


Pedro de Freitas Silva Torraca; Estela Mari Sandini; Tania Christina Marchesi de Freitas
Submitted on: 24/03/2021
Approved on: 22/06/2021
Financial support: none
Conflit of interest: none
How to cite this article: Torraca PFS, Sandini EM, Freitas TCM. Uso de tecnologias a laser e luz intensa pulsada no tratamento da ocronose exógena: uma revisão da literatura. Surg Cosmet Dermatol. 2021;13:e20210002
Exogenous ochronosis is a cutaneous hyperpigmentation condition caused by the accumulation of substances derived from phenol on the skin or mucous membranes without affecting other tissues. It occurs mainly due to the use of bleaching agents, most frequently hydroquinone. The lesions are difficult to treat, being resistant to several approaches. Sometimes it’s necessary to use laser technologies or intense pulsed light to achieve some degree of improvement. The present work consists of a literature review of publications on these technologies in exogenous ochronosis from January 1990 to July 2020.
Keywords: Hyperpigmentation; Intense pulsed light therapy; Lasers; Ochronosis
Exogenous ochronosis (EO) is described as skin and mucous membranes hyperpigmentation caused by phenol-derived substances deposits, most commonly after the use of whitening creams containing hydroquinone, topical resorcinol, or intramuscular or oral antimalarials.1,2,3,4 Contrary to endogenous ochronosis, which arises from homogentisic acid deposition in soft areas and internal tissues, exogenous ochronosis does not affect these sites. EO is considered uncommon:5 it presents a moderate incidence in South Africa,6 with isolated reports in Asia, Africa, and Latin America in patients with Hispanic ancestry and high skin phototypes.7,8,9
Rudolph Virchow named EO in 1865.10,11 Findlay6 related the disease to the use of bleaching cream with hydroquinone in 1975, and Beddard and Plumtre12 associated it to with use of phenol to treat leg ulcers in 1912.12
A recent review of cases in the American literature showed a total of 39 reports of EO in the United States, from January 1983 to June 2020. Of these cases, 18 described the disease onset from the use of whitening creams, and, among these, 14 had hydroquinone in the composition. The concentrations ranged from 2% to 7.5%, with application time from two months to 30 years until the onset of the lesions.2,3,8
Clinically, EO presents as asymptomatic bluish-black or yellow-brown macules, or areas of hyperpigmentation in sun-exposed regions, such as the face, neck, back, extensor zones of the upper limbs, distal portions of the forearms, legs, and dorsum of hands or feet.13 At the histological level, the clinical picture is similar to that of endogenous ochronosis, but with no pigment accumulation in joints, bones, urine, other secretions, or tissues.14,15
For some authors, the condition occurs due to resistance of melanocytes to the effect of whitening agents, with consequent pigment leakage in the papillary dermis and accumulation of this pigment in fibroblasts, resulting in phenols presence in elastotic fibers and their hyperchromia.6 Other authors argue that hydroquinone is oxidized to quinone forming hydroxylated indoles similar to melanin precursors.16 A third group believes that high hydroquinone concentrations stimulate melanocytes to produce more melanin.17 However, the most widely accepted theory is that hyperpigmentation results from homogentisic acid oxidase enzyme inhibition by hydroquinone, causing local homogentisic acid accumulation. The homogentisic acid then polymerizes, forming an ocher pigment in the papillary dermis, as occurs in other tissues in cases of endogenous ochronosis due to a primary structural defect of this enzyme.18
Exogenous ochronosis lesions observed in dermoscopy were initially described in 200819,20 as sites of blue-gray or brown to black, amorphous globules, with follicular obliteration areas. It contrasts with melasma cases where dermoscopy demonstrates a pattern of reticular pigmentation, pseudonet accentuation, and brownish granules and globules, sparing the follicles.21
