


Katherine Santacoloma; Barbara Ciraudo; Marcela Duarte Benez Miller; Guillermo Loda
Submitted on: 04/09/2020
Approved on: 04/03/2021
Financial support: Nenhuma
Conflit of interest: Nenhum
How to cite this article: Santacoloma K, Ciraudo B, Miller MDB, Loda G. East-west advancement flap: a useful tool to reconstruct nasal tip defects. Surg Cosmet Dermatol. 2021;13:e20210010.
The reconstruction of nasal defects secondary to non-melanoma skin cancer represents a surgical challenge, especially in the nasal tip, due to its limited local laxity and possible asymmetries. There are multiple techniques to perform this closure, but most are flaps from distant locations that can lead to less aesthetic results. We present two cases of basal cell carcinoma on the nasal tip, where reconstruction with the east-west advancement flap was performed after tumor excision, with a modification of the flap in one of the patients, obtaining a good structural and aesthetic result.
Keywords: Surgical flaps; Carcinoma, basal cell; Nose; Dermatologic surgical procedures
The nose is one of the most common sites for skin cancer, representing a surgical challenge because of its limited local laxity, especially on its tip. It often requires reconstruction with flaps from distant locations, leading to esthetic problems regarding texture, skin color, prominent and visible scars, and possible impairment of the anatomy of the nasal wings’ edges. The east-west flap is a horizontal advancement flap, useful for small to medium-sized defects. It is easy to design and execute, with little tissue movement and excellent esthetic results, preserving the nasal architecture and masking the suture lines.1,2 We present two cases where this flap was successfully performed, with a modification in one of the patients’ flaps.
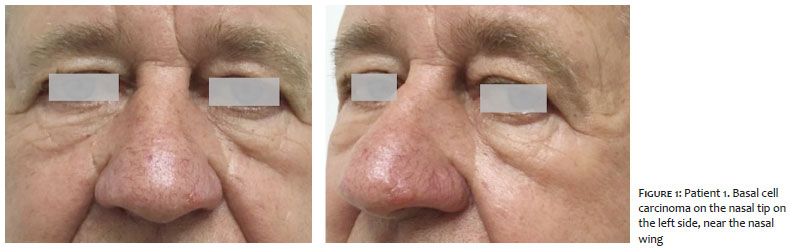
A 65-year-old man with controlled arterial hypertension consulted the dermatological surgery service due to a nodular basal cell carcinoma on the nasal tip, confirmed by biopsy, with two years of evolution. The tumor measured 1.3 x 1.0 cm, and it was located on the left side of the nasal tip, close to the free edge of the nasal wing (Figure 1). We performed the tumor excision with frozen-section control of surgical margins and repair with an east-west advancement flap.
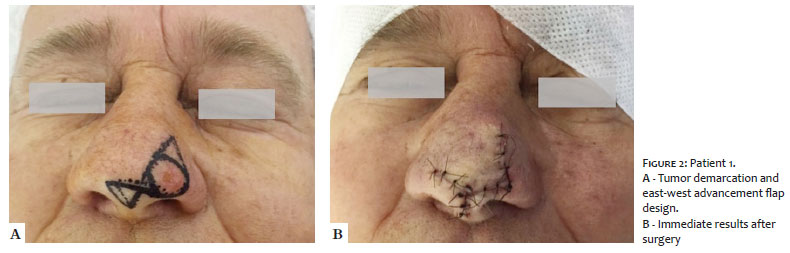
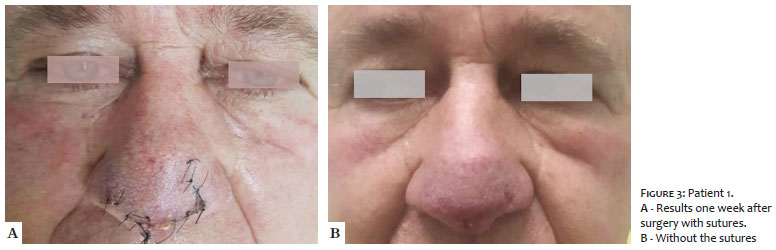
Regarding the surgical approach, the first step was marking the tumor with a 4 mm margin. Subsequently, we designed the flap with two triangles: the first superior triangle above the defect, and the second inferior one in the nasal midline, in the middle of the columella. After tumescent anesthesia and excision of the lesion, intraoperative frozen section confirmed that the margins were free. Afterward, we removed both triangles and detached the flap. Through a horizontal advancement, the tissue was moved from the nasal tip to the left lateral region of the defect, and the flap was synthesized using a subdermal suture with 5.0 absorbable suture threads and simple stitches on the surface with 5.0 nylon (Figure 2). The sutures were removed within a week, with an excellent esthetic outcome (Figure 3).
