


Magda Blessmann Weber1; Iago Gonçalves Ferreira1; Laura Oliveira Ferreira1; Anna Bittarello Silva1; Selma Schuartz Cernea2
Submitted on: 10/02/2021
Approved on: 04/04/2021
Financial support: None
Conflict of interest: None
How to cite this article: Weber MB, Ferreira IG, Ferreira LO, Silva AB, Cernea SS. Advanced squamous cell carcinoma and immunotherapy: new therapeutic perspectives. Surg Cosmet Dermatol. 2021;13:e20210023.
Squamous cell carcinoma (SCC) has the second highest incidence rate among non-melanoma skin cancers. About 5% of cases progress to locally advanced and/or metastatic lesions, making the surgical approach often unfeasible. Based on this, we performed a literature review on the use of immunotherapy drugs to treat advanced SCC. The results showed that immunotherapy is a potential therapeutic strategy due to the antitumor activity promotion through the individual immune response, reducing the adverse events of surgeries, chemotherapy, and radiotherapy
Keywords: Squamous cell carcinoma; Tumor Evasion; Immunotherapy; Skin neoplasms
Non-melanoma skin cancers (NMSCs) represent one of the most prevalent groups of malignancies in the world. Worldwide, an estimated 18 million new cancer cases occurred in 2018, causing around 100,000 deaths. Of these, approximately 1 million were NMSCs.1-3 In Brazil, the National Cancer Institute estimates near 625,000 cancer cases in the country, of which 177,000 are NMSCs. Thus, this is the group of malignant neoplasms with the highest incidence.3
NMSCs include several malignant neoplasms, including basal cell carcinoma (BCC), the most common skin cancer, and squamous cell carcinoma (SCC), the second most frequent skin malignancy.3 BCCs and SCCs originate from the neoplastic proliferation of epidermal keratinocytes exposed to carcinogenic factors, including exposure to ultraviolet (UV) radiation, chron-ic immunosuppression, burn scars, contact to ionizing radiation, among others.1,2
UV radiation stands out among the carcinogenic factors. It is recognized for its high mutagenic potential, providing BCCs and SCCs with the highest mutation load among all types of cancer. However, SCCs are a matter of greater concern given their more aggressive behavior: about 5% of cases evolve to locally advanced or metastatic conditions, with uncontrollable growth and substantial disfigurement.4-6
Regarding treatment, early surgical excision is considered the therapeutic option of choice, allowing the tumor type confirmation, histological differentiation degree, and free margins analysis. Nevertheless, some SCC cases are diagnosed in elderly patients with comorbidities that limit the adoption of more invasive therapeutic alternatives.5,6 The tumors’ location and size can also restrict surgical therapies, such as lesions with a diameter greater than 20 mm in periocular, auricular, labial, and temporal regions, as well as in cases of metastatic diseases.7,8
Locally advanced cutaneous SCC represents a significant therapeutic challenge. For unresectable, unsuitable for radiotherapy SCC, standard systemic treatment options include chemotherapy (usually platinum or fluoropyrimidine-based) or targeted therapy with epidermal growth factor receptor in-hibitors.6 The responses often have a short life and may be associated with significant adverse events in an elderly and frail population.
Despite the relevance of the surgical approach in ad-vanced SCCs, cases of greater clinical complexity can adopt therapeutic alternatives. These alternatives include radiotherapy and chemotherapy with cisplatin, 5-fluorouracil, paclitaxel, and methotrexate (often used in inoperable and advanced lesions).5,6
Improved understanding of the immunological con-trol mechanisms involved in skin cancer pathogenesis led to the development of specific immunotherapeutic treatments to promote antitumor activity. In this sense, immunotherapy provides individualized treatment to patients, with minimal adverse events, as it acts in the tumor microenvironment through molecular and cellular mechanisms.9,10
Given the new therapeutic approach proposed by im-munotherapy for malignant skin neoplasms, this study aimed to conduct an integrative review of immunotherapy drugs to treat advanced squamous cell carcinomas and/or in patients with comorbidities that limit other therapies.
The study aimed to overview the current scientific production on the use of immunomodulators to treat advanced cutaneous squamous cell carcinoma and/or in patients with co-morbidities that limit conventional therapies. It adopted the integrative review as a research method. Integrative reviews consist of research methods that aim to provide a synthesis of knowledge about a particular subject or field to integrate concepts, ideas, and results from original and/or secondary studies.11,12
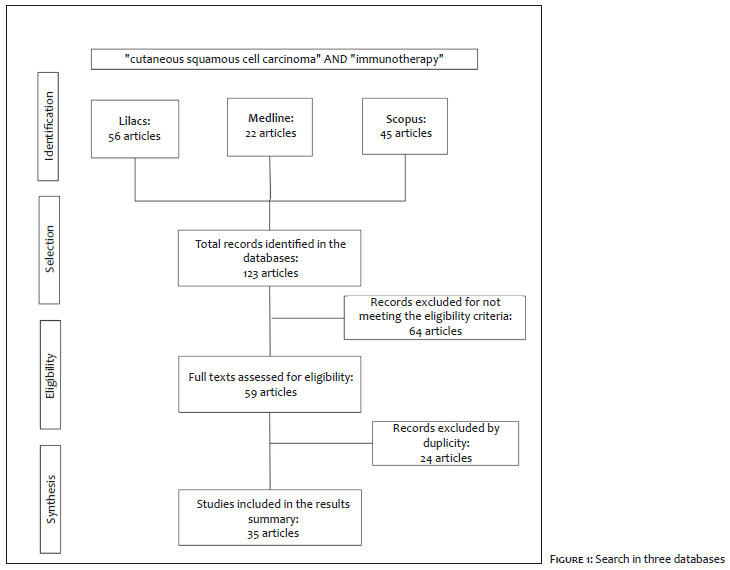
We conducted the literature review in three databases: Medline (Medical Literature Analysis and Retrieval System Online), Lilacs (Latin American and Caribbean Center on Health Sciences Information), and Scopus (SciVerse Scopus - Elsevier) adopting as search strategy the keywords: “cutaneous squamous cell carcinoma” AND “immunotherapy”. The search used the fil-ters “10 years” - to select studies published from 2010 to 2020 — and “full text” — to retrieve articles with the full version available.
