body mapping in dysplastic nevus syndrome. Surg Cosmet Dermatol. 2021;13:20210040
Melanoma is a rare neoplasm in the pediatric population, and it is even rarer in children under 10 years of age. Total body mapping constitutes a low-cost and non-invasive method that increases diagnostic accuracy in evaluating pigmented lesions, especially in high-risk patients. We reported the case of a 9-year boy with dysplastic nevus syndrome, in which one lesion presented a subtle change (asymmetry of structures) within a 6-months follow-up. Its excision resulted in melanoma with a Breslow thickness of 1 mm and a negative sentinel lymph node. Total body mapping reduces the number of unnecessary excisions. It allows diagnosis of melanomas in early and potentially curable stages, especially in children and patients with risk factors such as dysplastic nevus syndrome. We report this case due to the rarity of the neoplasia in this age group and also to demonstrate the importance of sequential digital dermoscopy in early diagnosis of melanoma in this population.
Keywords: Dermoscopy; Melanoma; Dysplastic nevus syndrome
Melanoma is the second leading cause of cancer in adolescents and young adults. Its incidence significantly increases with age, but it is infrequent in children.1; Interactions between sun exposure, nevi development, and family history are the main determinants of melanoma development during the first decades of life.1,2 Predisposing factors such as giant congenital melanocytic nevus, xeroderma pigmentosum (XP), or genetic mutations have been reported in rare cases of childhood melanoma.1,2
Early recognition is essential to prevent disease progression. Therefore, a high index of suspicion is necessary when evaluating children.1,3 Dermoscopic examination is vital to visualize pigmented lesions’ morphological characteristics and differentiate melanoma from melanocytic nevi.3 However, early melanomas may show extremely discrete or absent signs on dermoscopy in the first exam, being only detected through morphological changes during the follow-up.³ Thus, body mapping can detect incipient melanomas.3
A nine-year-old boy, white, was referred to the Dermatology Service two years ago for follow-up due to multiple melanocytic nevi. The patient denied a family or personal history of melanoma.
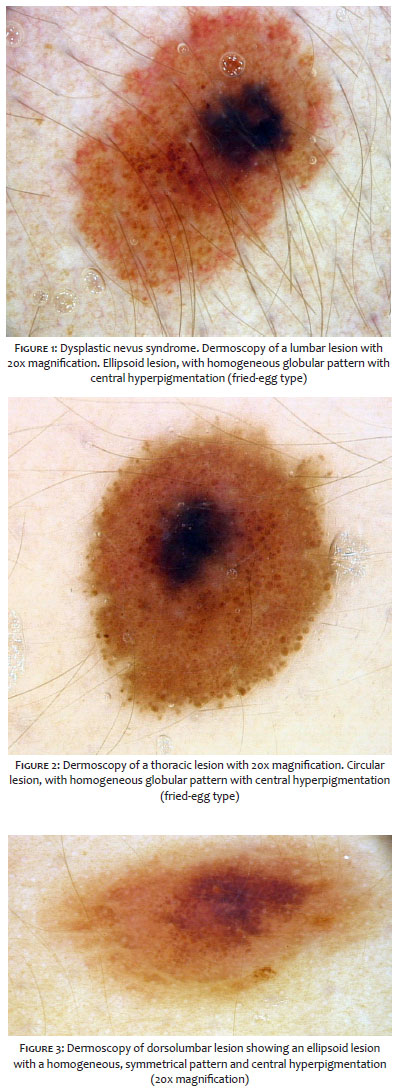
During the initial follow-up, dermoscopy presented nevus identity with homogeneous areas without structure, hyperpigmented, in a more centralized location (Figures 1-3). We performed exeresis, whose histopathology was compatible with a dysplastic nevus. The patient was referred to follow-up with body mapping (sequential digital dermoscopy).
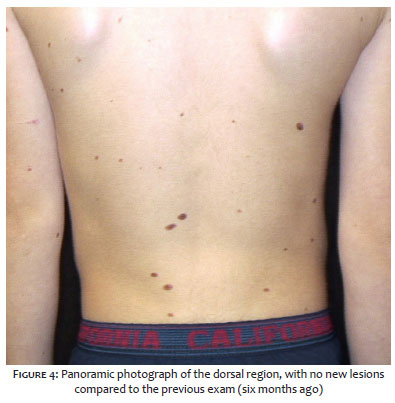
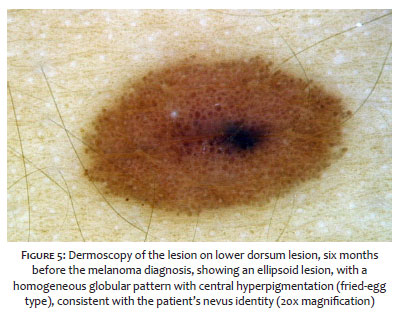
In the follow-up, the lesion evolved on the lower dorsum, which initially had characteristics similar to its nevus identity, with a homogeneous globular pattern and a central area without a hyperpigmented structure (Figures 4 and 5).