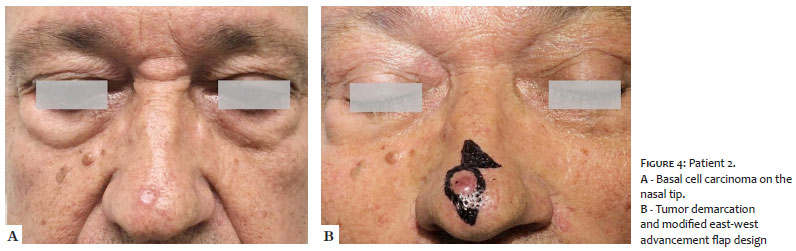
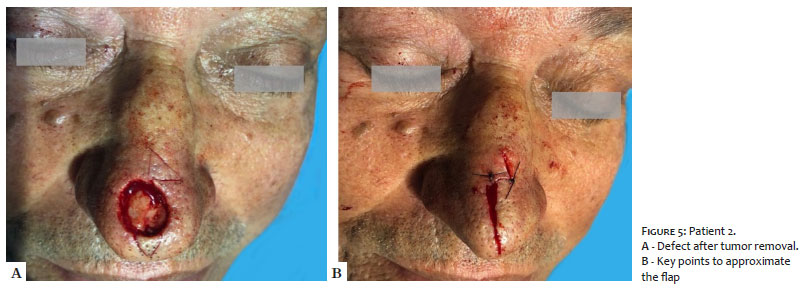
A 57-year-old man without comorbidities was diagnosed with nodular basal cell carcinoma in the nasal supratip region with a slight deviation to the right side (Figure 4). The tumor, measuring 1.0 x 0.9 cm, was excised with frozen-section control of surgical margins and closure with an east-west advancement flap.
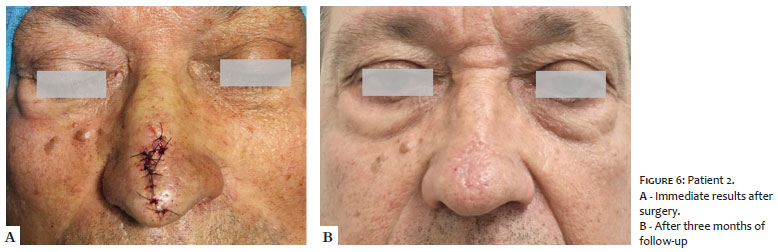
We chose a surgical approach similar to the first patient; however, we modified the flap design. In this case, the first triangle was designed on the left side of the defect, starting at the top, and the second inferior one was drawn below, in the nasal midline. After excising the tumor, we removed both triangles with a good detachment, moving the tissues horizontally and bilaterally from the lateral part to the middle of the nasal tip. The defect was closed by tissue synthesis, like in the previous case (Figure 5). The postoperative period, with three months of follow-up, showed an excellent outcome (Figure 6).
The east-west flap consists of a horizontal advancement movement. Perry Robins described it, and it uses Burow’s triangles to close defects.1,2 The Burow’s triangle advancement flap are half of an A-T advancement flap (also named O-T flap). Some of its advantages are having a pedicle with scarce tissue reserves and being used in challenging areas such as those close to free edges.3 This condition was evident in the first case, where the defect was very close to the free edge of the left nasal wing. This type of reconstruction prevents its deformity.