From the results obtained with the search strategy, we started the article selection process, using as inclusion criteria studies on the use of immunomodulators to treat cutaneous squamous cell carcinoma (SCC), with text in Portuguese or English available, and primary focus related to cutaneous im-munology in SCCs and/or the use of immunotherapy drugs in SCC treatment. The exclusion criteria adopted were: studies addressing SCC systemic treatments generically or broadly, with full texts not available, and relating immunotherapeutic treat-ment with other therapeutic alternatives. Such standards aimed to allow the data synthesis to be more targeted and specific to the study objectives.
We assessed the selected studies separately, dividing them into two thematic areas: “Immune system and immunotherapy in cutaneous squamous cell carcinoma” and “Immunotherapy drugs in cutaneous squamous cell carcinoma”. Then, the articles’ contents were analyzed and summarized through a conceptual synthesis.
The search in the databases identified a total of 123 publications. The titles and abstracts preliminary assessment through eligibility criteria allowed the selection of 59 studies, from which 24 were excluded due to duplicity. Thus, 35 publications comprised the sample analyzed in the review and conceptual synthesis (Figure 1).
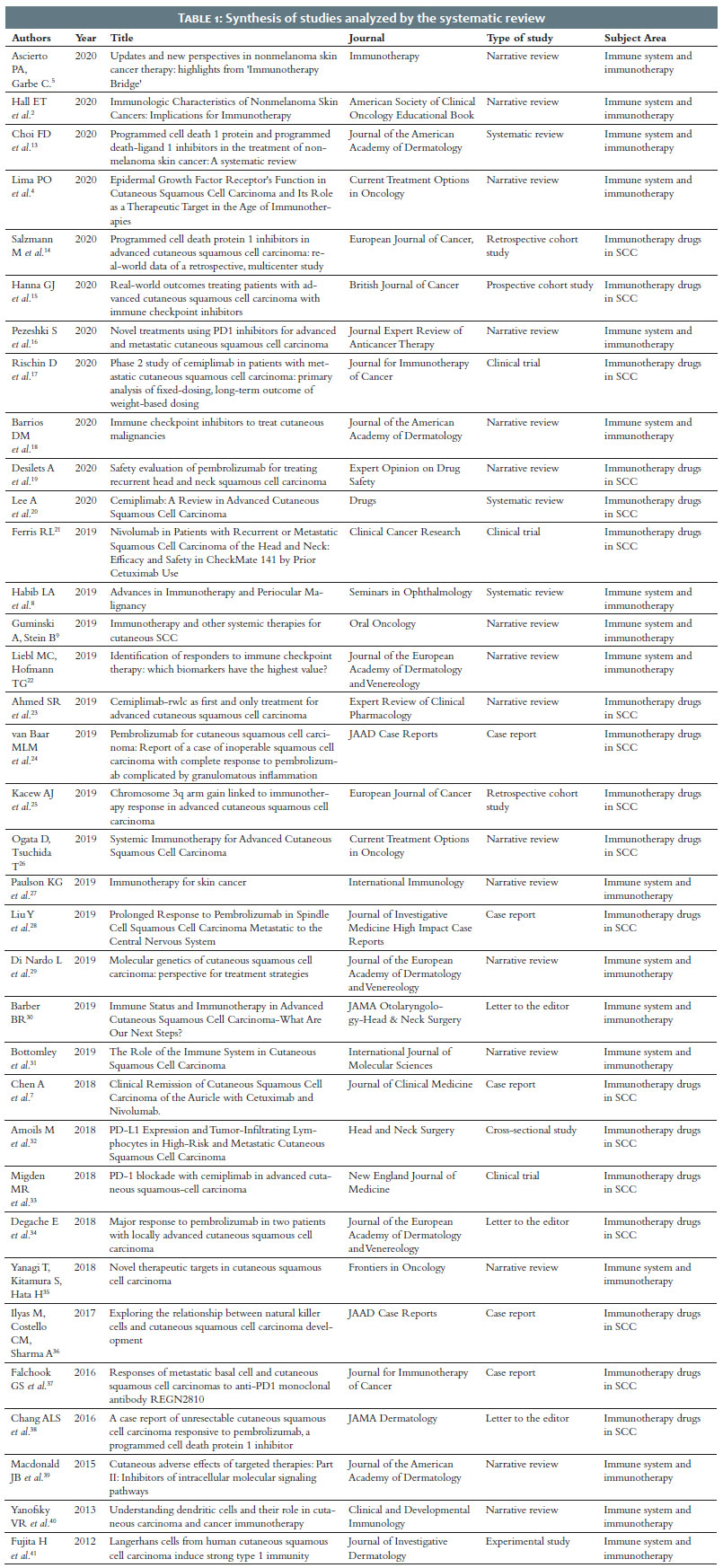
We distributed the assessed studies in two thematic areas: 17 studies in “Immune system and immunotherapy in cutaneous squamous cell carcinoma” and 18 studies in “Immunotherapy drugs in cutaneous squamous cell carcinomas”. Most of these
studies were composed of narrative reviews (16 articles) and case reports (five studies), and the year 2019 had the highest number of publications, with 13 studies (Table 1).
