


Bruna Cristina Mendes dos Santos1; Marina Riedi Guilherme1; Mayara Teixeira Cruz1; Marcelo de Souza Machado2; Lúcia Emiko Imazu3
Submitted on: 15/04/2021
Approved on: 15/07/2021
Financial support: None
Conflict of interest: None
How to cite this article: Santos BCM, Guilherme MR, Cruz MT, Machado MS, Imazu LE. Basal cell carcinoma of the vulva: a case report of cutaneous neoplasia in a special area. Surg Cosmet Dermatol. 2021;13:e20210033.
Basal cell carcinoma (BCC) is the most common skin cancer1. Among the risk factors for its development are exposure to ionizing and non-ionizing radiation, some chemicals, and previous scars.2 However, the most important factor is exposure to ultraviolet radiation, which explains the higher incidence of this neoplasm in photo-exposed areas.1 BCC in unexposed areas is uncommon. The purpose of this report is to describe a case of recurrent BCC in the vulva, to demonstrate the importance of dermatological examination in unusual areas, and to report the application of Mohs micrographic surgery.
Keywords: Basal cell carcinoma; Vulvar diseases; Vulvar neoplasms
Basal cell carcinoma (BCC) is the most common skin cancer, representing approximately 70% of cases.1 Among the risk factors for developing this type of tumor is exposure to ionizing and non-ionizing radiation, some chemical substances, such as tar and arsenic derivatives, and previous scars.2 However, the most important factor in BCC pathogenesis is exposure to ultraviolet radiation. This explains this neoplasm’s higher incidence in sun-exposed areas, affecting mainly fair-skinned and light-eyed people.1
BCC in non-photo exposed areas such as underarms, groin, buttocks, perianal, genital, and pubic regions is uncommon. BCCs that arise in the perianal area or on the vulva, specifically on the non-mucous surface of the labia majora, represent less than 2% of this type of epithelial tumor.3
This study aims to describe a case of recurrent BCC in the vulva, demonstrating the importance of surveillance of dermatological examination in unusual areas and reporting the application of Mohs micrographic surgery to spare and preserve special anatomical sites.
The 70-year-old white female patient, noticed. a mildly painful and slightly itchy lump inside her vulva, on the left (Figure 1). During a gynecological consultation in 2015, the patient’s physician observed the lesion and referred her to the dermatologist.
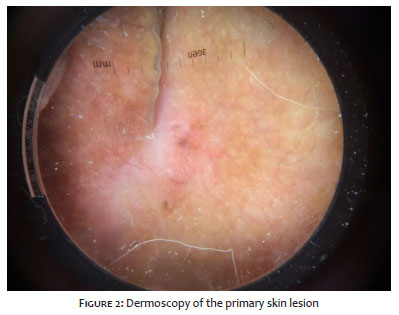
The dermatologist performed the analysis and raised the hypothesis of basal cell carcinoma. The lesion’s biopsy confirmed the hypothesis, showing a superficial basal cell carcinoma (Figure 2). However, as this is a rare involvement site for this type of skin cancer, the patient was referred to another Dermatology service in the state of São Paulo to get a second opinion from a dermatologist specialized in Cutaneous Oncology on the appropriate treatment for the lesion. In this service, the patient started treatment with imiquimod five times a week for six weeks and, after this cycle, the lesion disappeared.
However, a year later, the lesion reappeared in the same site, and a new biopsy was performed. The pathological examination confirmed that it was a recurrence of the previous basal cell carcinoma. The dermatologists who accompanied the patient, after discussing the case, suggested that the lesion was removed using the Mohs micrographic technique due to its greater precision and safety.
In 2016, the patient underwent surgical excision of the lesion, performed with free lateral and deep margins (Figure 3). Since then, the patient has undergone annual visits to the dermatologist. There has been no recurrence of the lesion to date.
BCC arises from follicular stem cells. Thus, its development in hairless areas is uncommon.4 The site of greatest involvement is the cephalic region (90%), mainly in the orbitopalpebral and nasal area, followed by the trunk and limbs.2 The most important factor in the pathogenesis of BCC is exposure to ultraviolet light. However, up to a third of cases occur in covered areas, such as armpits, groin, buttocks, perianal, genital, and pubic region.3,5,6
To date, the literature has described less than 300 cases of vulvar BCC. Tumors in this location represent approximately 2% of all BCCs and less than 3% of vulvar carcinomas.4 The exact cause of BCC development in non-sun exposed areas is still uncertain, but the relationship with increasing age has been reported in two large case series, in which the mean age of vulvar BCC development was between 70 and 73 years.7,8
Vulvar BCC shares the same risk factors as the sun-exposed BCCs. What sets them apart is that exposure to ultraviolet (UV) radiation does not play an important factor in the pathogenesis of vulvar BCC. Nevertheless, some authors suggest that exposure to UV radiation causes systemic immunosuppression, and it could be related to the BCC appearance in areas not exposed to the sun.9 Previous radiation is also one of the factors that predispose to vulvar BCC. Usually, the onset of lesions occurs years after exposure to irradiation.10,11 Another risk factor is genetic defects that can predispose to the development of BCC, such as the PTCH mutation, which leads to basal cell nevus syndrome and substantially increases the susceptibility to this neoplasm.12
