


Ada Regina Trindade de Almeida1; Renata Sitonio T. D. Monteiro2
Submitted on: 10/11/2020
Approved on: 15/01/2021
Financial support: none
Conflit of interest: none
How to cite this article: Almeida ART, Monteiro RSTD. Hematoma in aesthetic surgery: tips to avoid unaesthetic results Hyaluronidase and hematoma drainage. Surg Cosmet Dermatol. 2021;13:e20210004.
Hematomas are common following cosmetic surgery. When minor, they are treated with observation only as they are most often reabsorbed. However, even with small collections of blood, if no early intervention is adopted, poor aesthetic outcomes may occur. Early drainage has been especially described in otorhinolaryngology and radiology journals. The authors present an approach to early treating hematomas. Special emphasis is given to the use of hyaluronidase, which is well known by dermatologists and plastic surgeons for its ability to dissolve hyaluronic acid, but its utility in the treatment of hematomas is not so commonly known by these experts.
Keywords: Hyaluronoglucosaminidase; Hyaluronic Acid; Hematoma; Fibrosis
Hematoma is a localized collection of blood. 1 It is relatively common after cosmetic surgeries. Unaesthetic results can be avoided if early interventions are performed to evacuate them. Small hematomas are usually reabsorbed spontaneously,2 but in some cases, they may induce poor aesthetic results. 2, 3
The hematoma course comprises 3 stages:
Stage I (early formation): The wound is swollen, warm, and fluctuant and requires immediate intervention.
Stage II - (gelatinous): formation of clotting.
Stage III - (organization): Blood clots within the hematoma.
Stage IV - (liquefaction): Fibrinolysis. Needle aspiration or puncture followed by manual expression may be considered.1
Hyaluronidase degrades hyaluronic acid. It has been used to treat fluid collections such as injected drugs and contrast media.4,5 Recently, it has been used to correct adverse events from hyaluronic acid fillers,6,7 but few studies have investigated its utility for treating hematomas.4,8
The goal of this article is to discuss how to treat post-procedure hematomas with the purpose of shortening the recovery time to prevent complications.
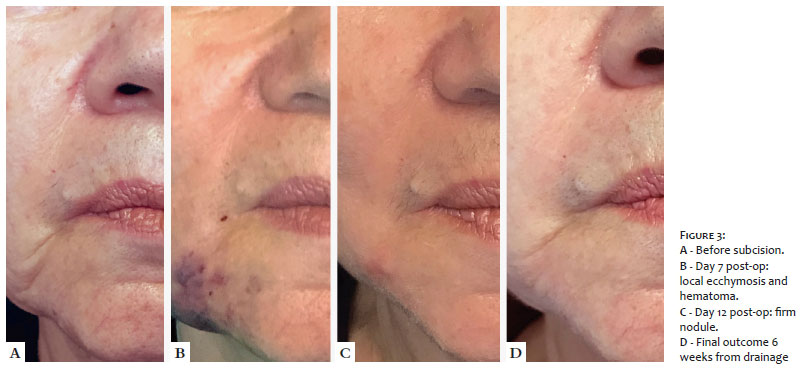
A 62-year-old woman underwent subcision to treat marionette lines. The needle was moved back and forth to form close parallel tunnels at dermal level, according to a subcision technique variant called “dermal tunneling”.9 On day 12 post-op she presented with firm local bumps on the treated area (Figure 1), which were punctured with a 22G needle and the blood was drained.
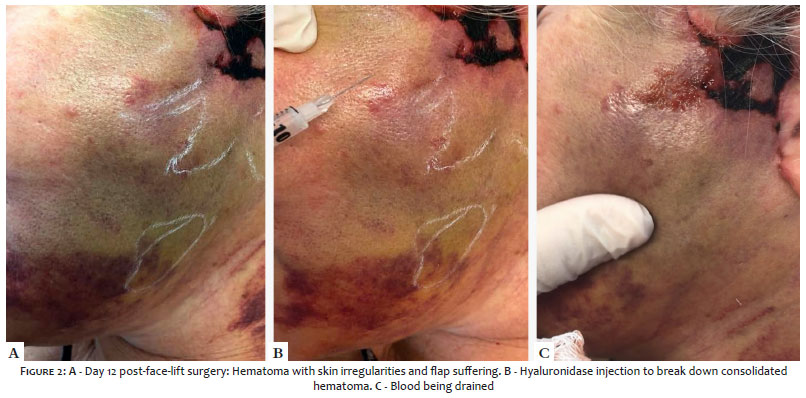
A 65-year-old woman underwent face-lift surgery and developed larges hematomas. She asked for our evaluation and intervention. On Day 12 post-op, the pre-auricular area was tender and partial scar dehiscence and necrosis had occurred. Although theoretically liquefaction phase was ongoing,1 the drainage was difficult to perform. Hyaluronidase was indicated to help break down the hyaluronic acid within the coagulated hematoma.4 Therefore, 2ml of hyaluronidase, reconstituted with 5 ml of diluent to a final concentration of 400u/ml, were injected into the indurated areas followed by fingertip massage. The skin was then punctured with a 22G needle and manual expression of the blood was made (Figure 2).