Cutaneous squamous cell carcinoma (SCC) is the sec-ond most frequent among non-melanoma skin cancers (NMSC). More than 90% of SCCs have a favorable prognosis, and early surgical treatment can cure it through the excision of the lesions. However, the disease progresses locally in about 4-5% of cases, becoming unresectable and/or metastatic and requiring alternative therapeutic approaches such as radiotherapy, chemotherapy, and, more recently, immunotherapy.5,18,31
The use of immunomodulators to treat squamous cell carcinomas is based on the ability of the immune system to control the carcinogenesis process.39 The high NMSC incidence among immunocompromised individuals, such as in HIV infection cases, or immunosuppressed patients, condition of solid organ transplant recipients, supports this perspective. Thus, the immunological surveillance role to control neoplasms is highlighted, making it relevant to understand the relationship between the immune system and cutaneous carcinogenesis.2 The immune system and skin cancers
The skin plays essential roles in the homeostasis of the human body, acting to maintain body temperature, protect against environmental agents (physical and chemical), and produce nervous and endocrine stimuli, in addition to working in the body’s immune defense. Such defense can occur in the form of innate immunity, characterized by the absence of immunological memory, represented by neutrophils, eosinophils, natural killer (NK) cells, mast cells, cytokines, complement, and anti-bacterial peptides; or in the form of adaptive immunity, through antigen-presenting cells (dendritic cells), T-lymphocytes (regulators, CD8 and CD4) and B-lymphocytes.8
The immune system, under physiological conditions, can recognize and destroy antigens from infectious agents and/ or neoantigens from neoplastic cells, acting through innate and adaptive immunities. The neoantigens formation results from the cell mutation process, through which unrepaired damage to cellular DNA sequences promote mutations that lead to changes in cell functions and carcinogenesis.2,8,27,30
Cutaneous squamous cell carcinomas (SCCs) originate from mutations in keratinocytes of the epidermal squamous cell layer, which expand into tissues through neoplastic clones. Tumor promoters stimulate clonal tumor expansion. They can be exogenous, such as ultraviolet radiation (UVR), chemical agents, medications, and infections, or endogenous, such as diet and immune suppression. SCCs carry one of the highest tumor mutation loads among all types of cancer, which increases their immunogenicity due to the expression of tumor neoantigens, mutations, and/or viral gene expression.2,27,30
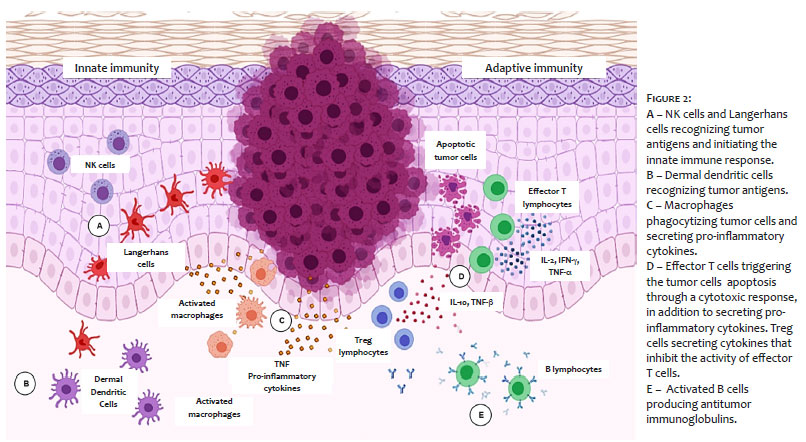
Natural killer (NK) cells represent one of the main cell lines of innate immunity, and they’re found mainly in the dermis.31 NK cells are responsible for the neoantigens immunosurveillance, controlling tumor progression through cytolytic response.36 Tissue macrophages also constitute another crucial lineage in the antitumor immune response, identifying damaged keratinocytes and promoting leukocyte recruitment and pro-inflammatory mediator in the neoplastic site to eradicate cancer cells. However, when infiltrated into neoplastic tissue, tumor-associated macrophages act as stimulating agents for tumor development by secreting pro-angiogenic factors such as vascular endothelial growth factor (VEGF) and matrix metalloproteinases (MMP).31,36
Dendritic cells (DCs) also promote antigens recogni-tion in peripheral tissues, and they’re differentiated into six sub-types of cutaneous dendritic cells. The Langerhans cells, present in the corneal and granular layers of the epidermis, and the dermal myeloid dendritic cells, found in the dermis, can be high-lighted. Dendritic cells recognize neoplastic neoantigens in the cutaneous tissue, introducing them to CD8+ and CD4+ naive T-lymphocytes located in regional lymph nodes .31,40,41
T cells make up about 10% of the cellular infiltrate of skin tumors, thus playing an essential role in neoplastic immunological control. Dendric cells introduce tumor neoantigens through the major histocompatibility complex (MHC). They promote the activation of naive T cells into effector T cells and the polarization of T cell responses into Th1, Th2, Th9, and Th17.31,40 The T response pattern is crucial to prevent the development of cutaneous malignancy and metastases. The Th1 pat-tern (cytotoxic response) is the main responsible for controlling tumor progression, and the Th2 pattern is generally associated with neoplastic development.31,40
In addition to cellular immunity, the humoral response of effector B cells is also an essential component of neoplastic control. B cells act through the immunoglobulins and cytokines production, contributing to the T-lymphocyte responses polar-ization, and to pro-inflammatory mechanisms chemotaxis and activation that will lead to carcinogenesis failure.31
Despite the immune control mechanisms, some neo-plasms can evade the immune system, proliferating and invading adjacent structures and spreading to other tissues.8 The neoplastic evasion process is strongly influenced by the tumor micro-environment through its cellular, molecular, and environmental characteristics.