In addition to its use in the nasal tip, the approach with Burow’s triangles can be performed in other areas such as the nasal ala, upper lip, malar region near the orbital rim (named “J-plasty” by Kouba and Miller), forehead, and temple, among others.2,3,4
However, the significance of this flap for nasal tip defects links to the high frequency of skin cancer in this topography, cutaneous tissue difficult mobilization due to its anatomical characteristics, and defects in the center of the face that can radically change the individual’s facial and aesthetic characteristics.1,2,5
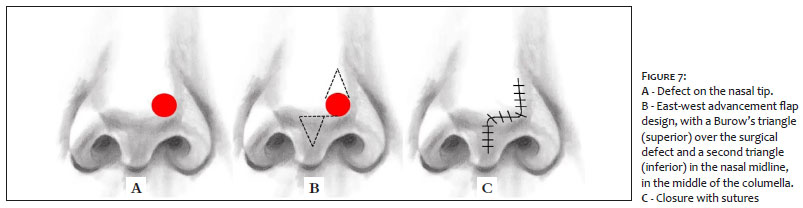
Regarding the making of the flap, the first Burow’s triangle (superior) is designed over the surgical defect, with its base tangent to the upper portion of the defect and its vertex towards the nasal dorsum. The second triangle (inferior) is designed in the nasal midline, in the middle of the columella, with its vertex pointing to the lip and its base tangent to a horizontal line drawn from the lower portion of the tumor (Figure 7). This lower triangle is designed medially, so the flap is moved towards a cosmetically more advantageous area.1,2,6
In the second case, the flap was adapted due to the location of the basal cell carcinoma. The flap was designed with a triangle inferior to the defect and another superior triangle on the left side due to the tumor’s sight deviation tumor to the right side. Thus, the east-west advancement flap can be modified, and its triangles repositioned according to the tumor’s position on the nasal tip.
This type of flap is beneficial to repair minor to medium-sized defects (<1.5 cm in diameter) on the nasal tip or dorsum laterally to the nasal supratip, as in the case of the two patients. Its benefits are keeping the reconstruction in the same nasal subunit, preserving the skin’s color and texture; excellent vascular supply through the large pedicle, with a lower risk of necrosis; enabling reconstructions without geometric or architectural distortion; not shortening or twisting the nose and not deforming the nasal wing free edge; good camouflage of the suture stitches in the vertical and horizontal axes of the nose. The advantage of good healing in the region should also be highlighted, as connective tissue constitutes most of the nasal structure, which is rich in sebaceous glands.1,2,5,6 Both cases evidenced all these benefits, with great esthetic result at one week and three months after surgery, respectively.
However, this study has limitations, such as wide defects, larger than 1.5 cm, because triangles can become very extensive, causing locoregional deformations. Also, the nose size influences the technique choice, as wider noses carry larger defects, while smaller noses may require movement of distant lateral tissue, resulting in a tight nose appearance. 1,2,6
The east-west advancement flap is an aesthetically excellent repair for small to medium-sized skin cancer defects on the nasal tip. In addition to being easy to design and execute, it requires little tissue movement, hides the suture lines well, maintains the color and texture of the nasal subunit skin, has a large pedicle reducing the risk of necrosis, and does not cause nose distortion. All of these benefits are critical because any defect in this area can seriously affect individual facial features. In well-selected cases, the result of this type of horizontal advancement flap may be superior to the rotation flap, which has long incisions that are difficult to disguise, or the transposition flap, which can cause tissue distortion.
Katherine Santacoloma 0000-0002-6645-7826
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Barbara Ciraudo 0000-0003-0805-0160
Study design and planning.
Marcela Duarte Benez Miller 0000-0003-0289-5656
Approval of the final version of the manuscript; critical revision of the manuscript.
Guillermo Loda 0000-0003-0511-0025
Approval of the final version of the manuscript.
1. Goldberg LH, Alam M. Horizontal advancement flap for symmetric reconstruction of small to medium-sized cutaneous defects of the lateral nasal supratip. J Am Acad Dermatol. 2003;49(4):685-9.
2. Magliano J, Abelenda MP, Navarrete J, Bazzano C. East-west flap after Mohs micrographic surgery. Actas Dermosifiliogr. 2019;110(9):759-62.
3. Krishnan R, Garmn M, Nunez-Gussman J, Orengo I. Advancement flaps: a basic theme with many variations. Dermatol Surg. 2005;31(8):986-94.
4. Ascari-Raccagni A, Dondas A, Righini MG, Trevisan G. The east-west advancement flap (horizontal advancement flap) to repair a defect on the nose ala. JEADV. 2010;24(8):926-29.
5. Summers BK, Siegle RJ. Facial cutaneous reconstructive surgery: facial flaps. J Am Acad Dermatol. 1993;29(6):917-41.
6. Geist DE, Malony ME. The "East-West" advancement flap for nasal defects: re examined and extended. Dermatol Surg. 2012;38(9):1529-34.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}