


Carla Aguiar Andrade1; Cláudia Cardoso de Macedo Oliveira1; Eduardo Vinícius Mendes Roncada1; Diogo Gonçalves Ribeiro2
Financial support: None
Conflict of interest: None
How to cite this article: Andrade CA, Oliveira CCM, Roncada EVM, Ribeiro DG. Primary oral mucosal melanoma: case report. Surg Cosmet Dermatol. 2021;13:e20210029
Oral mucosa melanoma (OMM) represents 0.2% to 8% of melanoma cases. It mainly affects the palate and gums of patients between 40 and 70 years old. It is initially asymptomatic, contributing to late diagnosis and poor prognosis. The treatment of choice consists of surgical resection, and adjuvant radiotherapy and chemotherapy may be used. We report a case in an 80-year-old male patient with primary gingival and hard palate melanoma who underwent tumor resection followed by palate reconstruction. We emphasize the importance of a complete physical examination and active search for lesions in the oral mucosa for early diagnosis.
Keywords: Melanoma; Mouth mucosa; Palate
Melanoma is the third most common type of skin cancer; however, it is uncommon in the oral mucosa.1,2 It mainly affects individuals over 40 years,3,4 with a slight predominance among men,5,6 and is located preferentially on the palate and gums. The condition presents a varied morphology, initially without symptoms, which leads to a late diagnosis and poor prognosis.7,8 The treatment of choice is surgical resection, followed or not by neck dissection, with the option of adjuvant chemotherapy or radiotherapy.9,10
We present a case of oral mucosal melanomas and discuss the differential diagnosis, treatment, and prognosis of these lesions.
The dentist referred an 80-year-old brown man for evaluation of an asymptomatic pigmented lesion, with four months of evolution, in the hard palate and upper region of the gingiva, on the right. The patient did not use dental prostheses and reported no drinking or smoking.
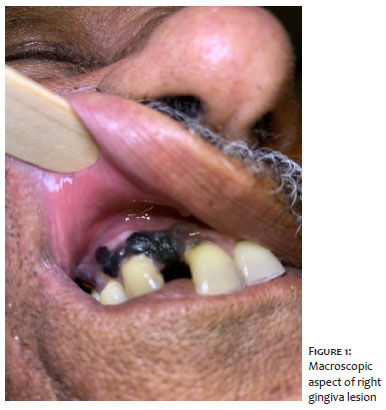
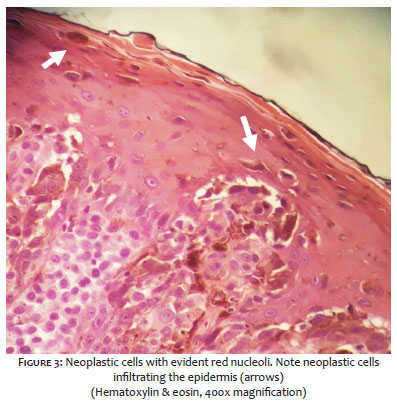
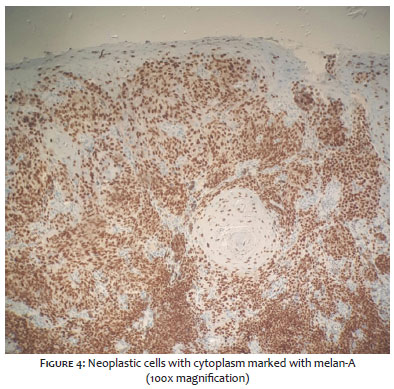
Oroscopy revealed a blackened plaque on the right hard palate, measuring approximately 1 cm, with an ulcerated area, accompanied by satellite lesions, and a blackened plaque on the right upper gingiva, measuring approximately 2.5 cm (Figures 1 and 2). Clinical examination showed no other suspicious lesions or palpable cervical lymph nodes. Computed tomography of the head, neck, and chest, abdominal ultrasound, and laboratory tests did not show significant findings. We performed an incisional biopsy, which showed an infiltrative growth neoplasm, consisting of anaplastic cells containing a large amount of melanin in the cytoplasm, with an intense degree of pleomorphism and nuclear atypia (Figure 3). The immunohistochemical profile was compatible with infiltrative malignant melanotic melanoma positive for HMB-45 and melan A (Figure 4).