The tumor microenvironment comprises several malignant and non-malignant cell types that establish complex and dynamic interactions through chemotactic agents, such as cytokines, growth factors, and inflammatory enzymes.31 In this perspective, the balance or imbalance between such biological interactions will determine tumor progression or suppression through mechanisms intrinsic or extrinsic to neoplastic cells (Figure 2).
Among the intrinsic factors is the tumor’s surface pro-teins expression, hindering recognition and phagocytosis by DCs, and the cytokines secretion, promoting DC dysfunction and inhibiting specific tumor T cells activation. It results in an increased SCCs tumor burden.31,40,41
The immune status is one of the extrinsic factors that influence the tumor microenvironment.27 It can also affect the Th1 and Th2 immunity patterns. Immunocompetent individ-uals tend to demonstrate gene expressions associated with Th1 and Th2 responses, while immunosuppressed individuals show a Th2 immunity predominance, an immune response more related to cell infiltration and tumor progression.27,31
Another extrinsic factor is ultraviolet (UV) radiation, which acts in the tumor microenvironment inducing dendritic cells’ apoptosis and reducing their lymphatic migration. Thus, it impairs the CD8+ T-lymphocyte cytotoxic response mediated by CDs. UV radiation also stimulates the pro-inflammatory mediators released by infiltrating keratinocytes and leukocytes that favor the SCCs initial development.27,31
From another perspective, Bottomley et al. proposed the concept of “immunoediting”, a process where the tumor cells’ elimination by immune defense mechanisms would lead to the neoplastic cells selection without specific immunogen-ic antigens. These cells, when not recognized by the immune system, would then have the ability to proliferate in the tumor microenvironment.31
However, the “immuneditingesIt theless cells (Treg),-main ‘e governan de modo globalnismo todo. Nao podemos , deppois so caminho e os. Os monstros uqe q” does not consist of an “escape” mechanism per se and may result in three types of outcomes: elimination, where the immune system can to-tally eliminate the tumor cells; equilibrium, where the immune mechanisms control the tumor progression but fail to eradicate the cancer cells completely; and escape, where tumor cell lines proliferate, combining characteristics of immune evasion and re-sistance to apoptosis.31
Immunological tolerance has also been recognized as one of the main “escape” tumor cells mechanisms. Under physiological conditions, inactivated and immature dendritic cells stimulate the regulatory T cells (Treg) differentiation, which acts by inhibiting the effector T cells cytotoxic responses, limiting excessive immune reactivity.31,40
Nevertheless, Treg cells act by preventing the secretion and proliferation of dendritic cells in the tumor microenvironment. It reduces the presentation quality of neoplastic neoantigens and results in an imbalance towards the inhibition of effector T activation.22,31,40 Regulatory T cells are identified in tumor infiltrates of BCCs and SCCs.2 This fact can be explained by the ability of tumor cells to recruit immunosuppressive cells, such as Treg cells and myeloid-derived suppressor cells (MDSCs), favor-ing neoplastic evolution.8
It is worth highlighting the influence of individual variants on the tumor microenvironment composition — cytokines, interleukins, interferons, and infiltrating immune cells (T, Treg, and B-lymphocytes), determining the immune response pattern and tumor progression control.22
Self-tolerance represents an essential element of the immune system. It promotes immune response regulation, preventing excessive inflammatory and cytotoxic processes that would cause the degradation of healthy tissues adjacent to the lesions. Under physiological conditions, immune modulation results from the activity of cellular molecules and receptors called immune checkpoints.8,9
Nevertheless, cancer cells have acquired the ability to overexpress molecules and receptors of immune checkpoints, evading the antitumor mechanism and, consequently, progressing uninhibitedly.8 Programmed cell death protein 1 (PD-1), programmed cell death ligand 1 (PD-L1), cytotoxic T-lympho-cyte-associated antigen 4 (CTLA-4), and epidermal growth fac-tor receptor (EGFR) represent the main immune checkpoints expressed in SCC tumor cells, signaling their relevance as potential therapeutic targets.8,9,14