At the histological level, the lesions show collagen fibers with a yellow-brownish color in a “banana shape”, degradation of these fibers, and formation of colloid milium amid an inflammatory infiltrate with plasma cells, histiocytes, and multinucleated giant cells in the development of the lesions.16,22
In 1979, Dogliotti and Leibowitz classified the clinical stages of exogenous ochronosis into stage I (lesions with erythema and some pigmentation); stage II (injuries presenting hyperpigmentation, hyperpigmented colloid milium, atrophy); and stage III (presence of papulonodular eruptive elements in a lesion with stage II features plus inflammatory characteristics in more recent wounds that are less pronounced in older injuries).23 In 1986, Phillips et al. classified ochronosis as mild, moderate, and severe in a series of 395 cases in patients assessed by the Dermatology Service of a hospital in Johannesburg, South Africa, during one year. Only lesions with altered skin hyperpigmentation and hypertrophy were considered as mild; presence of hyperchromic papules was the standard for moderate degree; and lesions with hyperchromic caviar-like papules, coalescent in plaques, were deemed as severe.8 In a third classification, in 1989, Hardwick et al. considered five grades of presentation: grade 1 comprised lesions with hyperchromic macules; grade 2, with macules and micropapules; grade 3 included injuries with darkened deposits and larger papules; grade 4, with colloid milium of 1 mm or more; and grade 5 encompassed lesions with keloid nodules and hyperchromic cysts.24
According to the European Society of Laser Dermatology (ESLD), the exogenous ochronosis treatment is challenging, with unpredictable results, often below expectations. The use of photoprotection becomes a relevant element in the initial approach by slowing the progression of the lesions and preventing the emergence of new hyperpigmented areas.15 Some cases achieved a partial response with topical retinoic and glycolic acid in low concentrations and oral use of tetracycline in papular presentations or with sarcoidosis-like lesions.25 In a recent review on the use of these technologies, the ESLD recommends such therapies associated with multiple laser technologies sessions, combining fractional ablative modalities such as CO2 or Erbium 2940nm with Q-Switched 1064nm for better and faster results.26,15
The present study reviews publications containing a therapeutic approach to exogenous ochronosis conditions using laser technologies or intense pulsed light, demonstrating the described protocols and results obtained from 1990 to July 2020.
Four databases were searched from June 15 to August 5, 2020: Embase, MEDLINE/Pubmed, LILACS, and Cochrane Library. The selected languages were English, Spanish, and Portuguese. In the first stage, the keywords used were chronosis, exogenous ochronosis, ocronose, and ocronosis. They generated a total of 1,377 results in the Embase platform, 978 in the MEDLINE/Pubmed, 32 in the LILACS, and 16 results in the Cochrane Library platform.
After this stage, the terms treatment, therapy, tratamento, tratamiento, efficacy, upade laser and intense pulsed light were included in the search. The results with crossings between these keywords obtained 79 results in the Embase platform, 19 in the MEDLINE/Pubmed, two in the LILACS, and one result in the Cochrane Library platform. Considering the objectives of the review, we selected studies that cited the use of laser technologies and intense pulsed light to treat exogenous ochronosis conditions published from January 1990 to July 2020.
Thus, the selection criteria were scientific articles on exogenous ochronosis regardless of its cause, approached with the use of laser or intense pulsed light at some point in the therapy. Studies on other pathologies, other ochronosis forms, or other therapies that did not address the use of lasers or intense pulsed light were excluded. The entire method of research and selection of articles containing the terms described was repeated by a secondary researcher, following the same methodology, generating the same data and articles.
