


Guilherme Aron Teixeira Silva; Daysiane Rocha Souza; Karina Emburana Costa Parreiras; Janaíne Cunha Polese; Fernanda Souza da Silva
Submitted on: 05/08/2020
Approved on: 07/02/2021
Financial support: none
Conflit of interest: none
How to cite this article: Silva GAT, Souza DR, Parreiras KEC, Polese JC, Silva FS. Effectiveness of cryolipolysis for subcutaneous fat reduction: a systematic review and meta-analysis. Surg Cosmet Dermatol. 2021;13: e 20210004.
INTRODUCTION: Cryolipolysis produces selective, controlled cooling, and it’s based on the concept that lipid-rich tissue is more susceptible to cold injury, reducing subcutaneous fat.
OBJECTIVE: To review the literature to assess the effectiveness of cryolipolysis in reducing subcutaneous fat.
METHODS: Systematic review with meta-analysis of studies published in the EBSCOhost, LILACS, and PUBMED databases.
RESULTS: Only one study did not present significant reduction in subcutaneous fat compared to the control group. There was a difference among the parameters in the studies.
CONCLUSION: Cryolipolysis is an effective tool for localized fat reduction.
Keywords: Apoptosis. Freezing. Subcutaneous Fat
The fact that more than 56.3% of Brazilian adults are overweight or obese,1 in addition to the desire to quickly lose fat without undergoing surgery,2 drive the growing demand for fat reduction methods. In this scenario, cryolipolysis emerges as one of the most recently developed modalities for the noninvasive reduction of localized fat.3
The US Food and Drug Administration (FDA) authorized the first cryolipolysis device (CoolSculpting system, Zeltiq Aesthetics, Pleasanton, CA, USA) to reduce flank fat (K080521) in 2010; abdominal fat (K120023) in 2012; and inner thigh fat (K133212), in April 2014.4 According to Suh et al.,5 the use of cryolipolysis was also approved for inner thigh, submental fat, arms, back, and lower buttocks.
This technique produces selective and controlled cooling. It is based on the concept that lipid-rich tissues are more susceptible to cold injuries than the water-rich tissues around them.6 Adipocytes undergo apoptosis more quickly because they are sensitive to cooling than the dermis, epidermis, muscles, vessels, and nerves. These dead cells cause an inflammatory process and are metabolically eliminated as part of normal digestion.7 According to Avram and Harry,8 the changes are not noticeable immediately after the treatment. Therefore, adipocytes and cell membranes are not affected. However, three days after the intervention, there is evidence that an inflammatory process occurs only in adipocytes. Between 14 and 30 days, lipid phagocytosis is apparent, resulting in decreased tissue volume in 60 days.
According to the literature, this procedure is safe, with report of patient satisfaction, especially when compared to other methods for localized fat reduction.9 However, with all its benefits, there is still a lack of substantial literature demonstrating this tool’s effectiveness. Therefore, this study has the general objective of systematically review the available literature to assess the effectiveness of cryolipolysis in reducing subcutaneous fat. Its specific objectives are to determine the temperature values and the application time commonly used to reduce subcutaneous fat and search the literature if the temperature and cryolipolysis application time specified in the cryolipolysis equipment influences the subcutaneous fat reduction.
This study is a systematic review conducted according to the PRISMA methodology (Preferred Reporting Items for Systematic Reviews and Meta-Analysis).10 The guiding question of the present study was elaborated using the PICOS strategy: (P) individuals with subcutaneous fat, (I) cryolipolysis, (C) control group or placebo group, that is, who did not receive the cooling intervention, (O) subcutaneous fat reduction, and (S) randomized clinical trials.
We performed a systematic review search using the EBSCOhost, LILACS, and PUBMED databases. The search was conducted using the following terms: (tw:(cryolipolysis)) OR (tw:(lipocryolysis)) OR (tw:(fat freezing)) OR (tw:(coolsculpting)) OR (tw:(adipocytolysis)) OR (mh:(cryotherapy)) AND (mh:(adiposity)) OR (mh:(subcutaneous fat)) OR (tw:(fat reduction)) OR (tw:(fat)) OR (tw:(localized fat)) OR (mh:(body contouring)) OR (tw:(nonsurgical reduction of fat)) OR (tw:(noninvasive fat removal)) OR (tw:(noninvasive body contouring)). In addition to the electronic search, we performed a manual search in the bibliographic references of the previously selected studies.