CTLA-4 is expressed on the surface of cytotoxic T-lymphocytes and acts to prevent these cells’ activation, trig-gered by the binding with CD80 and CD86 dendritic cells proteins. However, T cells also have the surface protein CD28, which promotes the stimulation of cytotoxic T activity through CD80 and CD86 ligands. Therefore, the effector T-lymphocyte’s response will depend on the balance of the bindings between CD80 and CD86 with the CTLA-4 (“inhibitory”) and CD28 (“stimulator”) receptors.8
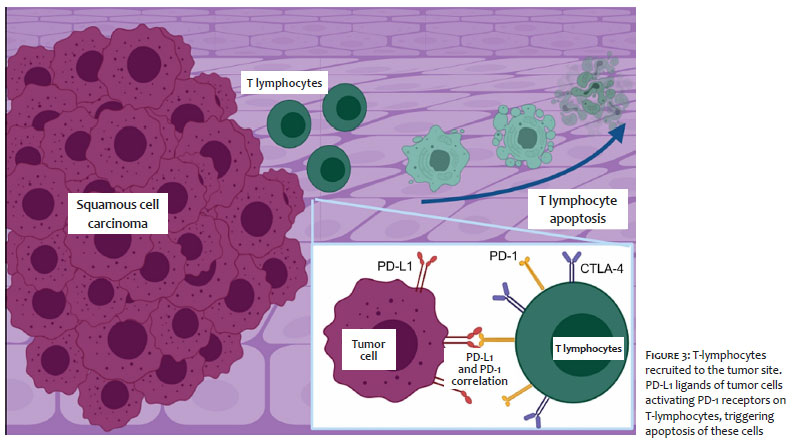
PD-1 is a cell surface receptor found on T and B cells, NK cells, dendritic cells, and monocytes. In T cells, PD-1 is only expressed after their activation, promoting effector T cells apop-tosis. Also, it inhibits Treg cells apoptosis by binding to PD-L1 and PD-L2 proteins (programmed cell death ligands 1 and 2) present on the surface of tumor cells.8,14,31,32 Thus, cancer clones can increase their PD-L1 surface presentation, avoiding immu-nological surveillance.19,32 Amoils et al. corroborated this understanding, emphasizing the association of increased PD-L1 expression with metastatic and recurrent SCCs. From another perspective, Pezeshki et al. highlighted the PD-1 and PD-L1 role in the “T cell exhaustion” phenomenon, resulting from the potency reduction in the T cell clones from chronic exposure to a particular antigen.16
The EGFR gene is another important tumor check-point component, encoding a transmembrane glycoprotein receptor responsible for activating multiple downstream signaling pathways - including MAPK/ERK and PI3K/AKT/mTOR -that control processes of maturation, proliferation, apoptosis inhibition, and cells angiogenesis.29 EGFR deregulation has been observed in head, neck, ovary, breast, bladder, colon, and lung carcinomas, and it is related to tumor proliferation. In cutaneous SCC cases, despite the low incidence of EGFR mutations — ranging from 2.5% to 5% — this gene overexpression has been associated with metastases and a worse prognosis.21,29
In this respect, the study of the immune response role in the tumor microenvironment in recent years has stimulated the development of target therapies aimed at overexpressed ligands in tumor tissue.8 The mechanisms of inhibition of CTLA-4 and PD-1 receptors on immune cells and PD-L1 on neoplastic cells were described for the first time in 2018. It enabled the in-terruption of the mechanism of the tumor evasion, allowing the effector T cells action to control the cancers’ progression (Figure 3).8,9,18,22,32
In this perspective, CTLA-4 blocking would allow the effector T-lymphocytes activation, while blocking PD-1 or PD-L1 would inhibit the effector T-lymphocytes apoptosis, as well as the phenomenon of“T cell exhaustion”. Thus, both therapeutic pathways would promote increased cellular immunity activity mediated by T cells.8 On the other hand, blocking the EGFR would inhibit one of the mechanisms of tumor cells “evasion”, allowing the immune system to act on them.21,29
Still, it is noteworthy that the immune activity stimula-tion by immunotherapy drugs can trigger nonspecific immune responses, in the form of autoimmune diseases such as vitiligo. Furthermore, these medications also demonstrate the potential to cause adverse events such as pruritus, lichenoid rash, papulopustular eruptions, among other skin manifestations, as well as diarrhea and hypothyroidism.19,24,39
Understanding the immune surveillance of cancers and the mechanisms of tumor “evasion” allowed the development of drugs that block the receptors involved in these pathways, with greater emphasis on the CTLA-4, PD-1, and EGFR receptors.8
Due to the high mutational load of SCCs, they become very susceptible to blocking immune checkpoints.8
The main indications for immunotherapy are locally advanced, unresectable, incurable, metastatic SCCs and cases of good tolerability to medications with potential increased survival.15 The combination of anti-CTLA-4 and anti-PD-1 medications has been reported in specific cases of melanoma, renal cell carcinoma, and recurrent and metastatic SCCs of head and neck, demonstrating better therapeutic responses.8,25 However, such combinations have higher toxicity, with the risk of triggering colitis and hypophysis.24
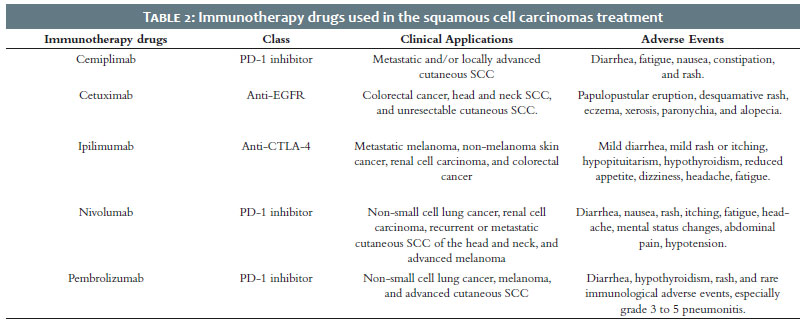