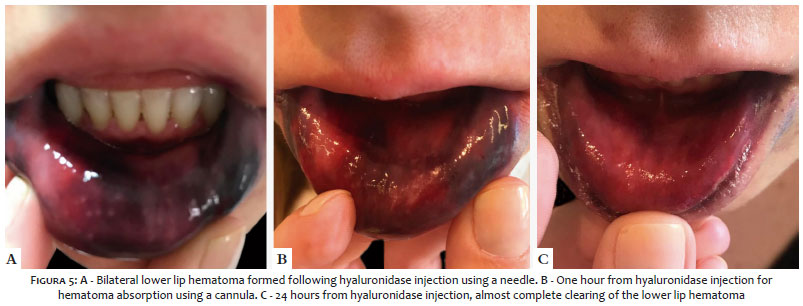
A 30-year-old woman had her lips injected with hyaluronic acid. Right after the procedure, the injecting physician noticed an area of impending necrosis characterized by pale skin on the right side of her lower lip, suggesting vascular occlusion. Hyaluronidase was immediately injected through several punctures and improvement of the pale area was observed. However, this procedure induced vascular injury and a large new hematoma emerged. The hematoma pressure was collapsing the vessels, leading to – once again –impending skin necrosis. In order to dissolve the hematoma and improve local blood flow, 2 ml of hyaluronidase (400u/ml) were injected, with 25G cannula. Fingertip massage was performed to help hyaluronidase break the clot and enhance fluid absorption.4
Within 6 weeks, there were no more nodules and local improvement of wrinkles and laxity could be observed (Figure 3).
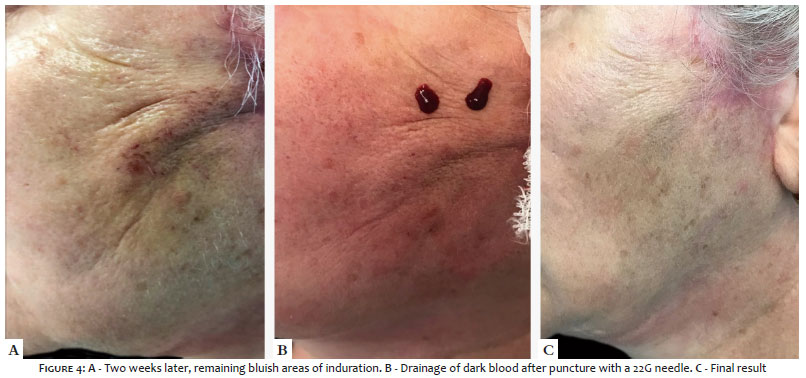
Immediately after treatment, the patient felt less discomfort. The wound started to heal on the following days. Two weeks later, small areas of localized blue-colored skin indurations were punctured again. Immediately after the procedure, the bluish color disappeared as well as the indurations (Figure 4).
One hour after the hyaluronidase injection, the purple color on her lip cleared and 24 hours later, almost complete resolution of the hematoma occurred (Figura 5).
Subcision is a procedure used to release fibrous attachments. Indications are correction of acne scars, cellulite dimples, and wrinkles, inducing formation of connective tissue through normal physiological healing. 9,10, 11 One of its adverse effects are residual indurations. Around 5-10% of patients develop hypertrophic response within 2-4 weeks post-operatively,9 especially in the glabellar region. This happens due to an exaggerated wound healing response or to an unrecognized and untreated hematoma 3 that can evolve to hypertrophic scars. Hence, the importance of recognition and early treatment of hematomas to prevent nodule formation.
Some authors advocate that patients are not bothered by the bumps.11 This is not our experience. We recommend early drainage of local hematomas in order to prevent or reduce the duration of these residual bumps, preventing posterior fibrosis, thus enhancing patient´s satisfaction.