The clinical manifestations of vulvar BCCs are nonspecific and don’t have classic BCC features. Lesions can appear as papules, nodules, or lesions that can be exophytic, pediculated, infiltrative, pigmented, and ulcerated in more advanced cases, or even in the combined form of these items.13 The signs and symptoms are not characteristic. The most reported ones are irritation, pain, and local itching. The non-specificity of the symptoms often causes the lesions to be treated as inflammatory and infectious dermatoses, leading to late diagnosis and, consequently, to an increase in the size of the neoplasm and local invasion.8
The vulvar BCCs are more aggressive when compared to the sun-exposed BCCs, and they are associated with deep local infiltration and occasional perineural extension. This type of neoplasm has a greater recurrence, as well as higher levels of local and distant metastases. It varies according to the histological pattern, and morphea-like, metatypic, adenocystic, and infiltrative tumors tend to be more recurrent and aggressive. 14, 15, 16
Surgical excision is the best form of treatment for vulvar BCC. Surgical margins should be wide, as a retrospective study showed that up to 25% of excisional biopsy margins were compromised. It is mainly due to the difficult demarcation, as this site is naturally erythematous, and the edges of the lesion are easily confused with healthy skin.8 The involvement of the margins results in a higher recurrence rate, which may reach 10% to 20% of cases.14
In large, histologically aggressive BCCs and in those with recurrence and poorly delimited borders, such as the tumor in this case report, Mohs micrographic surgery is the treatment of choice. It provides histological control of 100% of the margins, preserving normal skin, in addition to reducing changes in anatomical structures, making the reconstruction safer and with better aesthetic and functional results. In cases where the surgical approach is contraindicated or where there is edge involvement, radiotherapy is a therapeutic option, but it can lead to complications in the irradiated site.3,17,18
Early diagnosis is crucial to ensure less invasive surgery. However, vulvar BCC often has a delayed diagnosis because it occurs in a location that is less monitored during the physical examination.8 We concluded that there must be awareness that BCCs can appear in non-photo exposed areas and, many times, they can mimic other dermatoses. Thus, dermatologists, general practitioners, and gynecologists should perform a complete skin examination, especially in patients with a history of skin cancer, and biopsy is advisable in any suspicious skin lesion in these regions.
Bruna Cristina Mendes dos Santos 0000-0002-3213-3962
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marina Riedi Guilherme 0000-0003-4765-2180
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mayara Teixeira Cruz 0000-0002-5069-0519
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marcelo de Souza Machado 0000-0001-8817-0183
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Lúcia Emiko Imazu 0000-0002-6634-5509
Active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Belda Junior B, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 3th ed. Rio de Janeiro: Atheneu; 2018.
2. Azulay RD, Azulay DR, Azulay-Abulafia L. Dermatologia. 6th ed. Rio de Janeiro: Gen; 2013.
3. Pisani C, Poggiali S, De Padova L, Andreassi A, Bilenchi R. Basal cell carcinoma of the vulva. J Eur Acad Dermatol Venereol. 2006;20(4):446-8.
4. Sakai T, Goto M, Kai Y, Kato A, Shimizu F, Okamoto O, et al. Vulvar basal cell carcinoma with bone metastasis. J Dermatol. 2011;38(1):97-100.
5. Gloster HM Jr, Brodland DG. The epidemiology of skin cancer. Dermatol Surg. 1996;22(3):217-26.
6. Bhagchandani L, Sanadi RE, Sattar S, Abbott RR. Basal cell carcinoma presenting as finger mass. A case report. Am J Clin Oncol. 1995;18(2):176-9.
7. Gibson GE, Ahmed I. Perianal and genital basal cell carcinoma: A clinicopathologic review of 51 cases. J Am Acad Dermatol. 2001;45(1):68-71.
8. de Giorgi V, Salvini C, Massi D, Raspollini MR, Carli P. Vulvar basal cell carcinoma: retrospective study and review of literature. Gynecol Oncol. 2005;97(1):192-4.
9. Strickland PT, Creasia D, Kripke ML. Enhancement of two-stage skin carcinogenesis by exposure of distant skin to UV radiation. J Natl Cancer Inst. 1985;74(5):1129-34.
10. Benedet JL, Miller DM, Ehlen TG, Bertrand MA. Basal cell carcinoma of the vulva: clinical features and treatment results in 28 patients. Obstet Gynecol. 1997;90(5):765-8.
11. Mateus C, Fortier-Beaulieu M, Lhomme C, Rochard F, Castaigne D, Duvillard P, et al. Carcinome basocellulaire de la vulve: 21 cases. Ann Dermatol Venereol. 2001;128(1):11-5.
12. Susong CR, Ratz JL. Basal-cell carcinoma occurring in an axilla: a case presentation and a review of factors related to tumor development. J Dermatol Surg Oncol. 1985;11(5):526-30.
13. Mulvany NJ, Rayoo M, Allen DG. Basal cell carcinoma of the vulva: a case series. Pathology. 2012;44(6):528-33.
14. Mulayim N, Foster Silver D, Tolgay Ocal I, Babalola E. Vulvar basal cell carcinoma: two unusual presentations and review of the literature. Gynecol Oncol. 2002;85(3):532-7.
15. Watson GA, Kelly D, Prior L, Stanley E, MacEneaney O, Walsh T, et al. An unusual case of basal cell carcinoma of the vulva with lung metastases. Gynecol Oncol Rep. 2016;18:32-5.
16. Jacobs GH, Rippey JJ, Altini M. Prediction of aggressive behavior in basal cell carcinoma. Cancer. 1982;49(3):533-7.
17. Suzuki HS, Sato MS. A experiência da implantação da cirurgia micrográfica de Mohs em um serviço universitário. Surg Cosmet Dermatol. 2012;4(2):206-7.
18. Miller SJ, Alam M, Andersen J, Berg D, Bichakjian CK, Bowen G, et.al. Basal cell and squamous cell skin cancers. JNCCN. 2010(8):836-64.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}