


Maria Carolina Casa Souza; Fernando Eibs Cafrune
Received on: 02/03/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Hospital Complex Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil
Introduction: Facial skin cancer can be very challenging to surgical treatment. Reconstruction with cervicofacial flap is an adequate option when extensive damage is present. We describe a surgical procedure for complex lesions with high morbidity potential. Case study: 69-year-old woman with a large, recurring sclerodermiform basal cell carcinoma (BCC) in the left zygomatic area. Due to the lesion characteristics, we opt to perform Mohs surgery. A cervicofacial flap was used with good aesthetic results and no relapse. Discussion: The cervicofacial flap is ideal for extensively damaged areas and can be used as an alternative to skin graft.
Keywords: Carcinoma, Basal Cell; Mohs Surgery; Surgical Flaps
Basal cell carcinoma (BCC) is the most common type of skin cancer. Among its subtypes, sclerodermiform BCC is responsible for approximately 5% to 10% of the cases. It is called sclerodermiform because of its clinical similarity with plaque morphea or localized scleroderma. The condition is usually more aggressive than nodular and superficial subtypes. It tends to present subclinical spread with potential for extensive local dissemination.1,2 Surgical treatment is recommended for most of these carcinomas, and Mohs micrographic surgery is the method of choice. The technique is preferred for high-risk, recurrent, large-sized tumors and facial location. Its main advantage is to provide precise microscopic control of the entire margin of the tumor, maximizing the conservation of healthy tissue.3
During the performance of both Mohs micrographic surgery and the conventional technique, one of the most significant challenges is to repair the surgical defect while obtaining a good esthetic and functional result.4 In cancer cases in the malar, maxillary, and periorbital regions for more than 30 years, the literature has described the reconstruction technique with cervicofacial flap. Conceptually, it is a flap that explores the flaccidity of the skin of the cheek, pre-auricular, and neck regions. Its main advantage is maintaining the color and texture of the native tissue. Another advantage is that the method positions the incisions in areas of natural grooves, respecting the limits of facial aesthetic subunits. In some cases, this flap also allows adequate exposure of the cervical and facial structures for additional cancer procedures, such as lymph node dissection.5
We present a case of cervicofacial flap following Mohs surgery with multiple stages for excision of a sclerodermiform BCC in the left zygomatic region. The case proves challenging because of the large dimensions of the surgical wound and its location. A surgical option for complex lesions on the face and with great potential for morbidity has been demonstrated.
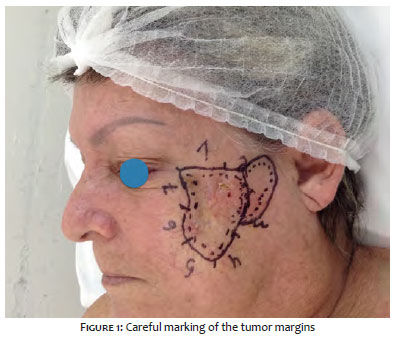
A 69-year-old woman was diagnosed with recurrent sclerodermiform carcinoma in the left zygomatic region that appeared more than ten years ago. She had undergone two previous (conventional) surgeries and treatment with radiotherapy with posterior recurrence of the lesion. The examination showed an erythematous plaque, infiltrated about 4.5 centimeters in its largest diameter, with multiple telangiectasias in dermoscopy and a small central crust. We chose the Mohs surgery (Figure 1) with local anesthesia and sedation. Free margins were obtained after four stages of additional 5 mm each. The resulting defect measured 6.5 x 7.5 cm, affecting the malar, pre-auricular, and left temporal regions (Figure 2). We used a cervicofacial transposition flap to repair the defect. The transposition arch was drawn up to the mandible, ipsilateral retroauricular, and cervical regions (Figure 3). The flap was elevated and transposed from the retroauricular and cervical regions to the surgical defect (Figure 4).
The flap was fixed with vicryl 4-0 (suture anchorage) in the zygomatic region and subcutaneous suture, and 5-0 mononylon thread for superficial cutaneous suture. We close the secondary defect primarily in the posterior portion, and by secondary intention in the retroauricular and mid-cervical regions (Figure 5).