Hematomas may lead to flap necrosis after face-lift surgeries, resulting in unaesthetic scars.2 Even being of small size, they may jeopardize the flap viability, leading to knots, necrosis, skin irregularities, hyperpigmentation and prolonged healing time.2
The ideal moment to drain the hematoma is when it is in the liquefaction phase.1
Hyaluronidase has been used for several years to enhance the absorption of extravasated fluids, 4,5,8 and recently, to correct HA adverse events. 7 But it would also degrade the hyaluronic acid deposited throughout the consolidated hematoma and extracellular matrix. 4 Thus, hyaluronidase may help break down the coagulated hematoma and facilitate the fluid drainage by creating outflow channels in the extracellular matrix, even when it is in its firm or gelatinous form. 4
Although this usage is off label, we feel it could help avoiding complications.
In an experimental study, Chuang injected blood in a dog’s abdominal wall to simulate bilateral hematomas. One side was treated with hyaluronidase injection and the other was left as a control. One hour from injection, the treated side showed 70% reduction of its size when compared with the control. The favorable results in animals allowed the use of hyaluronidase to treat patients with moderate-to-large hematomas following arterial catheterization in angiographic procedures. Positive effects were observed as early as 5-10 minutes from injection, while most patients responded after one hour by showing reduction and softening of the hematomas.8 Nelson et al. suggested using hyaluronidase as a tool to allow early reabsorption of facial and neck hematomas.4
Hyaluronidase was very useful in our post-rhytidectomy hematoma case, by inducing blood clot liquefaction, allowing its early release, and keeping flap viability.
It was also very effective in dissolving the lip hematoma that occurred after filler injection. To our knowledge, the use of hyaluronidase to make the reabsorption of lip hematomas easier had not been described before.
Hyaluronidase may help treat hematomas at early gelatinous and consolidation phases, thus reducing the risks of complications as well as patient’s downtime.
Hematoma is a frequent occurrence following surgical procedures. Observation is often adopted. But, in some cases, they may course with complications. The authors propose early intervention with drainage when in the liquefaction phase or by hyaluronidase injection when consolidated in order to reduce patient discomfort, downtime and to prevent poor aesthetic outcomes. Although the use of hyaluronidase is reported in other specialties journals, such use is still little known by dermatologists and plastic surgeons, who would benefit from this new indication.
Ada Regina Trindade de Almeida | 0000-0002-4054-2344
Final version approval of manuscript, study design and planning, Elaboration and writing, Obtaining, analyzing and interpreting the data, Effective participation in research guidance, Intellectual participation in propaedeutic and / or therapeutic conduct of studied cases, Critical review of the manuscript.
Renata Sitonio T. D. Monteiro | 0000-0001-8991-958X
Final version approval of manuscript, Elaboration and writing, Obtaining, analyzing and interpreting the data, Critical literature review, Critical review of the manuscript.
1. Bunick CG, Aasi SZ. Hemorrhagic complications in dermatologic surgery. Dermatol Ther. 2011;24(6):537-50.
2. Niamtu J III. Expanding hematoma in face-lift surgery: literature review, case presentations, and caveats. Dermatol Surg. 2005;31(9 Pt 1):1134-44.
3. Han JH, Kim J, Yoon KC, Shin HW. Treatment of post-traumatic hematoma and fibrosis using hyaluronidase injection. Arch Craniofac Surg. 2018;19(3):218-21.
4. Nelson RE, Carter JM, Moulthrop THM. Hyaluronidase injection for the treatment of facial and neck hematomas. Laryngoscope 2015;125(5):1090-2.
5. Lee A, Grummer SE, KriegeL D, Marmur E. Hyaluronidase. Dermatol Surg. 2010;36(7):1071-7.
6. Trindade de Almeida AR, Saliba AF. Hyaluronidase in cosmiatry: what should we know? Surg Cosmet Dermatol. 2015;7(3):197-204.
7. Almeida ART, Banegas R, Boggio R, Bravo B, Braz, A, Casabona G, et al. Diagnosis and treatment of hyaluronic acid adverse events: latin american expert panel consensus recommendations. Surg Cosmet Dermatol. 2017;9(3):204-13.
8. Chuang V. Hyaluronidase for the treatment of hematoma at an angiopathic puncture site. Radiology. 1983;146(1):227.
9. Lima EVA. Dermal tunneling: a proposed treatment for depressed scars. An Bras Dermatol. 2016;91(5):697-99.
10. Orentreich DS, Orentreich N. Subcutaneous incisionless [subcision] surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543-9.
11. Alam M, Omura Nayomi, Kaminer, MS. Subcision for acne scarring: technique and outcomes in 40 patients. Dermatol Surg. 2005;31(3):310-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}