Randomized clinical trials published between 2010 and 2019 in English, Portuguese, and Spanish, which had full text, were included. We selected the articles conducted in humans, both sexes, aged between 18 and 59 years old, analyzing cryolipolysis to reduce localized fat in the thigh, flank, abdomen, arm, or submental regions.
Review articles, animal research, studies that used another therapy combined with cryolipolysis aiming at localized fat reduction other than local massage were excluded. We also excluded studies with an intervention objective other than reducing localized fat and those that performed the treatment with cooling application three or more times in the same area.
Two researchers independently and blindly reviewed the titles and abstracts of potential articles and extracted the data. The selected titles and abstracts were submitted for a complete review. A third researcher was consulted when there were differences in the inclusion and exclusion of articles. The methodological quality of the studies was assessed using the PEDro scale, developed by the Physiotherapy Evidence Database to be used in experimental studies. According to Morton,11 the PEDro scale is a valid measure to assess the methodological quality of clinical trials. The scale has a total score of up to 10 points, including internal validity assessment criteria and presentation of the statistical analysis employed. For each criterion defined in the scale, one point (1) is attributed to indicators of the quality of the evidence, and zero (0) in the case of absence of these indicators. Two researchers applied the PEDro scale independently and blinded.
Statistical analysis was performed using the Review Manager (RevMan) program developed with the Cochrane collaboration. The characteristics of the samples between the studies were different, resulting in greater heterogeneity. In the case of significant statistical heterogeneity (I2>50%), a random-effect model n was used for the meta-analysis.
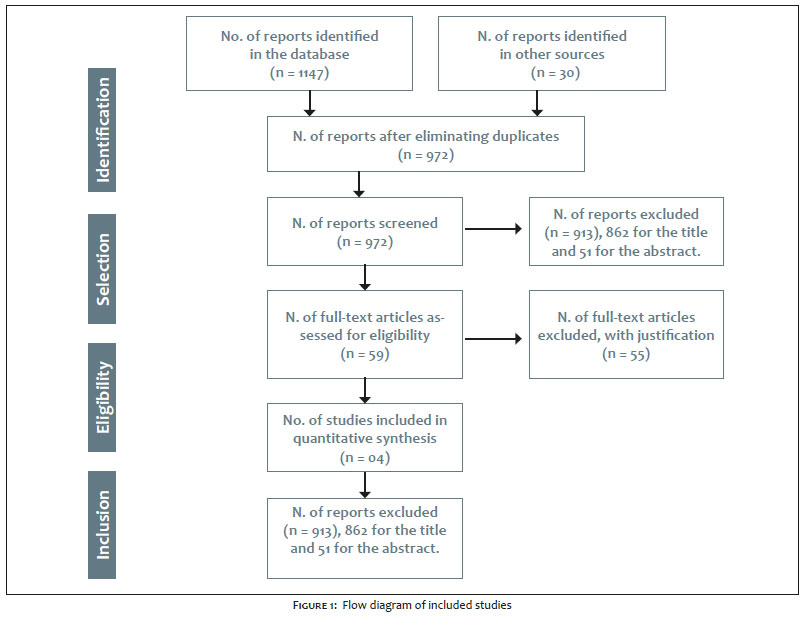
Searches in databases and other additional 30 studies identified through manual search resulted in 1,147 articles. After eliminating duplicates, 972 articles remained, of which 862 were excluded by title and 51 by abstract. Among the 59 articles assessed for eligibility, 55 were excluded because 22 were cohort studies, systematic or literature review, case report, or pilot study; 17 had participants’ ages incompatible with the inclusion criteria (over 59 years old); five were quasi-experimental studies; three studies used multiple treatments combined with cryolipolysis; two applied cryolipolysis to the breast and back region; one did not have cryolipolysis as primary endpoint; and five were not found for download or were not available. Thus, this systematic review included four articles (Figure 1). We found the highest percentage of articles (79.08%) in the PubMed database, followed by the EBSCOhost (11.68%) and LILACS (6.62%).