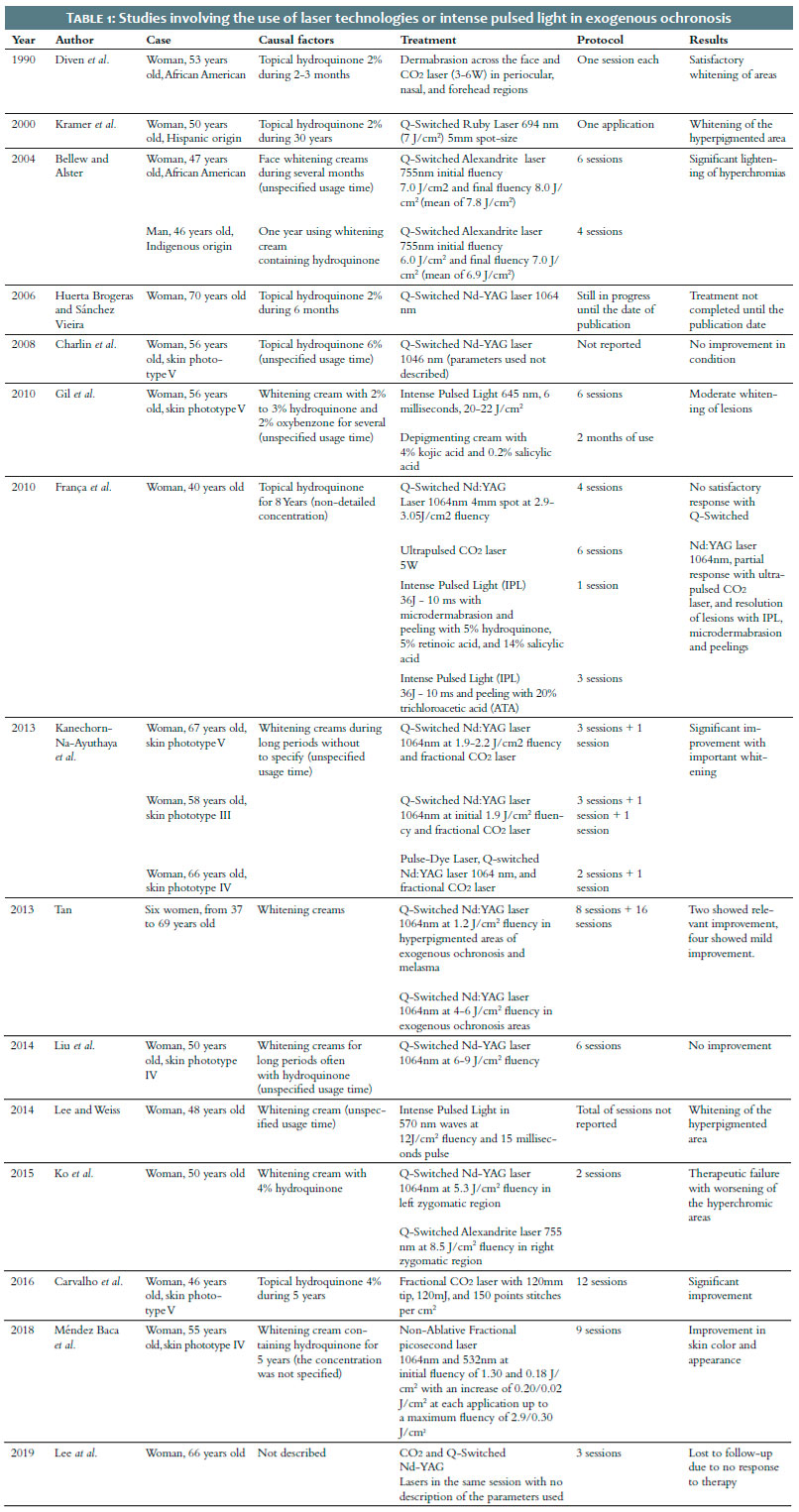
Among several therapeutic modalities, lasers are considered excellent options to treat hyperpigmented lesions, promoting selective photothermolysis of pigments.27 The most used lasers for this purpose are Q-Switched Ruby (QSRL), Q-Switched Alexandrite 755nm, Q-Switched Nd:YAG 1064nm, Q-Switched Nd:YAG 532nm, picosecond lasers,28,29 and intense pulsed light with specific filters.30 Technologies such as non-ablative Erbium-Glass 1550nm laser, ablative Erbium:YAG 2940nm,31 CO2 laser 10600nm,32 and Thulium laser 1927nm33 use water as a chromophore and can be alternatives both in pigments vaporization and in facilitating depigmenting agents penetration. In 2015, a review on therapeutic modalities in exogenous ochronosis cases was published. The main technologies used for this purpose were Q-Switched Ruby (694nm), Q-Switched Alexandrite (755nm), Q-Switched Nd:YAG (1064nm), CO2 lasers, and intense pulsed light.1 Only recently the picosecond laser was also reported as an option for treating hyperpigmented lesions (Table 1).34,35,36
In 1990, Diven et al. reported a case of exogenous ochronosis in the face of a 53-year-old African-American woman treated with dermabrasion and CO2 laser. It resulted in the first description of the use of laser technologies to approach ochronosis. After using 2% hydroquinone cream for two to three months, the patient had progressive darkening of the area. Approach attempts with tretinoin 0.025% topical gel, cryotherapy, and peeling with ATA 50% did not achieve improvement. Therefore, we opted for dermabrasion of the whole face, followed by CO2 3-6W application in defocused irradiation mode in the periocular regions, nose, and forehead, obtaining satisfactory results.32
Ten years later, Kramer et al. reported an exogenous ochronosis case treated with laser technology in bilateral zygomatic arch in a 50-year-old woman of Hispanic origin. At the time, the patient mentioned the use of 2% hydroquinone cream in the area for 30 years to treat melasma. Exogenous ochronosis was diagnosed histologically with yellow to brown pigment deposits and collagen fibers degeneration in the dermis, in addition to sparse lymphocytic infiltrate. The authors used a Q-Switched Ruby laser 694nm (7J/cm2), 5mm spot size. The patient reported improvement in the condition after the session.37
Elizabeth Arnold Spenceri, in a publication on Pigmentation Disorders in 2003, summarized as the main exogenous ochronosis treatment the discontinuation of the triggering factor and application of Q-Switched laser in refractory cases.38 In the following year, Bellew and Alster treated two exogenous ochronosis cases with Q-Switched Alexandrite laser 755nm. The first was a 47-year-old African-American woman with a history of hyperchromic lesions on the face for eight years, which worsened after using whitening creams in the area for several months, without specifying the period of time. The second was a 46-year-old man of indigenous origin presenting hyperchromic macules on the face for seven years, which worsened after using a bleaching cream containing hydroquinone for a year. In the first patient, the lesions were initially addressed with Q-Switched Alexandrite 755nm at 7 J/cm2 fluency, 3 mm spots, every 15 days, with an increase in fluency up to 8 J/cm2 (mean of 7.8 J/cm2). The whitening was achieved after six sessions. In the second patient, the initial fluency was 6 J/cm2 and the final fluency was 7 J/cm2 (mean of 6.9 J/cm2), totaling four sessions. There was a four-month interval for the resolution of post-inflammatory hyperpigmentation, considering the high sun exposure reported by the patient. The authors reported significant improvement of the lesions in both cases, with significant lightening.39
