


Adriana de Carvalho Corrêa1,2,3; Daniela Alves Pereira Antelo3
Received on: 06/03/2020
Approved on: 01/12/2020
Financial support: None
Conflict of interest: None
Study conducted at the Dermatology Service of the Pedro Ernesto University Hospital, of the Universidade do Estado do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
Atrophic acne scars are persistent and undesirable sequelae that have a negative cosmetic and psychosocial impact on patients. This issue becomes more delicate when such scars are located in the presternal region due to the risk of hypertrophic scars appearing when performing these procedures in the area. The literature has long recognized the role of insulin in promoting protein and fat synthesis. Insulin properties as a growth factor to treat these sequelae seems logical and has proved cosmetically satisfying, with quality of life improvement.
Keywords: Acne Vulgaris; Atrophy; Scar; Wound healing; Injections, subcutaneous; Insulin; Ambulatory surgical procedures; Quality of life; Tissue therapy
Acne scars have a negative impact on the quality of life and lead to feelings of shame and low self-esteem.1,2 Destruction of the extracellular matrix (ECM) components at the beginning of acne lesions is a foundation for the resulting atrophic scars.3 Jacob et al. classified this pattern of scars into the three basic types: icepick (<2 mm, narrow scars that taper as they extend to the deep dermis), rolling (4-5 mm, the depressed scars with sloping and shallow edges), and boxcar (1.5–4 mm, round to oval depressions with markedly demarcated vertical limits).1,4 There are several treatments to mitigate these scars.1,3 However, the pre-sternal region presents a tendency to hypertrophic scarring,5 discouraging the aggressive approach. Few observations of subcutaneous insulin administration suggest a good response in atrophic scars.6-8
A 20-year-old man (ACC) with no morbidities presented rolling and boxcar atrophic acne scars. The scars were distensible and hypochromic in the pre-sternal region.
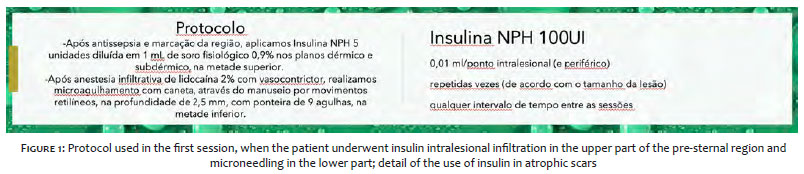
We divided the sternal region into two parts (upper and lower) and applied 5 units of NPH insulin, according to the protocol described in Figures 1 and 2. We observed petechiae, erythema, and edema after microneedling.
One week later, the treated area presented hyperemia and hyperchromia, in addition to partial improvement of some scars. Given the clinical improvement, we applied NPH insulin over the entire length of the lesion.
On each session, up to 15 units of NPH insulin were infused due to the extent of the lesions. Eleven sessions were held, with a weekly interval. There were no adverse events such as hypoglycemia or lipothymia.
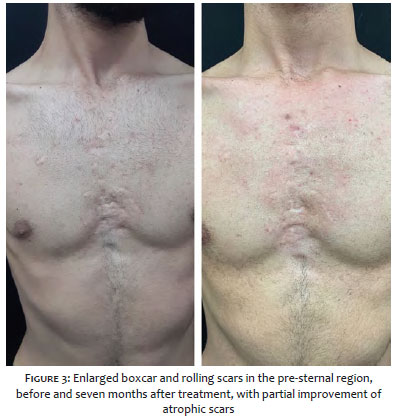
The patient presented a satisfactory result, with improvement in atrophy, as showed in the follow-up photographs after seven months (Figures 3 and 4).
