


Katherine Santacoloma; Gabriella Mazzarone de Sá Barreto; Guillermo Loda; Marcela Duarte Benez Miller
Submitted on: 16/11/2020
Approved on: 04/03/2021
Financial support: Nenhuma
Conflit of interest: Nenhum
How to cite this article: Almeida Santacoloma K, Barreto GMS, Loda G, Miller MDB. Giant hand lipoma: a surgical challenge. Surg Cosmet Dermatol. 2021;13:e20210009.
Lipomas are frequent soft tissue tumors and can be found anywhere in the body; however, their location in hand is rare. They are called giants when they exceed 5 cm. In these cases, the differential diagnosis must be made with liposarcoma. These benign tumors must be characterized preoperatively with an imaging study, and their treatment is surgical. We present the case of a patient with a giant hand lipoma successfully treated with a modified Bruner incision approach.
Keywords: Lipoma; Liposarcoma; Neoplasms, adipose tissue; Hand
Lipomas are the most common soft tissue tumors in the population. They are benign and composed of adipose tissue. These tumors can present anywhere on the body, often affecting the upper limbs but rarely the hand.1
Slow growing, fibroelastic consistency, mobility, and absence of pain characterize lipomas. They can be located subcutaneously, intermuscularly, or intramuscularly.1
Tumors measuring more than 5 cm in diameter are considered giant lipomas. This form of presentation is rare, mainly when located in hand. In this case, these tumors can act as a mass and limit function or generate symptoms such as paresthesia, requiring a surgical approach. Likewise, it is critical to rule out malignant degeneration, usually rare, represented mainly by liposarcoma.1
We report a case of giant lipoma case on the dorsum of the dominant hand. The patient had function limitations when performing daily tasks, without other symptoms. We describe the successful surgical approach performed by the modified Bruner incision technique.
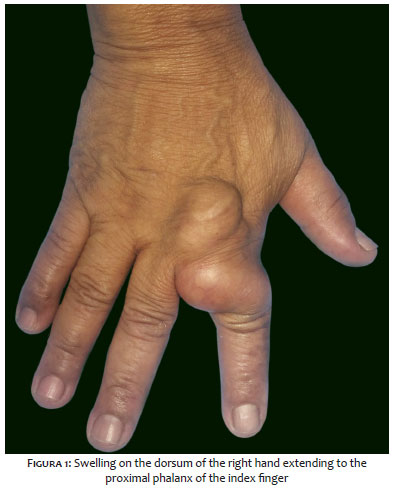
A 62-year-old woman, without comorbidities, consulted the dermatological surgery service for presenting a swelling on the dorsum of the right hand (dominant hand) extending to the index finger, with progressive growth over the last year. The patient did not present pain, paresthesia, or change in sensitivity but had limited mobility for her daily activities. Physical examination revealed a tumor with a soft consistency, smooth surface, not adhered to the deep planes. The tumor measured 7x4 cm and was located on the dorsum of the hand over the second and third metacarpals up to the second interdigital space and the proximal phalanx of the index finger (Figure 1). We performed an ultrasound that suggested lipoma.
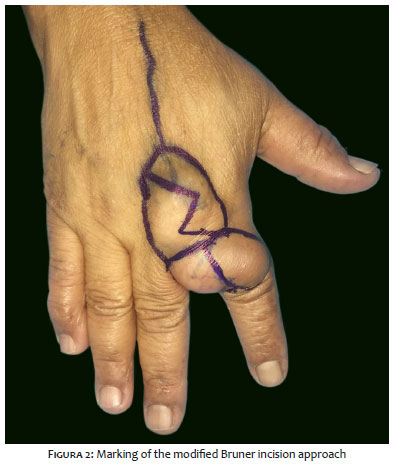
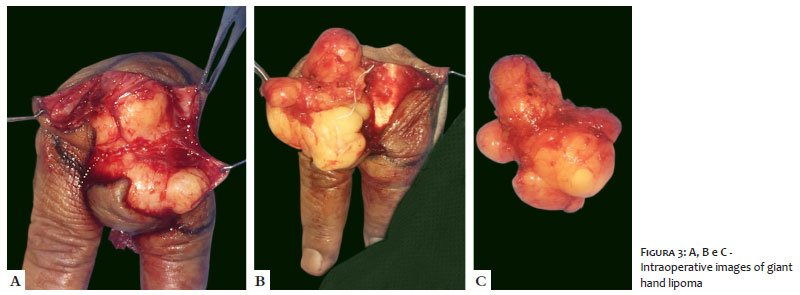
Regarding the surgical approach, we first demarcated the tumor, then drawing a zigzag incision on the dorsum of the hand and index finger, according to Bruner’s surgical principles (Figure 2). Anesthesia was regional for the radial nerve block and subsequently tumescent to obtain hydrodissection and protect the tendinous structures around the tumor. We carefully dissected the lesion from the tendon sheaths and neurovascular structures, performing a complete excision (Figures 3a, 3b, and 3c and Figures 4a and 4b). The procedure had no complications and the mobility and sensitivity of the patient’s hand were preserved. The histopathological study confirmed the diagnosis of lipoma.