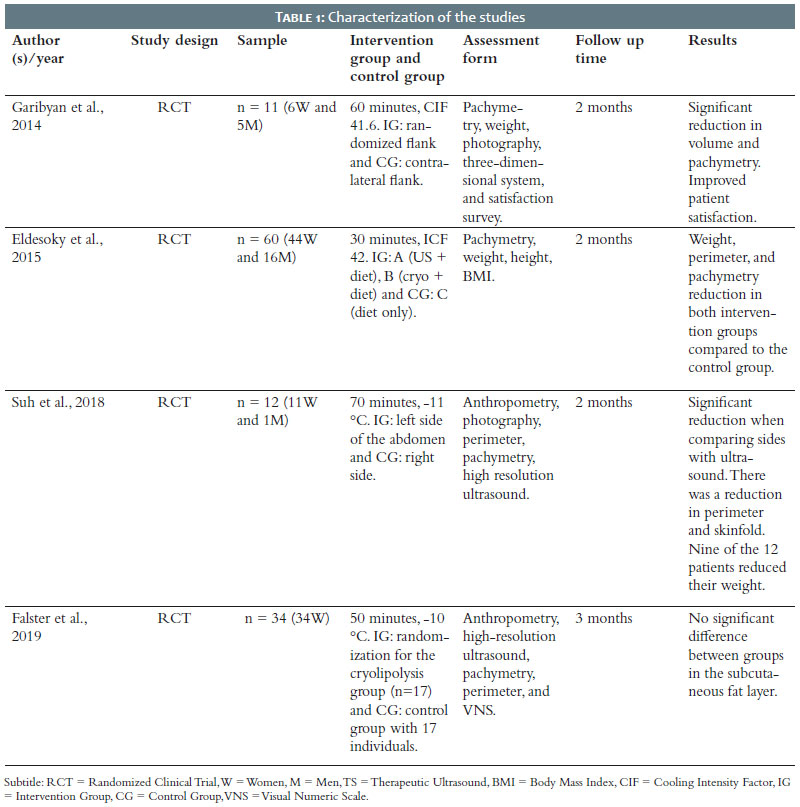
The four studies included in this review5,12,13,14 comprised a total of 117 participants, varying between 11 and 60 in each study. The sample was composed predominantly of women (81.20%), and the age ranged between 25 and 49 years. All studies assessed the cryolipolysis effect to reduce localized fat. The measurement instruments used were ultrasound,5 photography,5,13 visual analogue scale,14 satisfaction questionnaire,13 body mass index (BMI),12 anthropometry,5,14 pachymetry,12,13 perimetry,5,14 and weight.12, 13 The treated regions were abdomen5,12,14 and flank.13
All the studies analyzed showed a significant reduction in subcutaneous fat and/or a decrease in the localized fat circumference (Table 1), except for the study by Falster, et al.14 However, there was a difference regarding the parameters for applying cryolipolysis among studies.
When analyzing the cooling temperature adopted by the studies included in the present review, we observed that it varied by a few degrees and the way of adjusting the temperature in the equipment. Two studies adjusted the temperature in degrees Celsius, and two others in CIF, with a variation of 1 degree Celsius and 0.4 CIF, respectively.
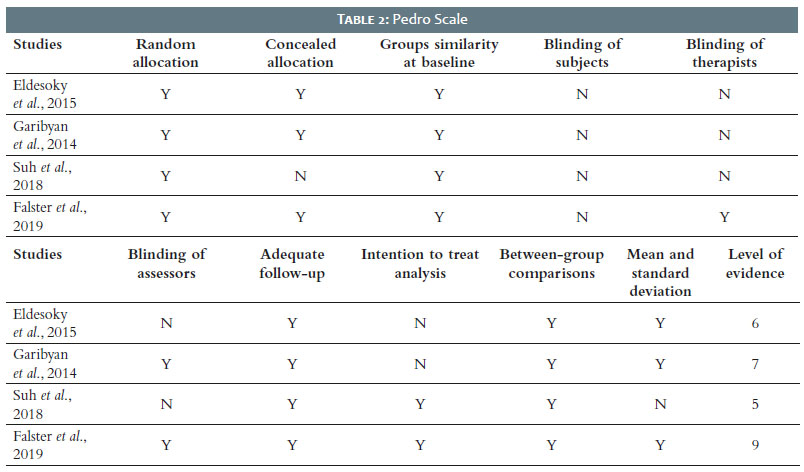
The average methodological quality assessed by the PEDro scale was 6.75, with no article scoring lower than five or higher than nine. The criteria with the highest deficit among the articles were related to the blinding of subjects, therapists, and assessors (Table 2).