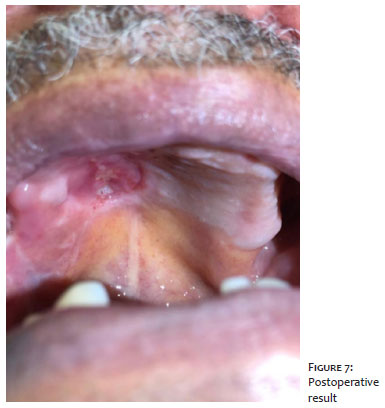
The patient underwent resection of the hard palate, medial upper gingiva fragment, teeth, and upper alveolar ridge on the right, followed by reconstruction of the palate using a right jugal mucosa flap (Figures 5 and 6). Histopathological examination of the surgical specimen confirmed the previous diagnosis of invasive malignant melanoma, with an extensive in situ component in the periphery of the lesion, ulceration, no perineural and angiolymphatic invasion, and surgical margins free of neoplasia. We chose not to perform cervical lymph nodes dissection and adjuvant treatment. The patient did not show signs of recurrence or dysfunction associated with the surgical procedure during a 12-month follow-up (Figure 7).
Oral mucosal melanoma (OMM) results from the uncontrolled growth of melanocytes found in the basal layer of oral mucous membranes.1-3 It is a rare tumor, representing only 0.2% to 8.0% of all melanomas and only 0.5% of oral malignancies,4-6 with reports of prevalence in Afro-descendants and Japanese.7,8 The highest incidence occurs after the age of 40, between the fifth and sixth decades of life, with a slight preponderance among men.9,10 They are located in 80% of cases in the hard palate and gingiva and 20% of cases in the oral mucosa, lips, tongue, base of the mouth, and uvula.7,9,10 Its etiology is unknown, as it is not associated with sun exposure.1,7,8 The condition has been linked to risk factors such as trauma, injuries from ill-fitting dentures, and exposure to alcohol, formaldehyde, and tobacco for long periods.3,4,6,10 Although most OMMs arise again, more than a third develop from benign melanocytic lesions.1,5,8
Initially, it presents as an asymptomatic macula or plaque that evolves with swelling, ulceration, bleeding, pain, tooth mobility, and the appearance of satellite lesions.7-10 Its color varies in shades of black, brown, gray, purple, and red. However, a third of the lesions present no pigment.3 It tends to recur locally and develop metastasis to lymph nodes (33%). In contrast, involvement of the lungs, brain, bones, and liver affects up to 85% of patients.4,5 Differential diagnosis includes amalgam tattoo, melanoacanthoma, smoking-associated melanosis, post-inflammatory pigmentation, melanocytic nevus, drug-induced melanosis (such as minocycline and antimalarials), Peutz-Jeghers syndrome, Cushing’s syndrome, Addison’s disease, Kaposi sarcoma, and other various conditions that cause pigmentation in the oral mucosa.1,2,8,9
Histologically, tumor cells are characterized by the proliferation of atypical melanocytes. The evaluated parameters include the presence or absence of melanocytes in the tumor; cell morphology (epithelial, spindle, plasmacytoid, or mixed); cellular organization (solid, alveolar, organoid, or pagetoid); presence of necrosis, perineural and perivascular invasion and depth of tumor invasion.7,10 Due to the lack of analogous histological landmarks between the skin and oral mucosa, the diagnosis of the depth or thickness of tumors, as defined by Clark and Breslow, is not accepted in the daily practice of OMM.4,7 Therefore, a classification based on the histopathological pattern of the tumor has been implied: melanoma in situ, limited to the epidermis and its junction with the connective tissue (15%); invasive melanomas, extending into the connective tissue (30%); and melanomas with a combined pattern between invasive and in situ (55%).1,5,8,10 The use of immunohistochemical staining helps confirm the diagnosis.9 The markers involved in the diagnosis of melanoma are S-100, HMB-45, melan-A, and tyrosinase.7,8 S-100 is sensitive (97%-100%) but not specific (75%-87%); HMB-45 and melan-A are considered more specific markers.8