Insulin is a peptide hormone and growth factor with numerous physiological roles. In addition to the regulation of serum glucose levels, it plays a promoting role in wound healing.9 We know that its deficiency slows tissue repair. Burned patients submitted to its systemic administration evolve with lesion improvement, in part, by improving the local protein balance.10 However, systemic administration generates metabolic changes and imbalances (hypoglycemia and hypokalemia) that limits its use.10
Insulin topical administration has been described in animal models and clinical trials.11-13 The local insulin application prevents systemic repercussions while maintaining its beneficial action on local healing. Liu et al. observed that insulin acts through its receptors, helping in the migration of keratinocytes in wounds without interaction with epidermal growth factor receptors.14 It is believed that the direct action on fibroblasts and keratinocytes, cells in which the presence of the insulin receptor has been identified, mediates its effect.9
Evidence from the literature suggests the role of insulin in regulating energy metabolism, protein synthesis, cell differentiation, and growth. Thus, its local injection promotes the granulation tissue’s growth and development, with consequent healing.15-18
Insulin stimulates the incorporation of (3H) thymidine in the skin’s fibroblasts, resulting in collagen synthesis.19 Topically, it accelerates wound healing in diabetes by improving the Protein Kinase B (AKT) and Extracellularly Regulated Kinase (ERK) pathways. It is assumed that insulin uses these two routes to increase repair.16 Upon connecting to the receptor, the intracellular tyrosines located in its b-subunits are phosphorylated and allow the Src 2 homology and collagen-A protein, found in the cytosol, to bind through the Src-214 homology domains. The signal is transduced through a series of messenger molecules to activate Ras (a member of a large family of small molecular weight GTP binding proteins)16 and transmitted via Raf, MEK (members of the GTP binding protein family), and ERK.20 It moves to the nucleus, where the cell receives the command to replicate DNA and multiply, with consequent tissue repair and wound healing.9 In the other pathway, the insulin receptor substrate 1 and 2 binds to it and transduces the signal via PI (3) kinase, PDK, and AKT. Such a reaction induces nitric oxide (NO) production, increased blood flow, cell survival, morphogenesis, and angiogenesis. The increase in phosphorylation of GSK-3β (Glycogen Synthase Kinase-3β) by AKT decreases its activity, which may be another mechanism to increase collagen production, reduce apoptosis, and accelerate wound closure.21
The insulin-like growth factor-1 (IGF-1) stimulates the production of an extracellular matrix component22 and induces the transformation factor-beta (TGF-β) in dermal fibroblasts, corroborating wound healing.23,24
Collens first described the reversing diabetic lipoatrophy technique by injecting the purest forms of insulin.25 Insulin is an anabolic hormone in the metabolism of fats and proteins. Adipose tissue is exquisitely sensitive to insulin; minimal amounts can inhibit lipolysis6 and promote the synthesis of proteins and fats.7
Amroliwalla administered subcutaneous insulin injections and achieved complete post-vaccine atrophic scars regression.6 Likewise, Kalil-Gaspar et al. achieved complete lesions remission in lipoatrophy inducing insulin and corticosteroids, respectively.7 Hallam et al. conducted a randomized controlled study to assess the potential of insulin as an anti-scar therapy, analyzing patients undergoing bilateral cosmetic breast operations. They observed that subcutaneous injections into scars reduced their appearance compared to placebo and suggested that the properties of insulin in lowering scars were more effective in individuals who were at risk of excessive or pathological scarring.8
Faced with a very distressed patient presenting extensive boxcar and rolling scars in the pre-sternal region, insulin infiltration, a technique overlooked by many dermatologists, could benefit tissue recovery. The most significant advantage of the method would be the ease of finding the drug and its cost. Moreover, its major disadvantage would be the need to repeat the scheme for a long period. Our patient was treated with weekly intralesional infiltration sessions for three months. The studies of Amroliwalla6 and Kalil-Gaspar7, which maintained therapy with daily frequency and an average time of 90 days, indicated continuity for a longer period. However, the patient was a university student and would be hindered from attending the clinic in the coming months for academic reasons. After seven months (free of treatment), although there is great difficulty in photographic documentation (two-dimensional) of normochromic atrophic scars, the patient and the attending physicians observed genuine lesions improvement. Today’s use of purer insulin forms can explain the maintenance of results without the long-term lipoatrophy produced by insulin in the past.
Insulin increases protein synthesis in the skin and stimulates the growth and development of different cell types. It also affects the proliferation, migration, and secretion of keratinocytes, endothelial cells, and fibroblasts.26,27 Therefore, it can correct keratinocyte proliferation blockade and replace excessively destroyed collagen, which would help recover some of the defects responsible for atrophic acne scars.3 It is interesting for wound care and scarring treatment, mainly because of its low cost compared to other growth factors and its universal availability. Further studies are needed to better understand insulin’s role in wound healing and more precisely outline which individuals can benefit from anti-scar insulin therapy.
Adriana de Carvalho Corrêa | 0000-0002-6519-0971
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Daniela Alves Pereira Antelo | 0000-0001-8203-1772
Critical revision of the manuscript.
1. Boen M, Jacob C. A review and update of treatment options using the acne scar classification system. Dermatol surg. 2019;45(3):411-22.
2. Dréno B. Assessing quality of life in patients with acne vulgaris: implications for treatment. Am J Clin Dermatol. 2006;7(2):99-106.
3. Moon J, Yoon JY, Yang JH, et al. Atrophic acne scar: a process from altered metabolism of elastic fibres and collagen fibres based on transforming growth factor-β1 signalling. Br J Dermatol, 2019;181(6):1226-37.
4. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45(1):109-17.
5. Meyer M, McGrouther DA. A study relating wound tension to scar morphology in the pre-sternal scar using langers technique. Br J Plast Surg. 1991;44(4):291-94.
6. Amroliwalla FK. Vaccination scar with soft-tissue atrophy restored by local insulin treatment. Br Med J. 1977;1(6073):1389-90.
7. Kalil-Gaspar N, Gaspar AP, Moreira AFB, Travasso Neto P. Tratamento de lipoatrofias localizadas com insulina monocompetente. An Bras Dermatol. 1984;59(3):135-6.
8. Hallam MJ, Pitt E, Thomas A, Nduka C. Low-dose insulin as an antiscarring therapy in breast surgery: a randomized controlled trial. Plast reconstr surg. 2018;141(4):476e-485e.
9. Hrynyk M, Neufeld RJ. Insulin and wound healing. Burns. 2014;40(8):1433-46.
10. Zhang XJ, Chinkes DL, Sadagopa Ramanujam VM, Wolfe RR. Local injection of insulin-zinc stimulates DNA synthesis in skin donor site wound. Wound repair regen, 2007;15(2):258-65.
11. Greenway SE, Filler LE, Greenway FL. Topical insulin in wound healing: a randomised, double-blind, placebo-controlled trial. J Wound Care. 1999;8(10):526-8.
12. Pierre EJ, Barrow RE, Hawkins HK, et al. Effects of insulin on wound healing. J trauma. 1998;44(2):342-45.
13. Weringer EJ, Kelso JM, Tamai IY, Arquilla ER. Effects of insulin on wound healing in diabetic mice. Acta Endocrinol. 1982;99(1):101-108, 1982.
14. Liu Y, Petreaca M, Yao M, Martins-Green M. Cell and molecular mechanisms of keratinocyte function stimulated by insulin during wound healing. BMC Cell Biol. 2009;10:1.
15. Malaguarnera R, Belfiore A. The emerging role of insulin and insulin-like growth factor signaling in cancer stem cells. Front Endocrinol. 2014;5:10.
16. Lima MHM, Caricilli AM, Abreu LL, et al. Topical insulin acelerates wound healing in diabetes by enhancing the AKT and ERK pathways: a double-blind placebo-controlled clinical trial. PLoS One. 2012;7(5):e36974.
17. Jiang H, Torregrossa AC, Potts A, et al. Dietary nitrite improves insulin signaling through GLUT4 translocation. Free Radical Biol Med. 2014;67:51-7.
18. Han JK, Kim HL, Jeon KH, et al. Peroxisome proliferator-activated receptor-δ activates endothelial progenitor cells to induce angio-myogenesis through matrix metallo-proteinase-9-mediated insulin-like growth factor-1 paracrine networks. Europ Heart J. 2013; 34(23):1755-65.
19. Verhofstad MH, Bisseling TM, Haans EM, Hendriks T. Collagen synthesis in rat skin and ileum fibroblasts is affected differently by diabetes-related factors. Int J Exp Pathol. 1998;79(5):321-8.
20. Gallagher KA, Liu ZJ, Xiao M, et al. Diabetic impairments in NO-mediated endothelial progenitor cell mobilization and homing are reversed by hyperoxia and SDF-1α. J Clin Invest. 2007;117(5):1249-59.
21. Kapoor M, Liu S, Shi-Wen X, et al. GSK-3β in mouse fibroblasts controls wound healing and fibrosis through an endothelin-1-dependent mechanism. J Clin Invest. 2008;118(10):3279-90.
22. Yu Y, Chai J. The function of miRNAs and their potential as therapeutic targets in burn-induced insulin resistance (Review). Int J Mol Med. 2015;35(2):305-10.
23. Ghahary A, Shen Q, Shen YJ, Scott PG, Tredget EE. Induction of transforming growth factor β1 by insulin-like growth factor-1 in dermal fibroblasts. J Cell Physiol. 1998;174(3):301-9.
24. Sridharan K, Sivaramakrishnan G. Efficacy of topical insulin in wound healing: a preliminary systematic review and meta-analysis of randomized controlled trials. Wound repair regen. 2017;25(2):279-87.
25. Collens WS, Boas LC, Zilinsky JD, Greenwald JJ. Lipoatrophy following the injection of insulin. New Eng J Med. 1949;241(16):610.
26. Brem H, Tomic-Canic M. Cellular and molecular basis of wound healing in diabetes. J Clin Invest. 2007;117(5):1219-22.
27. Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. 2008;453(7193):314-321.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}