The advent of checkpoint inhibitor therapy has raised promising expectations for the treatment of locally advanced, recurrent, and metastatic SCCs, with improved patient over-all survival as well as progression-free survival.8,25 Ipilimumab, CTLA-4 inhibitor, nivolumab, pembrolizumab, cemiplimab, PD-1 inhibitors, cetuximab, and anti-EGFR are the immuno-logical checkpoint inhibitors currently approved for skin neo-plasms (Table 2).8,18,35
Ipilimumab can cause adverse events such as autoimmune dermatitis, colitis, and diarrhea, in addition to skin reac-tions such as pruritus, morbilliform eruption, nodular pruritus, lichenoid rash, and photosensitivity. In general, these adverse events present after three to six weeks from the start of the medication, being dose-dependent and reversible with the end of the treatment.39
Nivolumab is a PD-1 receptor inhibitor that prevents the T-lymphocyte’s deactivation and preserves the cellular immunity function. The FDA approved the drug in 2017 to treat recurrent or metastatic head and neck SCCs, and advanced melanoma.21,26 However, nivolumabs role in non-melanoma skin cancers has not yet been fully elucidated.7
Chen et al. reported a case of complete remission of an invasive and poorly differentiated SCC in the auricle. The treatment was based on immunotherapy using a combination of nivolumab and cetuximab — antibody against the epidermal growth factor receptor (EGFR). The case reported by Chen et al. avoided extensive surgery with a potential risk of facial nerve palsy through these immunotherapy drugs and showed promis-ing results.7
Regarding adverse events, mild fatigue represented the most common condition. However, the literature has also re-ported dermatological disorders such as vitiligo, skin rash, itch-ing, endocrine hypofunction, and hip fracture.26,39
Cemiplimab is a human IgG4 monoclonal antibody with a high affinity for the PD-1 receptor. It promotes the blocking of PD-L1 (expressed in tumor cells) and stimulates the effector T cells’ action. It was the first systemic therapy approved to treat metastatic or locally advanced SCCs not suitable for curative surgery or radiotherapy17,20,23,26,37
Several studies have demonstrated the effectiveness of cemiplimab use to treat SCCs, reducing the diameters of target lesions.17,23,37 Ahmed et al. demonstrated a cemiplimab response rate of 50% in advanced SCC cases — in a phase 1 study — and a response rate of 47% in metastatic disease cases — in a phase 2 study.23
Regarding the adverse events, the most common are diarrhea, fatigue, nausea, constipation, and rash,23,33 which are solved by adjusting the therapeutic doses and/or discontinuing the treatment.23 Despite the adverse events, cemiplimab has a clinically significant lasting effect, with acceptable safety and tol-erability profile.20
Cetuximab is a chimeric immunoglobulin (IgG1mAb) that binds to domain 3 of the extracellular domain of the epi-dermal growth factor receptor (EGFR), leading to innate and adaptive immune responses in tumors dependent on this oncogenic pathway.13,21 The response to cetuximab correlates to the tumor’s EGFR expression. It can restore the anti-tumor immune response, lead to cell cytotoxicity of NK cells, in addition to maturation and crosstalk between NK and dendritic cells.13,21
Cetuximab was initially approved to treat colorectal cancer. Currently, it has been approved for advanced head and neck and/or platinum-refractory SCCs, and it can be adopted as adjuvant therapy to surgery and radiotherapy.4 Cetuximab has been described as the most effective anti-EGFR in SCC treatment, with promising results when combined with other therapeutic alternatives.4,13
A 2014 study on the treatment of unresectable SCCs compared the use of cetuximab in monotherapy with combinations of the drug with carboplatin or radiotherapy. The results showed control rates of 50% for monotherapy, 87.5% for cetuximab + carboplatin, and 100 % for cetuximab + radiotherapy.4 Another phase 2 clinical trial study on the use of cetuximab in monotherapy to treat unresectable SCCs observed disease stabi-lization in 58% of cases.21 However, the medication still presents unpromising cure rates: 3% of complete remission and 8% partial response in advanced SCC cases.21
The treatment of cutaneous neoplasms is at an advanced stage, benefiting patients affected with tumors that are challenging to access surgically and reconstruct anatomically. The use of many of these therapies is still under investigation, clinical trial, or approval. Still, the literature already presents evi-dence to support the consideration of the great importance and benefit of these new therapeutic strategies.