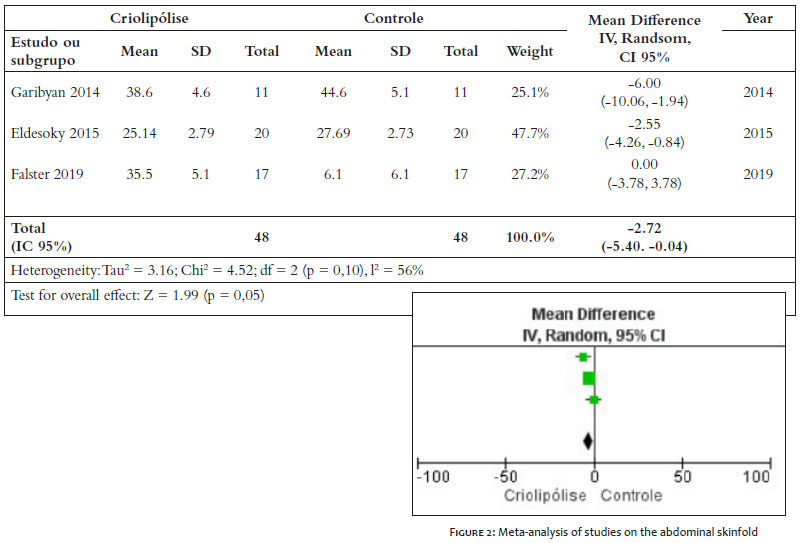
Also, we conducted a meta-analysis comparing three of the four studies in this review.12,13,14 These studies used an equivalent assessment method (pachymetry) to measure the abdomen and flanks skinfold. In total, 96 participants were included in the meta-analysis, 48 in the experimental group, and 48 in the control group. We observed a statistically significant 2.27 mm reduction in body fat (95% CI -5.40 to -0.04; Tau2 = 3.16; Chi2 = 4.52; I2 = 56%) in the intervention group compared to control (Figure 2).
Temperature and time values found in the articles were not standardized. Temperatures varying between -5 oC and -15 oC and time ranging from 30 to 60 minutes were commonly observed. The review by Borges and Scorza15 reported this variation, also describing that the temperature adjusted in the equipment is not the same as that observed in adipose tissue, mainly at deep levels. However, this effect is not harmful to the intervention. The authors also claim that, despite varying, the most used time in clinical practice is 60 minutes.
When searching the literature, it was not possible to find many articles relating the influence of time and temperature on reducing subcutaneous fat. However, in the study by Maia,16 53 individuals received an application of cryolipolysis in the lower abdominal region. Different from the temperature treatment applied in the Maia16 study, two groups (a total of four groups) received the treatment for 70 minutes. In this study, the protocol that showed the most significant results was the combination of a 70-minute time and variable temperatures (-5 °C and -8 °C). It corroborates the statement by Grivicich et al.,17 who stated that when the temperature decreases, there is a higher energy reserve expenditure (lipids) because of the increase in the metabolic rate. This theory indicates that the lower the temperature, the better localized fat reduction of due to the adipose tissue transformation from liquid (body temperature) to solid (post-cooling) (Limonta et al.).18
According to the study by Adjadj et al.19, cryolipolysis has become the gold standard for reducing subcutaneous fat in areas such as the abdomen, knees, flanks, inner thighs, back, and arms, being a good alternative for reducing subcutaneous tissue in patients with moderate fat. It corroborates the result found in the meta-analysis, where we observed the significance of the studies to apply cryolipolysis to reduce the subcutaneous skinfold. However, this decrease had an average of -2.72 (95% CI -5.40 mm to -0.04 mm), casting doubts regarding this method’s applicability to the clinical environment since this subcutaneous fat reduction is not essentially visible to the patient in the clinic.
Although there is no conformity on application time and temperature in most studies, cryolipolysis effectively reduces localized fat. The temperature varied between Celsius (-10 ° C and -11 ° C) and CIF (41.6 and 42); the application time varied between 30 and 70 minutes.
This systematic review included three studies that indicated significant results regarding subcutaneous fat reduction. The study by Garibyan et al.13 observed that, after two months of treatment, the mean reduced volume was 39.5 cm3 compared to the control side (p<0.01). The decrease in fat thickness was 14.9% on the treated side and 0.7% on the control side (p<0.01). Eldesoky et al.12 also pointed out significant results in the group receiving cryolipolysis and diet (group B). There was a body mass index reduction of 5.83% (p<0.01), a waist circumference of 6.47% (p<0.0001), and a suprailiac skinfold of 17.41% (p<0.01). Finally, the study by Suh et al.5 showed significant results when observing, through ultrasound, a decrease of 6.04 mm (standard deviation of 4.57 mm) in the treated abdomen (p 0.03). However, one study14 did not show significant results when comparing the control group with the experimental group in all evaluation methods. The fact that the average age and weight of the participants were lower than that found in the studies included in this research may explain this difference.
