


Jaqueline Barbeito de Vasconcellos; Isabele Oliveira Santos; Daniela Alves Pereira Antelo
Financial support: None
Conflict of interest: None
How to cite this article: Vasconcellos JB, Santos IO, Antelo DAP. Use of botulinum toxin for rosacea: a pilot study. Surg Cosmet Dermatol. 2021;13:e20210019
INTRODUCTION: Rosacea is a chronic inflammatory skin disease. The intradermal application of botulinum toxin (BT) has been studied as a therapeutic option for patients who struggle to manage flushing and/or persistent facial erythema. There is no standard protocol for TB application in rosacea.
OBJECTIVE: To evaluate the effectiveness of botulinum toxin application on erythematotelangiectatic rosacea.
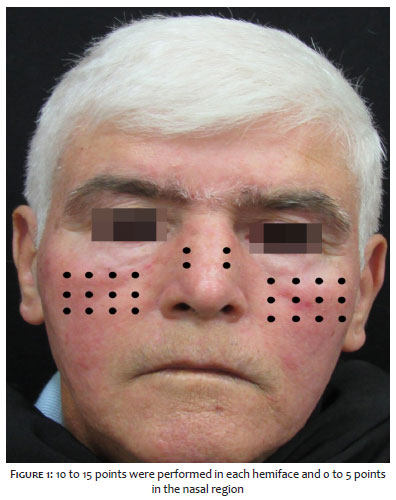
METHODS: Pilot study with case series. We applied intradermal TB in 10 patients with a diagnosis of rosacea and symptoms of persistent erythema and/or facial flushing. Patients received 10 to 15 injections per hemiface (1 unit of onabotulinum TB per injection) and 0 to 5 injections in the nasal region, totaling 25 to 35 units per patient.
RESULTS: Seventy-five percent of the patients presented a reduction in flush and erythema intensity. The follow-up time was three months, and no serious adverse events were observed.
CONCLUSIONS: The therapeutic arsenal to control erythema and facial flushing of rosacea, especially refractory to the usual treatment, should consider the intradermal application of TB type A.
Keywords: Erythema; Rosacea; Flushing; Botulinum toxins
Rosacea is a chronic inflammatory skin condition that predominantly affects the midfacial region. It is characterized by recurrent episodes of flushing, transient or persistent erythema, papules, pustules, and telangiectasias.1,2 Its prevalence ranges from 1% to 22%, according to different studies and populations.3
Although its pathophysiology has not yet been fully understood, the literature shows that innate immune deregulation and commensal skin microbiota imbalance occur. Triggering factors include mite Demodex folliculorum infection, ultraviolet radiation exposure, alcohol, heat, exercise, and spicy foods, which support the role of neurogenic inflammation in disease development.4,5 It is assumed that activating the peripheral sensory neurons of transient receptor potential vanilloid type 1 (TRPV1) and transient receptor potential ankyrin 1 (TRPA1) receptors stimulates the release of vasoactive neuropeptides that cause the disease exacerbation.5 In addition to vascular hyperreactivity, innate immune system deregulation through cathelicidin abnormal levels (antimicrobial peptides from human skin) also plays a central role in the pathogenesis of rosacea.5
Rosacea can be classified into four clinical presentations: erythematotelangiectatic, papulopustular, phymatous, and ocular. According to the 2017 ROSCO panel, this classification is shifting, and one or more characteristics may be present simultaneously in the same patient. The phymatous changes can be individually diagnostic for rosacea, and persistent centrofacial erythema, associated with periodic intensification by potential aggravating factors, is a feature of this condition. In their absence, the diagnosis can also be established by two or more main characteristics: papules and/or pustules, facial flushing, telangiectasia, and specific ocular manifestations.1,4
Management regimens aim to suppress inflammatory lesions, erythema, and, to a lesser degree, telangiectasia involved with rosacea.2 Treatment is based on the phenotype of each patient, and they often overlap. Topical agents such as metronidazole, azelaic acid, ivermectin, brimonidine, and oral agents such as tetracyclines are widely used. Technologies like intense pulsed light and off-label oral medications, such as antihypertensive beta-blockers and adrenergic agonists, can be used to control flushing. However, oral medications often have adverse events and, even with optimized treatment, it can be challenging to treat persistent erythema and flushing in refractory rosacea cases. The intradermal application of botulinum toxin (BT) has been studied as a therapeutic option in patients in whom flushing and/or erythema compromise the quality of life.6
This study aims to evaluate the effect of botulinum toxin type A (Botox®) application on rosacea erythema in a series of patients.