It’s essential to understanding the physiopathogenesis of SCCs to promote the development of new therapeutic ap-proaches that may soon benefit a more significant number of patients.
Magda Blessmann Weber 0000-0001-5885-5851
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Iago Gonçalves Ferreira 0000-0002-4695-1982
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Laura Oliveira Ferreira 0000-0003-2767-7479
Author's contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Anna Bittarello Silva 0000-0003-4277-1439
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Selma Schuartz Cernea 0000-0002-0710-5935
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
1. Parekh V, Seykora JT. Cutaneous squamous cell carcinoma. Clin Lab Med [Internet]. 2017;37(3):503-25.
2. Hall ET, Fernandez-Lopez E, Silk AW, Dummer R, Bhatia S. Immunologic characteristics of nonmelanoma skin cancers: implications for immunotherapy. Am Soc Clin Oncol Educ Book. 2020;40:1-10.
3. Ministério da Saúde. Estimativa 2020 - Incidência de Câncer no Brasil [Internet]. Ministério da Saúde - Instituto Nacional de Câncer José Alencar Gomes da Silva. Rio de Janeiro; 2019. Available at: https://ejournal.poltektegal.ac.id/index.php/siklus/article/view/298%0Aht-tp://repositorio.unan.edu.ni/2986/1/5624.pdf%0Ahttp://dx.doi.or-g/10.1016/j.jana.2015.10.005%0Ahttp://www.biomedcentral.com/1471-2458/12/58%0Ahttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&P
4. 4Lima PO, Joseph S, Panizza B, Simpson F. Epidermal growth factor re-ceptor's function in cutaneous squamous cell carcinoma and its role as a therapeutic target in the age of immunotherapies. Curr Treat Options Oncol. 2020;21(1):9.
5. Ascierto PA, Garbe C. Updates and new perspectives in nonmelanoma skin cancer therapy: highlights from "Immunotherapy Bridge". Immu-notherapy. 2020;12(3):167-74.
6. Misiakos EP, Damaskou V, Koumarianou A, Gouloumi AR, Patapis P, Za-vras N, et al. A giant squamous cell carcinoma of the skin of the tho-racic wall: a case report and review of the literature. J Med Case Rep. 2017;11:136.
7. Chen A, Ali N, Boasberg P, Ho A. Clinical remission of cutaneous squamous cell carcinoma of the auricle with cetuximab and nivolumab. J Clin Med. 2018;7(1):10.
8. Habib LA, Wolkow N, Freitag SK, Yoon MK. Advances in immunotherapy and periocular malignancy. Semin Ophthalmol. 2019;34(4):327-33.
9. Guminski A, Stein B. Immunotherapy and other systemic therapies for cutaneous SCC. Oral Oncol. 2019;99:104459. Epub 2019 Nov 9.
10. Taefehshokr N, Baradaran B, Baghbanzadeh A, Taefehshokr S. Pro-mising approaches in cancer immunotherapy. Immunobiology. 2020;225(2):151875.
11. Cunha PLP. Manual revisão bibliográfica sistemática integrativa: a pesquisa baseada em evidências. Belo Horizonte: Grupo Anima Educação; 2014. 63 p.
12. Souza MT, Dias M, Carvalho R. Revisão integrativa: o que é e como fazer. Einstein. 2010;8(1):102-6.
13. Choi FD, Kraus CN, Elsensohn AN, Carley SK, Lehmer LM, Nguyen RT, et al. Programmed cell death 1 protein and programmed death-ligand 1 inhibitors in the treatment of nonmelanoma skin cancer: a systematic review. J Am Acad Dermatol. 2020;82(2):440-59.
14. Salzmann M, Leiter U, Loquai C, Zimmer L, Ugurel S, Gutzmer R, et al. Programmed cell death protein 1 inhibitors in advanced cutaneous squamous cell carcinoma: real-world data of a retrospective, multicen-ter study. Eur J Cancer. 2020;138:125-32.
15. Hanna GJ, Ruiz ES, LeBoeuf NR, Thakuria M, Schmults CD, Decaprio JA, et al. Real-world outcomes treating patients with advanced cutaneous squamous cell carcinoma with immune checkpoint inhibitors (CPI). Br J Cancer. 2020;123(10):1535-42.
16. Pezeshki S, Hemmati S, Rezaei N. Novel treatments using PD1 inhibitors for advanced and metastatic cutaneous squamous cell carcinoma. Expert Rev Anticancer Ther. 2020;20(10):819-22.
17. Rischin D, Migden MR, Lim AM, Schmults CD, Khushalani NI, Hughes BGM, et al. Phase 2 study of cemiplimab in patients with metastatic cutaneous squamous cell carcinoma: primary analysis of fixed-dosing, long-term outcome of weight-based dosing. J Immunother Cancer. 2020;8(1):e000775.
18. Barrios DM, Do MH, Phillips GS, Postow MA, Akaike T, Nghiem P, et al. Immune checkpoint inhibitors to treat cutaneous malignancies. J Am Acad Dermatol. 2020;83(5):1239-53.
19. Desilets A, Soulières D. Safety evaluation of pembrolizumab for treating recurrent head and neck squamous cell carcinoma. Expert Opin Drug Saf. 2020;19(8):927-34.