In 2006, Huerta Brogeras and Sanchés-Vieira presented the case of a 70-year-old woman with a history of melasma on the face and the use of 2% hydroquinone bleaching cream for six months, who had hyperpigmentation in the bilateral malar region and eyelids. Anatomopathological examination of the hyperpigmented area showed deposition of yellow-brown globules in the dermis, confirming the diagnosis of exogenous ochronosis. The authors used a Q-Switched Nd:YAG 1064nm laser for the treatment, with sessions still in progress at the date of publication of the report.40
Two years later, Charlín et al. published four cases of exogenous ochronosis triggered by topical use of hydroquinone for melasma. In one of the cases, the patient was a 56-year-old woman, with skin phototype V and melasma for 25 years, treated with 6% hydroquinone without specifying the duration of use. In this case, other topical medications were not reported, and the patient presented darkening of almost the entire face, except for the upper region of the lips and forehead. Therapeutic testing was performed with a Q-Switched Nd:YAG laser 1046nm, with no improvement. The authors do not describe the parameters used or the application protocol.19
Gil et al., in 2010, reported a case of exogenous ochronosis in a 63-year-old woman, with skin phototype V, developed after using a whitening cream with 2% to 3% hydroquinone and 2% oxybenzone for several years, without specifying the duration of use. The diagnosis was confirmed histologically by the presence of yellow-brown material deposits in the papillary and medial dermis. She was treated with intense pulsed light 645nm, six milliseconds, 20-22J/cm2, associated with depigmenting cream with 4% kojic acid and 0.2% salicylic acid. Moderate lightening of the lesions was achieved after two months of topical use and six sessions of intense pulsed light.41
Also in 2010, França et al. described an exogenous ochronosis case in a 40-year-old woman with hyperchromic macules and papules in the malar region and a history of topical hydroquinone use for eight years (the study did not describe the concentration). A histopathological examination revealed yellow-brown filaments in the papillary dermis, and investigation of deposits in other tissues was negative, ruling out an endogenous picture. In this report, the approach started with four sessions of Q-Switched Nd:YAG 1064nm laser, 4 mm spot, and 2.9-3.05 J/cm2 fluency, without satisfactory response. Then, the authors opted for six sessions of ultrapulsed CO2 laser, with one-month interval between each session, at 5W fluency, reaching some response. Finally, intense pulsed light (IPL) 36 J-10 ms was associated with the therapy, applied to the malar area, followed by microdermabrasion and chemical peeling with 5% hydroquinone, 5% retinoic acid, and 14% salicylic acid. The lesions resolved only after three more sessions, with intervals of 30 days of intense pulsed light (IPL) 36 J-10 ms and trichloroacetic acid (ATA) 20% peeling.13
Kanechorn-Na-Ayuthaya et al., in 2013, assessed the use of the combination of Q-Switched Nd:YAG and fractional CO2 laser to treat exogenous ochronosis. They applied these modalities in three cases. The first was a 67-year-old woman, skin phototype V, with a history of face melasma for 28 years and use of whitening cream for long periods (the time has not been determined), presenting darkening of the malar and zygomatic areas. She received three sessions of Q-Switched Nd:YAG 1064nm at 1.9-2.2 J/cm2 fluency and one session of fractional CO2 laser, totaling four months of applications. The second patient was a 58-year-old woman, skin phototype III, with a history of recalcitrant melasma for 28 years and long-term use of hydroquinone bleaching cream, presenting hyperchromia in the temporal, malar, eyelid, and perilabial regions. For the treatment, she also received three applications of Q-Switched Nd:YAG 1064nm laser