This is a pilot study with a series of cases. We selected ten patients from the Cosmiatry Clinic of the University Hospital Pedro Ernesto of the State University of Rio de Janeiro (UERJ). Patients of both genders diagnosed with erythematotelangiectatic rosacea (persistent facial erythema and episodes of facial flushing) were enrolled. All individuals agreed to participate in the research and signed the informed consent form (ICF).
We turned off the air conditioner and exposed the skin to the LED red light mask for five minutes to stimulate the erythema. Antisepsis of the face was performed with an alcoholic 2% chlorhexidine solution, followed by delimitation of the erythema region. Erythema was classified into: (1) absence of erythema; (2) erythema and/or mild flushing; (3) erythema and/or moderate flushing; (4) erythema and/or intense flushing; (5) very intense erythema and/or flushing.
We marked 10-15 application points per hemiface and 0-5 application points in the nasal region, with a distance of 1cm between them (Figure 1). Onabotulinum toxin (Botox®Allergan Inc., Irvine, CA, USA) was used, reconstituting the 100 U vial in 1 ml of 0.9% saline solution (1 U per 0.01 ml) and applying intradermally 1 U per marked point.
Clinical evaluation, photographic documentation, and quantification of erythema intensity were performed after 30 and 90 days.
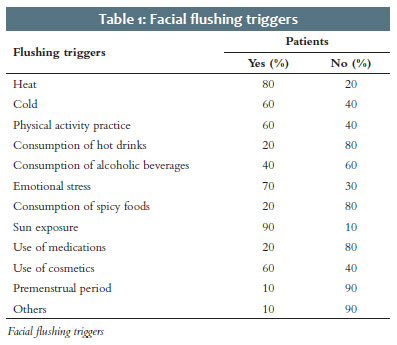
We conducted the treatment in eight women and two men. Age ranged from 19 to 60 years, and skin phototypes, from I to III. Among the triggering factors for erythema and flushing, sun exposure was the most reported, followed by exposure to heat, emotional stress, and physical activity (Table 1).
Of the 10 treated patients (P1 to P10), eight returned for reassessment on the scheduled dates (P1, P2, P3, P4, P7, and P10 showed up in 30 days; P1, P2, P3, P4, P5, and P6 showed up in 90 days).
Of the eight reassessed patients, five reported improvement in erythema and flushing symptoms within 30 days, one reported improvement within 90 days, and two subjects reported no improvement in symptoms. All patients who described enhancement within 30 days maintained the same positive report within 90 days (Figures 2 and 3).
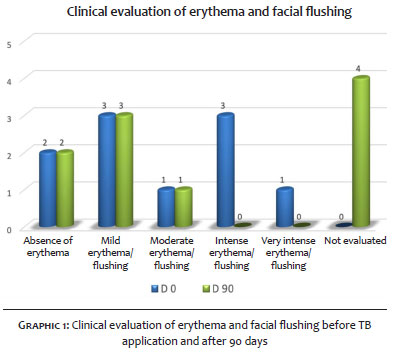
Regarding the analysis and clinical classification of facial erythema and flushing intensity after exposure to LED light, 63% of patients (n=5) decreased their intensity stage, 25% (n=2) remained in the same stage, and 12% (n=1) increased one intensity stage (Graph 1).
Statistical analyzes with non-parametric tests were performed, assessing the results at 30 and 90 days. For the D0-D90 test, the p-value was 0.035 (<0.05), rejecting the null hypothesis. Thus, we can say that there is a reduction in erythema after treatment, with statistical significance.