The TNM system (tumor, lymph node, and metastasis) recognizes three stages for OMM:1,8
- Stage I: Presence of only primary tumor (N0M0)
Level I: Melanoma in situ with no evidence of invasion or “microinvasion”
Level II: Invasion to the lamina propria
Level III: Musculoskeletal, bone, or cartilage invasion
- Stage II: Tumor with metastasis to regional lymph nodes (N1M0)
- Stage III: Tumor with distant metastasis (M1)
Currently, the best option for treatment is complete surgical resection of the lesion with 1.5 cm of surrounding healthy tissue, with or without lymph node neck dissection.7,8,10 Some authors recommend adjuvant radiotherapy to maximize regional control.3,4,6 Chemotherapy and immunotherapy can prevent distant metastases.1 Careful monitoring of the patient is essential to check for recurrences.2
The prognosis is poor and related to advanced age, tumor extension, low resectability, amelanotic lesions, lymph node involvement, high mitotic rate of atypical melanocytes, and vascular or neural invasion. Five-year survival for OMM is around 15% to 30%.1,6,10
We report a primary oral mucosal melanoma case in a man who achieved therapeutic success after tumor resection and continues to be followed up in our Service to assess the recurrence or appearance of new suspicious lesions. The authors emphasize the importance of careful clinical examination for early detection of suspicious lesions, as cases of OMM are often initially asymptomatic, and early biopsy plays a fundamental role in the prognosis.
Carla Aguiar Andrade | 0000-0002-9348-5304
Preparation and writing of the manuscript; critical literature review.
Cláudia Cardoso de Macedo Oliveira | 0000-0002-2367-1662
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Eduardo Vinícius Mendes Roncada | 0000-0002-2149-2388
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
Diogo Gonçalves Ribeiro | 0000-0003-2024-1162
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Munde A, Juvekar MV, Karle RR, Wankhede P. Malignant melanoma of the oral cavity: Report of two cases. Contemp Clin Dent. 2014;5(2):227-30.
2. Manigandan T, Sagar GV, Amudhan A, Hemalatha VT, Babu NA. Oral malignant melanoma: A case report with review of literature. Contemp Clin Dent. 2014;5(3):415-8.
3. Oranges CM, Sisti G, Nasioudis D, Tremp M, DI Summa PG, Kalbermatten DF, et al. Hard Palate Melanoma: A Population-based Analysis of Epidemiology and Survival Outcomes. Anticancer Res. 2018;38(10):5811-7.
4. Malinoski H, Reddy R, Cohen DM, Bhattacharyya I, Islam MN, Bowers TL 4th. Oral Melanomas: A Case Series of a Deadly Neoplasm. J Oral Maxillofac Surg. 2019;77(9):1832-6.
5. Tchernev G, Lotti T, Wollina U. Palatal Melanoma: The Silent Killer. Open Access Maced J Med Sci. 2018;6(2):364-6.
6. Kumar V, Vishnoi JR, Kori CG, Gupta S, Misra S, Akhtar N. Primary malignant melanoma of oral cavity: A tertiary care center experience. Natl J Maxillofac Surg. 2015;6(2):167-71.
7. Topić B, Mašić T, Radović S, Lincender I, Muhić E. Primary Oral Mucosal Melanomas - Two Case Reports and Comprehensive Literature Review. Acta Clin Croat. 2017;56(2):323- 30.
8. Deyhimi P, Razavi SM, Shahnaseri S, Khalesi S, Homayoni S, Tavakoli P. Rare and Extensive Malignant Melanoma of the Oral Cavity: Report of Two Cases. J Dent (Shiraz). 2017;18(3):227-33.
9. Martinelli-Kläy CP, Laporte ML, Martinelli CR, Martinelli C, Lombardi T. Oral Malignant Melanoma Initially Misdiagnosed as a Racial Pigmentation: A Case Report. Dermatopathology (Basel). 2016;3(1):1-7.
10. Guevara-Canales JO, Gutiérrez-Morales MM, Sacsaquispe-Contreras SJ, Sánchez-Lihón J, Morales-Vadillo R. Malignant melanoma of the oral cavity. Review of the literature and experience in a Peruvian Population. Med Oral Patol Oral Cir Bucal. 2012;17(2):206-11.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}