The studies by Garibyan et al.13 and Suh et al.5 used a system developed by Zeltiq Aesthetic Inc (Pleasanton, CA), which developed a unique temperature mechanism, named Cooling Intensity Factor (CIF), which represents the rate of heat flow into or out of the tissue opposite the cooling device.12 Both studies obtained significant results concerning subcutaneous fat reduction. The other studies included measured the temperature in degrees Celsius. The equipment currently available on the market has a temperature range of -5 °C to -15 °C.15
In the study by Eldesoky et al.12, low temperatures (CIF 42) demonstrated a significant result in the cryolipolysis technique regarding the fat thickness reduction, with a higher apoptotic lesion in the adipocytes. However, the study by Falster et al.,14 which used a temperature of -10 oC, did not obtain significant improvement results in any of the instruments assessed.
Regarding the application time, the study by Garibyan et al.13 used 60 minutes, with a reduction in flank volume and caliper measurements (p<0.01). In the study by Eldesoky et al.12, the cryolipolysis group used the therapy for 30 minutes and also obtained satisfactory results, such as significant decrease in weight, skinfolds, and circumference (p<0.01). The study by Suh et al.5 used 35 minutes, repeated twice, totaling 70 minutes of cryolipolysis application, obtaining a significant result of subcutaneous fat reduction (p=0.03). Finally, the study by Falster et al.14 applied cryolipolysis for 55 minutes, according to the protocol by Derrick et al.,20 not obtaining significant results (p>0.05), which can be explained by the difference presented in the age and weight of the participants regarding the other studies.
The literature shows that the protocols used for the cryolipolysis application vary from 30 to 60 minutes,13,15,21,22 and they present good statistical and clinical results. Only one article did not fit this pattern: the study by Suh et al.,5 which used cryolipolysis for 70 minutes, and was taken from the research by Kilmer et al.23 Also, the study by Falster et al.,14 even using the application time within the literature standards, did not obtain a significant result, making it challenging to analyze the direct relationship between the application time and better outcomes.
The adverse events of cryolipolysis found in the researches were: erythema after the session;13,19 skin hyperpigmentation;19 blisters in the treated area;12 edema;13 and pain.13 Among the adverse events, it was also observed that 100% of the participants had reduced sensitivity for 10 minutes after application, 73% after three weeks, and 18% in the second month after treatment.13 Several studies report these events after the cryolipolysis use. However, numerous researchers state that they occur in a short period and do not have significant repercussions.24,25
This research’s findings evidence the need for further studies in the area – studies with good methodological quality and standardized assessment instruments that allow conducting new meta-analyses, ensuring the safe application of cryolipolysis as a method to reduce subcutaneous fat. However, the study presented as limitations the failure to research all scientific databases and the inclusion of only articles published between 2010 and 2019, in English, Portuguese, Spanish, which had full text available.
The assessment method of areas submitted to cryolipolysis did not present conformity: the articles used parameters repeated in different authors or cited in a single study. However, as the meta-analysis demonstrated, cryolipolysis is an effective tool in reducing subcutaneous fat. Nevertheless, other studies with better methodological quality, investigating temperature and application time for subcutaneous fat reduction and presenting a standardization of assessment methods, should be proposed, given the scarcity in the literature.
Guilherme Aron Teixeira Silva | 0000-0002-2499-0147
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis; critical literature review.
Daysiane Rocha Souza | 0000-0003-4528-701X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis; critical literature review.
Karina Emburana Costa Parreiras | 0000-0003-4966-6252
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis; critical literature review.
Janaíne Cunha Polese | 0000-0003-3366-1545
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis; active participation in research orientation; critical literature review.
Fernanda Souza da Silva | 0000-0002-3161-2531
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis; active participation in research orientation; critical literature review.
1. Sa NNB, Moura EC. Excesso de peso: determinantes sociodemográficos e comportamentais em adultos, Brasil, 2008. Cad Saúde Pública. 2011;27(7):1380-92.
2. Mulholland RS, Paul MD, Chalfoun C. Noninvasive body contouring with radiofrequency, ultrasound, cryolipolysis, and low-level laser therapy. Clin Plast Surg. 2011;38(3):503-20.
3. Ingargiola MJ, Motakef S, Chung MT, Vasconez HC, Sasaki GH. Cryolipolysis for fat reduction and body contouring: safety and efficacy of current treatment paradigms. Plast Reconstr Surg. 2015;135(6):1581-90.