Adverse events were observed in only two patients: one presented ecchymosis at the BT application site with resolution within five days, and another presented mild asymmetrical smile (not perceived by the patient), corrected with the application of 1U of BT in the region of the contralateral zygomaticus major muscle.
The therapeutic arsenal to treat rosacea aims at controlling vascular inflammation. Topical medications such as metronidazole, azelaic acid, and, more recently, ivermectin reduce erythema related to vascular inflammation, as well as the group of oral cyclins. However, they have minor effects on erythema caused by permanently dilated superficial vessels.7 Vasoconstrictor drugs, such as brimonidine, which acts as an alpha-adrenergic agonist, promote transient effects on facial erythema (9 to 12 hours) with reports of a rebound effect.8 Some oral drugs, such as non-steroidal anti-inflammatory drugs, antihistamines, clonidine, and beta-blockers, have off-label use to control flushing in rosacea, with variable results and presence of adverse events.9 According to the ROSCO 2019 panel, topical alpha-adrenergic modulating agents and oral beta-blockers were discouraged due to limited scientific evidence to treat flushing.10
BT use was suggested in the search for other alternatives to treat flushing and facial erythema. Its mechanism of action is not yet fully understood. Among the hypotheses is the inhibition of the release of the neuropeptides associated with vasodilation and inflammation, such as substance P (SP), calcitonin gene-related peptide (CGRP), vasoactive intestinal peptide (VIP), and acetylcholine (ACh) from the presynaptic vesicle.5
In a recent study, Choi et al. demonstrated through in vivo tests that the mechanism of botulinum toxin in rosacea treatment involves blocking the mast cells degranulation through the soluble N-ethylmaleimide-sensitive factor attachment protein receptor (SNARE) proteins cleavage. Therefore, it proposed that BT targets the rosacea’s neurogenic inflammatory component and also has direct inhibitory effects on mast cells.5 Its effect in reducing the size of noticeable pores has also been reported. Its therapeutic benefit is possibly explained by blocking acetylcholine directed to the hair’s erector muscles, decreasing pore size, and muscarinic receptors located in the sebaceous glands.11
Yuraitis and Jacob published the first report on intradermal BT type A as an effective treatment for facial erythema in 2004.12 The authors reconstituted BT-A with 5 ml of isotonic saline for a final dilution of 2 IU by 0.1 ml. The application was performed at points 1 cm apart, in a total of 10 UI of BT in each treated region. The study observed a satisfactory result within two weeks after application, and the patient returned one month later to continue treatment in other areas. However, not all BT serotypes are effective in treating rosacea. An open, double-blind, split-face study, conducted in 2011 in Korea, aimed to assess BT-B’s effectiveness in treating facial flushing. Fifteen individuals participated in the study, receiving the application of 682 units of BT-B on one side of the face, and saline solution on the other side, as a control. However, after evaluating the erythema index between the two treated sides, the BT-B injection side showed no significant decrease in erythema compared with the control side.13