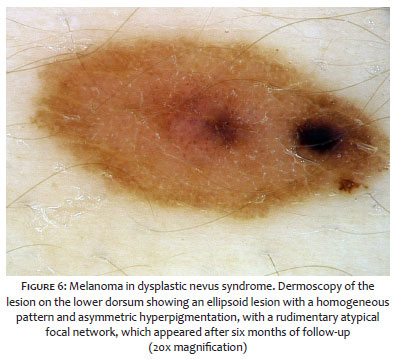
After six months, the lesion evidenced eccentric pigmented blur and atypical central vessels (Figure 6). We conducted the exeresis, and the histopathological examination revealed melanoma in the vertical growth phase, with a Breslow thickness of 1.0 mm, without ulceration, mitosis, or perineural invasion. We performed enlargement of the lesion margins and searched for sentinel lymph nodes, negative for neoplasia.
Melanoma is the most common skin neoplasm in children, although it is infrequent in this population, being even rarer in children under 10 years of age. Diagnosis is often tricky and late due to its rarity in this age group.3,4
Compared to adults, children have thicker primary lesions, often nodular and amelanotic, with atypical vascular structures or chrysalis, evidenced only by dermoscopy, in addition to not meeting the traditional ABCDE criteria.4,5 Furthermore, in contrast to melanoma in adults, a significant proportion of neoplasms arise from preexisting nevus (80%), and regular monitoring of lesions is essential for early diagnosis.4,5,6
Body mapping, or sequential digital dermoscopy, presents as a low-cost and non-invasive method capable of increasing the diagnostic accuracy in assessing pigmented skin lesions.7 The exam is based on the analysis of digital dermoscopic images sequenced throughout the time to find specific dynamic criteria that indicate a change in the biological behavior of the lesion.7,8 Thus, body mapping reduces the number of unnecessary excisions and allows the early diagnosis of early-stage and potentially curable melanomas.7,8
The importance of the examination is mainly due to young patients in whom the different pigmented lesions do not present typical characteristics at initial dermoscopy.6,7,8 Thus, when comparing the same lesion at different times, sequential digital dermoscopy allows the early detection of subtle changes that may suggest the diagnosis of melanoma.8,9
The nevus identity of the reported patient is composed of several dysplastic lesions with very similar or even more atypical dermoscopic characteristics than the lesion in which melanoma was diagnosed, making early diagnosis even more difficult.
In conclusion, this case confirms the importance of sequential body mapping as a fundamental tool for the early diagnosis of incipient melanoma in this population.
Priscila Neri Lacerda 0000-0001-8100-5978
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Maria Estela Bellini Ribeiro 0000-0002-4116-244X
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Izabelle Ferreira da Silva Mazeto 0000-0003-2325-8701
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Vinícius de Souza 0000-0002-4971-0439
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Hélio Amante Miot 0000-0002-2596-9294
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Saiyed FK, Hamilton EC, Austin MT. Pediatric melanoma: incidence, treatment, and prognosis. Pediatric Health Med Ther. 2017;8:39-45.
2. Pappo AS. Melanoma in children and adolescents. Eur J Cancer. 2003;39(18):2651-61.
3. Brandão FV, Rezze GG, Canosa JM. The contribution of total body mapping and digital dermoscopy for the early diagnosis of melanoma. Surg Cosmet Dermatol. 2021;4(4):364-6.
4. Neves JM, Duarte B, Lopes MJP. Melanoma em idade pediátrica: epidemiologia, patogênese, diagnóstico e tratamento. SPDV. 2020;78(2):107-13.
5. Brecht IB, De Paoli A, Bisogno G, Orbach D, Schneider DT, Leiter U, et al. Pediatric patients with cutaneous melanoma: a european study. Pediatr Blood Cancer. 2018;65(6):e26974.
6. Merkel EA, Mohan LS, Shi K, Panah E, Zhang B, Gerami P. Paediatric melanoma: clinical update, genetic basis, and advances in diagnosis. Lancet Child Adolesc Heal. 2019;3(9):646-54.
7. Tschandl P. Sequential digital dermatoscopic imaging of patients with multiple atypical nevi. Dermatol Pract Concept. 2018;8(3):231-7.
8. Gadens GA. Lack of compliance: a challenge for digital dermoscopy follow-up. An Bras Dermatol. 2014;89(2):242-4.
9. Kittler H, Guitera P, Riedl E, Avramidis M, Teban L, Fiebiger M, et al. Identification of clinically featureless incipient melanoma using sequential dermoscopy imaging. Arch Dermatol. 2006;142(9):1113-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}