every 30 days, with an initial fluency of 1.9 J/cm2 progressively increasing in multiple passes until the appearance of petechiae or purpura. After the third application, a CO2 laser was performed only once at the end of four months of treatment. Three months later, pulse-dye laser was applied for telangiectasias in the areas. The third case described was a 66-year-old woman, skin phototype IV, with a history of melasma for 20 years. She used whitening creams and complaint of bilateral darkening of the malar region. In this case, a Q-Switched Nd:YAG laser 1064nm was used in two sessions with a 30-day interval, resulting in purpura after each application. Fractioned CO2 laser was performed after the second Q-Switched session. All the cases showed significant skin improvement, with lightening of hyperchromic lesions and skin rejuvenation with enhancement of telangiectasias.26
In the same year, Tan described six cases of exogenous ochronosis successfully treated after sessions of Q-Switched Nd:YAG 1064nm. Six women aged between 37 and 69 years, with a history of melasma and the use of whitening creams, two of them containing hydroquinone, presented hyperchromia in the application areas. The diagnosis was confirmed with histopathological examination, and the conditions were classified according to the ochronosis staging method described by Dogliotti and Leibowitz: stage I, lesions with erythema and some pigmentation; stage II, lesions with hyperpigmentation, hyperpigmented colloid milium, and atrophy; and stage III, papulonodular eruptive elements in a lesion with stage II characteristics.23 Four of the patients had stage I EO; one, stage II; and one, stage III. The cases were treated with a Q-Switched Nd:YAG 1064nm laser at 1.2 J/cm2 fluency, 8 mm spot size, in four passes in the hyperpigmented areas, which included lesions of exogenous ochronosis and melasma. Subsequently, only areas considered as having exogenous ochronosis received new applications at 4-6 J/cm2 fluency, 4 mm spot size, with two or three applications in stacks in each macula until the appearance of erythema or petechiae. Stage II and III patients showed significant improvement in areas of exogenous ochronosis after eight and 16 sessions, respectively. Nevertheless, stage I patients had no resolution of the lesions, but slight improvement in color after treatment.42
In 2014, Liu et al. reported an exogenous ochronosis case in a 50-year-old woman, skin phototype IV, with a history of hyperchromic macules in malar areas. She was treated with whitening creams for long periods, often with hydroquinone, in different concentrations, which had been darkening for one year of the description, even with adequate photoprotection. The dermoscopy showed areas with sparse blue-gray dots and globules, and homogeneous follicular ostia obliteration. Histological examination revealed dilated and basophilic collagen fibers, fragmented and with ocher pigmentation. Exogenous ochronosis was classified as Dogliotti stage II, and the patient received six sessions of Q-Switched Nd:YAG 1064nm laser with 6-9 J/cm2 fluency, with no improvement.43
Also in 2014, Lee and Weiss presented an exogenous ochronosis case in a 48-year-old woman, after years of using a bleaching cream for facial dyschromia. Intense pulsed light in waves of 570nm was used for the treatment, at 12 J/cm2 fluency, 15 milliseconds pulse, with sessions every six weeks, without description of the total number of sessions. The authors observed whitening of the maculae since the first application.44 The following year, Ko and Wang reported exogenous ochronosis in a 50-year-old woman after using a whitening cream containing 4% hydroquinone. Therapeutic response test was performed using Q-Switched Nd:YAG laser 1064nm at 5.3 J/cm2 fluency, 3 mm spot size, in the left zygomatic region, and Q-Switched Alexandrite laser 755nm at 8.5 J/cm2 fluency, 3 mm spot size, in the right zygomatic region. After two applications with a 5-week interval, both areas showed darkening, indicating therapeutic failure.45