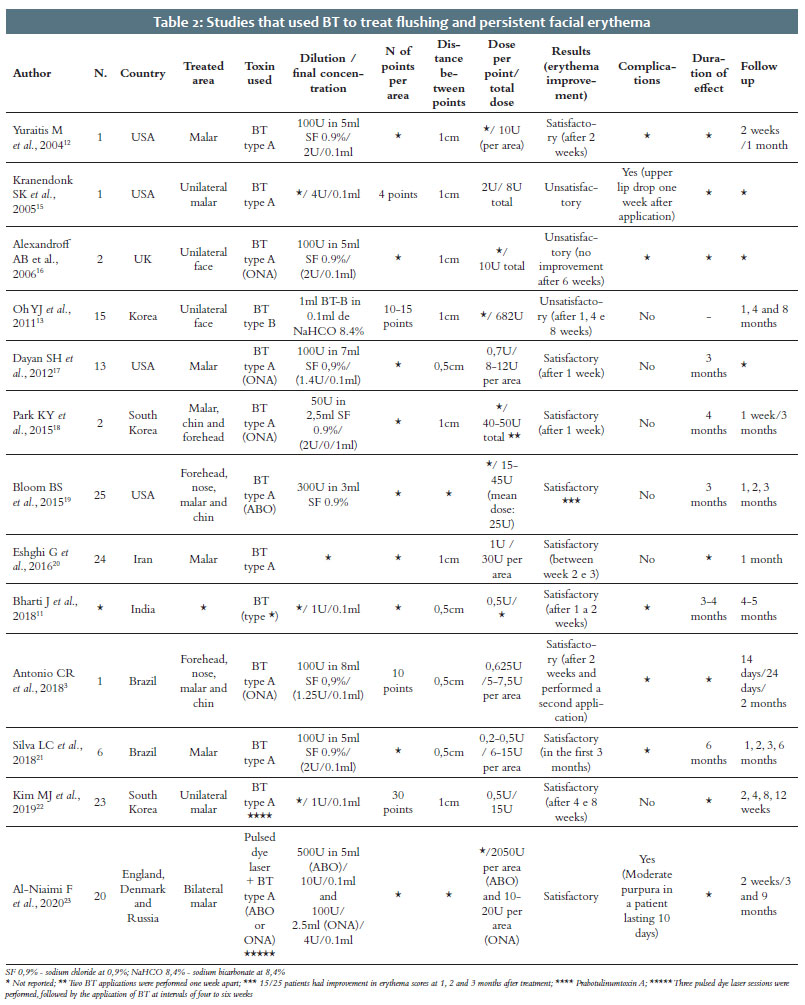
According to the literature, there are no explicit criteria for treatment dilution, dose, and frequency, considering the different presentations of BT and each author’s experience. A 2019 review analyzed 30 articles on the use of BT to treat facial flushing and rosacea. The dose of BT applied ranged from 1 UI to 6 UI for each cm2 of treated area, and the number of sessions varied from 1 to 3 with different time intervals between them. All articles had satisfactory results.14 Table 2 presents a literature review on the studies that used BT to treat flushing and persistent facial erythema with dilutions, doses, complications, duration, follow-up time, and results.3,11-13, 15-23 In the present study, we opted for clinical observation of erythema after exposure to a LED red light mask (with heat emission) to standardize the stimulus since the heat was one of the triggers most reported by patients. Our series found satisfactory results, with few adverse events in the 1:1 BT dilution and a total dose ranging from 25 U to 35 U per patient.
Our limitations include the small sample size, the lack of a control group to compare the results and a long-term follow-up, and the fact that this was an open-label study. More extensive, randomized, blinded, placebo-group studies are needed for standardization and consensus on the ideal dose, technique, and treatment duration.
The intradermal application of BT can be considered a therapeutic alternative to control rosacea’s erythema and facial flushing without a rebound effect or systemic repercussion. There is no consensus in the literature regarding the best dilution, number of points, dose, and frequency of application in these cases. The protocol performed (standard dilution 1:1 [1 U per 0.01ml]) generated good clinical results without significant adverse events.
Jaqueline Barbeito de Vasconcellos 0000-0002-9726-0719
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Isabele Oliveira Santos 0000-0002-2263-3736
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Daniela Alves Pereira Antelo 0000-0001-8203-1772
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Van Zuuren EJ, Fedorowicz Z, Tan J, Van Der Linden MMD, Arents BWM, Carter B, et al. Interventions for rosacea based on the phenotype approach: an updated systematic review including GRADE assessments. Br J Dermatol. 2019;181(1):65–79.
2. Abokwidir M, Feldman SR. Rosacea management. Skin Appendage Disord. 2016;2(1–2):26–34.
3. Antonio CR, Trídico LA, Antonio JR. Tratamento de rosácea com toxina botulínica. Surg Cosmet Dermatol. 2018;10(3):36–9.
4. Schaller M, Almeida LM, Bewley A, Cribier B, Dlova NC, Kautz G, et al. Rosacea treatment update: recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176(2):465–71.