Lipomas are benign tumors formed by mature adipocytes, responsible for approximately 16% of soft tissue mesenchymal tumors. They are the most common tumors in adults with a prevalence of 1% and can be found in any part of the body at the subcutaneous, intermuscular, or intramuscular level, and, less frequently, in internal organs.2,3,4
Its location in the hands is infrequent, around 5%. In this case, the thenar and hypothenar regions are the most prevalent, and the phalanges are the rarest, with a 1% prevalence. The most common benign soft tissue tumors in hand are pyogenic granuloma, ganglion cyst, giant cell tumor of the tendon sheath, hemangiomas, and others.2,3,4,5
Clinically, lipomas are firm, flexible, and relatively mobile subcutaneous nodules, slow-growing and asymptomatic. However, when they are extensive or in hand, they can compress a nerve and cause changes in sensitivity (paresthesias and dysesthesias). They can also produce functional changes, as in our patient’s case, who had limited index finger flexion.3,4 Lipomas appear mainly in the fifth and sixth decades of life, as evidenced in this patient.2
The etiology of these tumors is unknown. Nevertheless, multiple causal factors have been proposed, such as genetic, traumatic, and metabolic factors.2,4 Concerning genetic factors, lipomas are commonly associated with translocations and rearrangements of the 12q13-q15 and 6p13q chromosome regions.4,6 Regarding traumatic factors, lipomas were previously believed to be a herniation of preexisting adipose tissue through the fascia. Later, the theory emerged that growth factors, cytokines, and other inflammatory mediators released after trauma could induce the differentiation of preadipocytes into mature adipocytes, forming the tumor.6
Rapid growth, pain, large size (tumors larger than 5 cm are considered giant), or the presence of local invasion to other structures on magnetic resonance imaging may be signs of malignancy. Therefore, it is critical to conduct an imaging study, both for planning the surgical approach and to rule out malignancy, with liposarcoma as its main differential diagnosis.2,7
Imaging studies are diagnostic in 71% of cases, and computed tomography and magnetic resonance imaging are the gold standards.2 Other low-cost modalities can be used, such as radiography and ultrasound. Our patient underwent an ultrasound examination, which demonstrated a circumscribed and homogeneous hyperechoic area. Ultrasound is diagnostic in most cases, but magnetic resonance sensitivity is 94%, in addition to defining the anatomical extent of the lesion and its relationship with critical structures.4,7
Regarding surgery, the first step was to mark the tumor. The approach followed the principles of Bruner incision, especially for the flexion and extension areas of the fingers, which could extend to the hand to avoid further functional limitation with hypertrophic scars and contractures. Bruner described a zigzag volar-digital incision, where the flap angles are 90 degrees or more and are at the level of the joint folds, ensuring that the incision does not cross them.8,9 In our patient’s case, we modified the Bruner method: the zigzag incision was made at the dorsal level of the hand and index finger, due to the tumor location, without crossing the second metacarpophalangeal joint, with 90 degrees angles or less in the flaps. It allowed a good exposure of the lipoma and surrounding structures and maintained the vascularity and sensitivity of the flaps.
This modified Bruner incision approach enabled performing a complete excision of the giant lipoma, preserving hand sensitivity and motricity and managing to prevent compartment syndrome. After more than one year of follow-up, the patient also did not present contractures, hypertrophic scars, or complex regional pain syndrome, which are possible post-surgical complications.2,4
Giant hand lipomas are rare, benign tumors with an excellent prognosis after successful surgical excision and low recurrence. However, preoperative imaging assessment is essential for planning the surgical approach. Bruner incision technique is an interesting strategy to be considered in the hand region for its satisfactory functional and cosmetic outcomes.
Katherine Santacoloma 0000-0002-6645-7826
Preparation and writing of the manuscript; critical literature review.
Gabriella Mazzarone de Sá Barreto 0000-0002-6650-9737
Preparation and writing of the manuscript.
Guillermo Loda 0000-0003-0511-0025
Approval of the final version of the manuscript; critical revision of the manuscript
Marcela Duarte Benez Miller 0000-0003-0289-5656
Approval of the final version of the manuscript; critical revision of the manuscript.
1. Kim KS, Lee H, Lim DS, Hwang JH, Lee SY. Giant lipoma in the hand: a case report. Medicine. 2019;98(52):e18434.
2. Ramirez-Montaño L, Pacheco-López R, Sastre-Ortiz N. Giant lipoma of the third finger of the hand. SpringerPlus. 2013;2(164):1-4.
3. Morales C, López-Mendoza J, Gargollo-Orvañanos C, Jiménez Y. Lipoma de la mano, clínica y quirúrgimente un tumor menospreciado. Cir Plást Iberolatinoam. 2011;37(4):349-53.
4. Enríquez-Merino J, Navarrete-Franco G, Nava-Estrada M, Espinosa-Villaseñor N. Lipoma en falange. Rev Cent Dermatol Pascua. 2016;25(1):24-6.
5. Irmak F, Basdelioglu K, Serhat SS, Sevim KZ, Yesilada AK. Benign soft tissue tumors of the hand: a retrospective review of 17-year experience. Hand Microsurg. 2018;7(2):88-92.
6. Nadar MM, Bartoli CR, Kasdan ML. Lipomas of the hand: a review and 13 patient case series. E-plasty. 2010;10:e66.
7. Mota FP, Díaz HFS, Hualda AL, Egea Gámez RM, García HV. Lipoma gigante bilobular en la mano: caso clínico y revisión de la literatura. Rev Iberoam Cir Mano. 2011;39(1):70-4.
8. Bruner JM. The zig-zag-volar-digital incision for flexor-tendon surgery. Plast Reconstr Surg. 1967;40(6):571-4.
9. Hsu CS, Hentz VR, Yao J. Tumours of the hand. Lancet Oncol. 2007;8(2):157-66.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}