In 2016, Carvalho et al. described ochronosis lesions like hyperchromic papules and macules on the forehead, nasal dorsum, and malar regions of a 46-year-old woman, skin phototype V, using topical 4% hydroquinone for five years to treat melasma on the face. After ruling out endogenous ochronosis due to the absence of pigmentary deposits in other tissues, joint pain, and urinary alterations, the application of fractional CO2 laser was started on the entire face, using a 120 mm tip, 120 mJ energy, and 150 points per cm2 density, in monthly sessions for one year, totaling 12 applications and reaching significant improvement of the condition.46
Méndez Baca et al., in 2018, depicted the case of a 55-year-old woman, skin phototype IV, with exogenous ochronosis lesions in the bilateral malar region, reporting the appearance of blue-gray macules in the area after applying bleaching cream containing hydroquinone for five years to treat hyperpigmented lesions. The condition had been previously approached with intense pulsed light associated with depigmenting agents with 4% hydroquinone, kojic acid, phytic acid, ferulic acid, citric acid, as well as topical pimecrolimus and sunscreens, without improvement. It was then decided to use a fractionated non-ablative picosecond laser 1064nm and 532nm, at an initial 1.30-0.18 J/cm2 fluency, with an increase of 0.20/0.02 J/cm2 each session, up to a maximum 2.9/0.30 J/cm2 fluency. The sessions occurred every two months, with applications until obtaining uniform facial erythema. After nine sessions, there was an improvement in skin color and texture.47
In 2019, Lee et al. reported an exogenous ochronosis case in a 66-year-old woman with hyperpigmented perilabial and scleral lesions for one year. Skin lesions were treated with CO2 laser and Q-Switched Nd:YAG in the same session, without description of the parameters used. After three applications, the patient was lost to follow-up due to lack of response.48
Despite the extensive use of hydroquinone bleaching agents in Dermatology, reports of exogenous ochronosis are infrequent. The difficulty in treating hyperchromic lesions reinforces the need for multiple therapeutic approaches to reach satisfactory results. In this context, the use of lasers or light therapies can be a promising alternative. However, there are several types of technologies used without a specific protocol.
The vast majority of studies on the topic refer to isolated cases of the use of lasers or different light technologies, without respecting standardization both in the clinical evaluation of the response and in the selected modalities. The need for population studies considering a larger number of cases, assessment standardization, exogenous ochronosis lesions and treatment classification, becomes, therefore, crucial for further clarification.
Pedro de Freitas Silva Torraca 0000-0002-8417-0685
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Estela Mari Sandini 0000-0002-2362-396X
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Tania Christina Marchesi de Freitas 0000-0002-5609-5884
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
1. Simmons BJ, Griffith RD, Bray FN, Falto-Aizpurua LA, Nouri K. Exogenous ochronosis: a comprehensive review of the diagnosis, epidemiology, causes, and treatments. Am J Clin Dermatol. 2015;16(3):205-12.
2. Qorbani A, Mubasher A, Sarantopoulos GP, Nelson S, Fung MA. Exogenous Ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10(4):e2020197.
3. Martins VMR, Sousa ARD, Portela NC, Tigre CAF, Goncalves LMS, Castro Filho RJL. Exogenous ochronosis: case report and literature review. An Bras Dermatol. 2012;87(4):633-6.