4. Lee SJ, Jang HW, Kim MH, Suh DH, Ryu HJ. Non-invasive cryolipolysis to reduce subcutaneous fat in the arms. J Cosmet Laser Ther. 2016;18(3):126-9.
5. Suh DH, Park JH, Kim BY, Lee SJ, Moon JH, Ryu HJ. Double stacking cryolipolysis treatment of the abdominal fat with use of a novel contoured applicator. J Cosmet Laser Ther. 2019;21(4):238-42.
6. Savacini MB, Bueno DT, Molina ACS, Lopes ACA, Silva CN, Moreira RG, et al. Effectiveness and safety of contrast cryolipolysis for subcutaneous-fat reduction. Dermatol Res Pract. 2018;(2):1-9.
7. Ferraro GA, Francesco F, Cataldo C, Rossano F, Nicoletti G, D'Andea F. Synergistic effects of cryolipolysis and shock waves for noninvasive body contouring. Aesthetic Plast Surg. 2012;36(3):666-79.
8. Avram MM, Harry RS. Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med. 2009;41(10):703-8.
9. Dierickx CC, Mazer JM, Sand M, Koenig S, Arigon V. Safety, tolerance, and patient satisfaction with noninvasive cryolipolysis. Dermatol Surg. 2013;39(8):1209-16.
10. Galvão TF, Pansani TSA. Principais itens para relatar revisões sistemáticas e meta- análises: a recomendação PRISMA. 2015;24(2):335-342.
11. De Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2):129-33.
12. Eldesoky MTM, Abutaleb EEM, Mousa GSM. Ultrasound cavitation versus cryolipolysis for non-invasive body contouring. Australas J Dermatol. 2016;57(4):288-93.
13. Garibyan L, Sipprell WH, Jalian RH, Sakamoto FH, Avram M, Anderson RR. Three-dimensional volumetric quantification of fat loss following cryolipolysis. Lasers Surg Med. 2014;46(2):75-80.
14. Falster M, Schardong J, Santos DP, Machado BC, Peres A, Rosa PV, et al. Efeitos da criolipólise na espessura da gordura abdominal inferior de mulheres saudáveis e satisfação do paciente: um estudo controlado randomizado. Rev Bras Fisio. 2019.
15. Borges FS, Scorza FA. Fundamentos da criolipólise. Fisio Ser. 2014;9(4):219-24.
16. Maia VRC. Desenvolvimento de um protocolo biomédico para a redução da adiposidade abdominal feminina utilizando a criolipólise. Curitiba. Dissertação [Programa de Pós- Graduação em Engenharia Biomédica] - Universidade Tecnológica Federal do Paraná; 2018. Available from: http://repositorio.utfpr.edu.br/jspui/handle/1/3402.
17. Grivicich I, Regner A, Rocha AB. Morte celular por apoptose. Revista Brasileira de Cancerologia. 2007;53(3):335-43.
18. Limonta AN, Ribeiro V da S, Gomes JPC, Moraes CAP. Criolipólise: a importância da membrana anticongelante na prevenção de queimaduras. InterfacEHS. 2017;12(1):128-43.
19. Adjadj L, SidAhmed-Mezi M, Mondoloni M, Meningaud JP, Hersant B. Assessment of the efficacy of cryolipolysis on saddlebags: a prospective study of 53 patients. Plast Reconstr Surg. 2017;140(1):50-7.
20. Derrick CD, Shridharani SM, Broyles JM. The safety and efficacy of cryolipolysis: a systematic review of available literature. Aesthetic Surg J. 2015;35(7):830-6.
21. Manstein D, Laubach H, Watanabe K, Farinelli W, Zurakowski D, Anderson RR. Selective cryolysis: a novel method of noninvasive fat removal. Lasers Surg Med. 2008 ;40(9):595-604.
22. Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J. Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plastic Surgery. 2009;33(4):482-8.
23. Kilmer SL. Prototype coolcup cryolipolysis applicator with over 40% reduced treatment time demonstrates equivalent safety and efficacy with greater patient preference. Lasers Surg Med. 2017;49(1):63-8.
24. Klein KB, Zelicson B, Riopelle JG, Okamoto E, Bachelor EP, Harry RS, Preciado JA. Non-invasive cryolipolysis for subcutaneous fat reduction does not affect serum liipid levels or liver function tests. Lasers Surg Med. 2009;41(10):785-90.
25. Stevens WG, Pietrzak LK, Spring MA. Broad overview of a clinical and commercial experience with cool sculpting. Aesthet Surg J. 2013;33(6):835-46.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}