External sutures were removed after 15 days. In the postoperative period, the patient presented a small focus of necrosis in the upper scar region, with improvement after debridement in about five weeks. After two months, the patient had a good healing. The patient currently presents a one-year postoperative period without signs of recurrence of the lesion and maintains a good result (Figure 6).
Skin flaps are necessary resources for closing skin tumor excisions.6 Transposition flaps are versatile and can be used anywhere on the face. They recruit tissues from different regions, resulting in color and texture compatible with the defect area, especially when coming from nearby areas. The skin abundance in the neck and retroauricular areas make the use of these flaps an attractive option for reconstructions in the mid-lateral region of the face.7 On the face, the smooth and harmonic reconstruction remains challenging. The procedure must not only recover the facial function, but it also has to present a good aesthetic result, avoiding ectropion formations and, mainly, injury to the facial nerve.
When making the flap, after emerging from the parotid gland 1.7 cm before the tragus, the temporal branch of the facial nerve crosses the zygomatic arch between 3.2 cm and 3.9 cm posterior to the lateral border of the orbit, at the level of the orbital-tragus line, which corresponds to the middle third of the zygomatic arch. There is vulnerability of the temporal branch at the middle third of the zygomatic arch. However, although this branch of the facial nerve presents a wide pattern variation, its direction is constant. It allows the definition of a safe dissection plane for the temporal region.8
Cervicofacial flap is ideal for significant defects that can’t be repaired with small local tissue mobilization, allowing reconstruction without the need for grafting.9 Its versatility and good rotation arc allow this flap to cover large areas of a surgical wound.5 However, the main disadvantage of this type of flap is the possibility of distal ischemia, which can lead to necrosis, primarily when the flap is sutured with tension due to defect extension or when the patient already has some disease that could compromise the local microcirculation.10 In the present case, the patient had already presented numerous lesion recurrences, requiring several stages of Mohs surgery to obtain free margins. It led to an extensive surgical defect that was adequately corrected with the cervicofacial flap, with no evidence of recurrence after one year of surgery.
Maria Carolina Casa Souza 0000-0002-8241-8376
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Fernando Eibs Cafrune | 0000-0002-6645-0122
Active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Midgen MR, Chang ALS, Dirix L, Stradigos AJ, Lear JT. Emerging trends in the treatment of advanced basal cell carcinoma. Cancer Treat Rev. 2018;64:1-10.
2. Marzuka AG, Book SE. Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. Yale J Biol Med. 2015;88(2):167-79.
3. Patel TN, Patel SB, Franca K, Chacon AH, Nouri K. Mohs micrographic surgery: history, technique, and advancements. Skinmed. 2014;12(5):289-92.
4. Grosfeld EC, Smit JM, Krekels GA, van Rappard JH, Hoogbergen MM. Facial reconstruction following Mohs micrographic surgery: a report of 622 cases. J Cutan Med Surg. 2014;18(4):265-70.
5. Sakellariou A, Salama A. The use of cervicofacial flap in maxillofacial reconstruction. Oral Maxillofac Surg Clin North Am. 2014;26(3):389-400.
6. Kondo RN, Pontello Júnior R, Lopes VCH, Bittar RA, Pereira AM. Retalho de interpolação para fechamento de defeito cirúrgico em lóbulo de orelha. Surg Cosmet Dermatol. 2012;4(2):192-4.
7. Pletcher SD, Kim DW. Current concepts in cheek reconstruction. Facial Plast Surg Clin North Am. 2005;13(2):267-81.
8. Rendon NB, Barazzetti PHO, Garcia CP, D'Avila AK, Vasconcelos ZAA, Ely JB. Retalho cervicofacial composto: uma alternativa para reconstrução facial. Rev. Bras. Cir. Plást. 2018;33:114-6.
9. Ebrahimi A, Nejadsarvari. Experience with cervicofacial flap in cheek reconstruction. J Craniofac Surg. 2013;24(4):372-4.
10. Saito N, Tsutsumida A, Furukawa H, Sekido M, Oyama A, Funayama E, et al. Reconstructive considerations in the treatment of soft tissue sarcomas of the cheek. Acta Otorhinolaryngol Ital. 2010;30(2):103-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}