4. Zawar VP, Mhaskar ST. Exogenous ochronosis following hydroquinone for melasma. J Cosmet Dermatol. 2004;3(4):234-6.
5. Levitt J. The safety of hydroquinone: a dermatologist's response to the 2006 Federal Register. J Am Acad Dematol. 2007;57(5):854-872.
6. Findlay GH, Morrison JG, Simson IW. Exogenous ochronosis and pigmented colloid milium from hydroquinone bleaching creams. Br J Dermatol. 1975;93(6):613-22.
7. Bhattar PA, Zawar VP, Godse KV, Patil SP, Nadkarni NJ, Gautam MM, et al. Exogenous ochronosis. Indian J Dermatol. 2015;60(6):537-43.
8. Phillips JI, Isaacson C, Carman H. Ochronosis in black South Africans who used skin lighteners. Am J Dermatopathol. 1986;8(1):14-21.
9. Findlay GH, Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57(6):187-90.
10. Findlay GH. Ochronosis. Clin Dermatol. 1989;7(2):28-35.
11. Laymon CW. Ochronosis. AMA Arch Derm Syphilol. 1953;67(6):553-60.
12. Beddard AP, Plumtre CM. A further note on ochronosis associated with carboluria. QJM. 1912;5(4):35-7.
13. Franca ER, Paiva V, Toscano LPN, Nunes GJB, Rodrigues TFA. Exogenous ochronosis: a case report. Surg Cosmet Dermatol. 2010;2(4):319-21.
14. Zawar V, Tan SK. Exogenous ochronosis: a review for clinicians. Expert Rev Dermatol. 2012;7(2):171-80.
15. Passeron T, Genedy R, Salah L, Fusade T, Kositratna G, Laubach HJ, et al. Laser treatment of hyperpigmented lesions: position statement of the European Society of Laser in Dermatology. J Eur Acad Dermatol Vene-reol. 2019;33(6):987-1005.
16. Cullison D, Abele DC, Quinn JL. Localized exogenous ochronosis: report of a case and review of the literature. J Am Acad Dermatol. 1983;8(6):882-9.
17. Engasser PG. Ochronosis caused by bleaching creams. J Am Acad Dermatol. 1984;10(6):1072-3.
18. Penneys NS. Ochronosislike pigmentation from hydroquinone bleaching creams. Arch Dermatol. 1985;121(10):1239-40.
19. Charlin R, Barcaui CB, Kac BK, Soares DB, Rabello-Fonseca R, Azulay-Abu-lafia L. Hydroquinone-induced exogenous ochronosis: a report of four cases and usefulness of dermoscopy. Int J Dermatol. 2008;47(1):19-23.
20. Romero SA, Pereira PM, Mariano AV, Francesconi F, Francesconi VA. Use of dermoscopy for diagnosis of exogenous ochronosis. An Bras Dermatol. 2011;86(Suppl 1):S31-4.
21. Khunger N, Kandhari R. Dermoscopic criteria for differentiating exogenous ochronosis from melasma. Indian J Dermatol Venereol Leprol. 2013;79(6):819-21.
22. Levin CY, Maibach H. Exogenous ochronosis. An update on clinical features, causative agents and treatment options. Am J Clin Dermatol. 2001;2(4):213-7.
23. Dogliotti M, Leibowitz M. Granulomatous ochronosis - cosmetic induced skin disorder in blacks. S Afr Med J. 1979;56(19):757-60.
24. Hardwick N, Van Gelder LW, Van der Merwe CA et al. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120(2):229-38.
25. Fisher AA. Tetracycline treatment for sarcoid-like ochronosis due to hydroquinone. Cutis. 1988;42(1):19-20.
26. Kanechorn-Na-Ayuthaya P, Niumphradit N, Aunhachoke K, Nakakes A, Sittiwangkul R, Srisuttiyakorn C. Effect of combination of 1064 nm Q-s-witched Nd:YAG and fractional carbon dioxide lasers for treating exogenous ochronosis. J Cosmet Laser Ther. 2013;15(1):42-5.
27. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220(4596):524-7.
28. Chan JC, Shek SY, Kono T, Yeung CK, Chan HH. A retrospective analysis on the management of pigmented lesions using a picosecond 755-nm alexandrite laser in Asians. Lasers Surg Med. 2016;48(1):23-9.