20. Lee A, Duggan S, Deeks ED. Cemiplimab: a review in advanced cuta-neous squamous cell carcinoma. Drugs. 2020;80(8):813-9.
21. Ferris RL, Licitra L, Fayette J, Even C, Blumenschein G, Harrington KJ, et al. Nivolumab in patients with recurrent or metastatic squamous cell carcinoma of the head and neck: Efficacy and safety in checkmate 141 by prior cetuximab use. Clin Cancer Res. 2019;25(17):5221-30.
22. Liebl MC, Hofmann TG. Identification of responders to immune checkpoint therapy: which biomarkers have the highest value? J Eur Acad Dermatol Venereol. 2019;33(Suppl 8):52-6.
23. Ahmed SR, Petersen E, Patel R, Migden MR. Cemiplimab-rwlc as first and only treatment for advanced cutaneous squamous cell carcinoma. Expert Rev Clin Pharmacol. 2019;12(10):947-51.
24. van Baar MLM, Guminski AD, Ferguson PM, Martin LK. Pembrolizumab for cutaneous squamous cell carcinoma: report of a case of inoperable squamous cell carcinoma with complete response to pembrolizumab complicated by granulomatous inflammation. JAAD Case Reports. 2019;5(6):491-4.
25. Kacew AJ, Harris EJ, Lorch JH, Haddad RI, Chau NG, Rabinowits G, et al. Chromosome 3q arm gain linked to immunotherapy response in advanced cutaneous squamous cell carcinoma. Eur J Cancer. 2019;113:1-9.
26. Ogata D, Tsuchida T. Systemic immunotherapy for advanced cutaneous squamous cell carcinoma. Curr Treat Options Oncol. 2019;20(4):30.
27. Paulson KG, Lahman MC, Chapuis AG, Brownell I. Immunotherapy for skin cancer. Int Immunol. 2019;31(7):465-75.
28. Liu Y, Fitzgerald B, Perry E, Pathak A, Chao HH. Prolonged response to pembrolizumab in spindle cell squamous cell carcinoma metastatic to the central nervous system. J Investig Med High Impact Case Reports. 2019;7:1-5.
29. Di Nardo L, Pellegrini C, Di Stefani A, Del Regno L, Sollena P, Picceril-lo A, et al. Molecular genetics of cutaneous squamous cell carcinoma: perspective for treatment strategies. J Eur Acad Dermatology Venereol. 2020;34(5):932-41.
30. Barber BR. Immune status and immunotherapy in advanced cutaneous squamous cell carcinoma -What are our next steps? JAMA Otolaryngol Neck Surg. 2019;145(4):361.
31. Bottomley MJ, Thomson J, Harwood C, Leigh I. The role of the immune system in cutaneous squamous cell carcinoma. Int J Mol Sci. 2019;20(8):2009.
32. Amoils M, Kim J, Lee C, Sunwoo JB, Colevas AD, Aasi SZ, et al. PD-L1 Ex-pression and Tumor-Infiltrating Lymphocytes in High-Risk and Metas-tatic Cutaneous Squamous Cell Carcinoma. Otolaryngol - Head Neck Surg. 2018;160(1):93-9.
33. Migden MR, Rischin D, Schmults CD, Guminski A, Hauschild A, Lewis KD, et al. PD-1 blockade with cemiplimab in advanced cutaneous squa-mous-cell carcinoma. N Engl J Med. 2018;379:341-51.
34. Degache E, Crochet J, Simon N, Tardieu M, Trabelsi S, Moncourier M, et al. Major response to pembrolizumab in two patients with locally ad-vanced cutaneous squamous cell carcinoma. J Eur Acad Dermatology Venereol. 2018;32(7):e257-8.
35. Yanagi T, Kitamura S, Hata H. Novel therapeutic targets in cutaneous squamous cell carcinoma. Front Oncol. 2018;8:79.
36. Ilyas M, Costello CM, Sharma A. Exploring the relationship between natural killer cells and cutaneous squamous cell carcinoma development. JAAD Case Reports. 2017;3(4):364-6.
37. Falchook GS, Leidner R, Stankevich E, Piening B, Bifulco C, Lowy I, et al. Responses of metastatic basal cell and cutaneous squamous cell car-cinomas to anti PD1 monoclonal antibody REGN2810. J Immunother Cancer. 2016;4(1):1-5.
38. Chang ALS, Kim J, Luciano R, Sullivan-Chang L, Colevas AD. A case re-port of unresectable cutaneous squamous cell carcinoma responsive to pembrolizumab, a programmed cell death protein 1 inhibitor. JAMA Dermatology. 2016;152(1):106-8.
39. Macdonald JB, Macdonald B, Golitz LE, LoRusso P, Sekulic A. Cuta-neous adverse effects of targeted therapies. J Am Acad Dermatol. 2015;72(2):203-18.
40. Yanofsky VR, Mitsui H, Felsen D, Carucci JA. Understanding dendritic cells and their role in cutaneous carcinoma and cancer immunothera-py. Clin Dev Immunol. 2013;2013:624123.
41. Fujita H, Suárez-Farías M, Mitsui H, Gonzalez J, Bluth MJ, Zhang S, et al. Langerhans cells from human cutaneous squamous cell carcinoma in-duce strong type 1 immunity. J Invest Dermatol. 2012;132(6):1645-55.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}