5. Choi JE, Werbel T, Wang Z, Chi Wu C, Yaksh TL, Di Nardo A. Botulinum toxin blocks mast cells and prevents rosacea like inflammation. J Dermatol Sci. 2019;93(1):58-64.
6. Oussedik E, Bourcier M, Tan J. Psychosocial burden and other impacts of rosacea on patients’ Quality of life. Dermatol Clin. 2018;36(2):103–13.
7. Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part II. Topical and systemic therapies in the treatment of rosacea. J Am Acad Dermatol. 2015;72(5):761–70.
8. Steinhoff M, Schmelz M, Schauber J. Facial erythema of rosacea – Aetiology, different pathophysiologies and treatment options. Acta Derm Venereol. 2016;96(5):579–89.
9. Thiboutot D, Anderson R, Cook-Bolden F, Draelos Z, Gallo RL, Granstein RD, et al. Standard management options for rosacea: The 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–10.
10. Schaller M, Almeida LMC, Bewley A, Cribier B, Del Rosso J, Dlova NC, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182(5):1269–76.
11. Bharti J, Sonthalia S, Jakhar D. Mesotherapy with Botulinum toxin for the treatment of refractory vascular and papulopustular rosacea. J Am Acad Dermatol. 2018;19:S0190-9622(18)30808-9.
12. Yuraitis M, Jacob CI. Botulinum toxin for the treatment of facial flushing. Dermatol Surg. 2004;30(1):102–4.
13. Oh YJ, Lee NY, Suh DH, Koh JS, Lee SJ, Shin MK. A split-face study using Botulinum Toxin type B to decrease facial erythema index. J Cosmet Laser Ther. 2011;13(5):243–8.
14. Scala J, Vojvodic A, Vojvodic P, Vlaskovic-Jovicevic T, Peric-Hajzler Z, Matovic D, et al. Botulin toxin use in rosacea and facial flushing treatment. Open Access Maced J Med Sci. 2019;7(18):2985–7.
15. Kranendonk SK, Ferris LK, Obagi S. Re: Botulinum Toxin for the Treatment of Facial. Dermatol Surg. 2005;31(4):491.
16. Alexandroff AB, Sinclair SA, Langtry JA. Letter: Successful use of botulinum toxin a for the treatment of neck and anterior chest wall flushing. Dermatol Surg. 2006;32(12):1536.
17. Dayan SH, Pritzker RN, Arkins JP. A new treatment regimen for rosacea: onabotulinumtoxinA. J Drugs Dermatol. 2012;11(12):e76–9.
18. Park KY, Hyun MY, Jeong SY, Kim BJ, Kim MN, Hong CK. Botulinum toxin for the treatment of refractory erythema and flushing of rosacea. Dermatology. 2015;230(4):299–301.
19. Bloom BS, Payongayong L, Mourin A, Goldberg DJ. Impact of intradermal abobotulinumtoxinA on facial erythema of rosacea. Dermatol Surg. 2015;41:S9–16.
20. Eshghi G, Khezrian L, Alirezaei P. Botulinum toxin-a in treatment of facial flushing. Acta Med Iran. 2016;54(7):454–7.
21. Silva LC, Ferreira ILO, Silveira ML, Steiner D. Estudo prospectivo para tratamento do rubor da rosácea com toxina botulínica tipo A. Surg & Cosmet Dermatol. 2018;10(2):121–6.
22. Kim MJ, Kim JH, Cheon HI, Hur MS, Han SH, Lee YW, et al. Assessment of Skin Physiology Change and Safety After Intradermal Injections With Botulinum Toxin: A Randomized, Double-Blind, Placebo-Controlled, Split-Face Pilot Study in Rosacea Patients With Facial Erythema. Dermatol Surg. 2019;45(9):1155–62.
23. Al-Niaimi F, Glagoleva E, Araviiskaia E. Pulsed dye laser followed by intradermal botulinum toxin type-A in the treatment of rosacea-associated erythema and flushing. Dermatol Ther. 2020;33(6):e13976.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}