29. Levin MK, Ng E, Bae YS, Brauer JA, Geronemus RG. Treatment of pigmentary disorders in patients with skin of color with a novel 755 nm picosecond, Q-switched ruby, and Q-switched Nd:YAG nanosecond lasers: a retrospective photographic review. Lasers Surg Med. 2016;48(2):181-7.
30. Pimentel CL, Rodriguez-Salido MJ. Pigmentation due to stasis dermatitis treated successfully with a noncoherent intense pulsed light source. Dermatol Surg. 2008;34(7):950-1.
31. Badawi AM, Osman MA. Fractional erbium-doped yttrium aluminum garnet laser-assisted drug delivery of hydroquinone in the treatment of melasma. Clin Cosmet Investig Dermatol. 2018;11:13-20.
32. Diven DG, Smith EB, Pupo RA, Lee M. Hydroquinone-induced localized exogenous ochronosis treated with dermabrasion and CO2 laser. J Dermatol Surg Oncol. 1990;16(11):1018-22.
33. Niwa Massaki AB, Eimpunth S, Fabi SG, Guiha I, Groff W, Fitzpatrick R. Treatment of melasma with the 1,927-nm fractional thulium fiber laser: a retrospective analysis of 20 cases with long-term follow-up. Lasers Surg Med. 2013;45(2):95-101.
34. Levin MK, Ng E, Bae Y-SC, Brauer JA, Geronemus RG. Treatment of pigmentary disorders in patients with skin of color with a novel 755 nm picosecond, Q-switched ruby, and Q-switched Nd:YAG nanosecond lasers: a retrospective photographic review. Lasers Surg Med. 2016;48(2):181-7.
35. Lipp MB, Angra K, Wu DC. Safety and efficacy of a novel 730 nm picosecond titanium sapphire laser for the treatment of benign pigmented lesions. Lasers Surg Med. 2021;53(4):429-34.
36. Vanaman Wilson MJ, Alkhonizi S, Wu DC. Successful treatment of under-eye pigmentation in skin type IV with a picosecond alexandrite laser with diffractive lens array. Dermatol Surg. 2017;43(8):1095-7.
37. Kramer KE, Lopez A, Stefanato CM, Phillips TJ. Exogenous ochronosis. J Am Acad Dermatol. 2000;42(5 Pt 2):869-71.
38. Spenceri EA. Disorders of pigmentation. Facial Plast Surg Clin North Am. 2003;11(2):209-17.
39. Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-swit-ched alexandrite (755 nm) laser. Dermatol Surg. 2004;30(4 Pt 1):555-8.
40. Huerta Brogeras M, Sanchez-Viera M. Exogenous ochronosis. J Drugs Dermatol. 2006;5(1):80-1.
41. Gil I, Segura S, Martinez-Escala E, Lloreta J, Puig S, Velez M, et al. Dermoscopic and reflectance confocal microscopic features of exogenous ochronosis. Arch Dermatol. 2010;146(9):1021-5.
42. Tan SK. Exogenous ochronosis: successful outcome after treatment with Q-switched Nd:YAG laser. J Cosmet Laser Ther. 2013;15(5):274-8.
43. Liu WC, Tey HL, Lee JS, Goh BK. Exogenous ochronosis in a Chinese patient: use of dermoscopy aids early diagnosis and selection of biopsy site. Singapore Med J. 2014;55(1):e1-3.
44. Lee MD, Weiss E. Treatment of exogenous ochronosis with advanced fluorescence technology. Dermatol Surg. 2014;40(9):1046-8.
45. Ko WL, Wang KH. Exogenous ochronosis. Dermatol Sin. 2015;33(1):29-30.
46. Carvalho CGS, Vilela VN, Rocha AEA, Carvalho GSM, Franca ER, Rodrigues AGA. Exogenous ochronosis treated with CO2 Laser. Surg Cosmet Dermatol. 2016;8(4):370-2.
47. Mendez Baca I, Al-Niaimi F, Colina C, Anuzita A. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. Epub 2018 Dec 16.
48. Lee MY, Yun SJ, Lee SC, Won YH, Lee JB. A case of ochronosis with atypical manifestations involving the perioral area and sclera. Ann Dermatol. 2019;31(1):106-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}