


Dalv a Regina Neto Pimentel; Rafael Tomaz Gomes; Cleonic e Hirata
Received on: 07/08/2020
Approved on: 02/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the no Stomatology Outpatient Clinic, Department of Dermatology of the Escola Paulista de Medicina (UNIFESP).
INTRODUCTION: The venous lake is a venous ectasia that usually occurs on the lips and oral mucosa of the elderly. Although sclerotherapy is one of the most suitable treatments for this condition, dermatologists don't use this technique very often. Also, the concentration of the sclerosing agent, dose, and method of application are not standardized.
OBJECTIVES: This study aims to report the use of ethanolamine oleate 5% (EO5%) as a sclerosing agent to treat the oral venous lake and suggest a sclerotherapy protocol.
METHODS: We used a standardized protocol to treat an oral venous lake in ten consecutive patients, based on the experience of a University Dermatology Clinic, specialized in Stomatology. EO5% was applied in deep and central intralesional injections, with a predetermined volume proportional to the lesion’s dimensions. Results: Six patients had total lesion regression with one session. Another three patients achieved satisfactory regression with two monthly sessions, and one patient required three monthly sessions. All participants reported edema or burning for one to three days.
CONCLUSION: The oral venous lake treatment with EO5% is a safe and effective technique that can be used in the dermatologist's clinical practice.
Keywords: y, Venous Lake, Ethanolamine Oleate.
The venous lake is a venous ectasia that appears mainly on the lower lip, but it can also occur on the oral mucosa, being more frequent in the elderly1. It is generally asymptomatic, of variable size, and may present with aesthetic impairment or bleeding after local trauma.1,2
Sclerotherapy is a conservative technique consisting of intralesional injection of sclerosing agents that lead to inflammation of the vessels followed by occlusion and vascular sclerosis, resulting in lesion regression.2,3
Although sclerotherapy is affordable, effective, and has a low risk of complications, the concentration of the sclerosing agent, dose, and method of application are not entirely standardized in the treatment of the venous lake.4,5
This article aims to report the use of 5% ethanolamine oleate (OE5%) as a sclerosing agent for the treatment of the oral venous lake, both on the lip and oral mucosa, and to suggest a sclerotherapy protocol based on the experience of our clinical center.
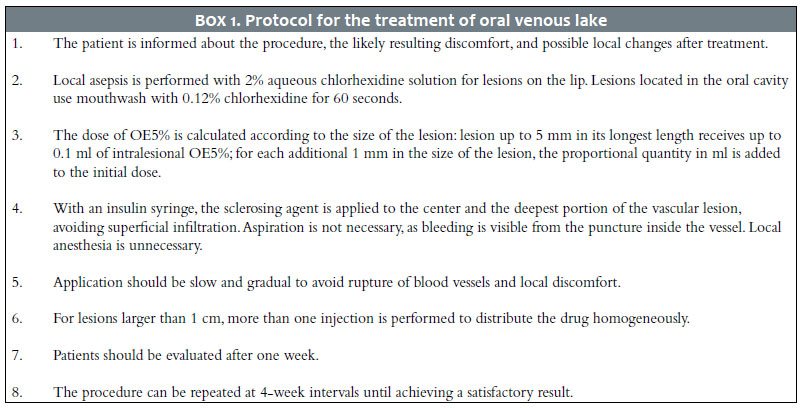
Box 1 describes the treatment protocol for oral venous lake using OE5% with a sclerosing agent (Ethamolin®, Farmoquímica - Brazil). We use the technique in 10 consecutive patients attending the Stomatology Outpatient Clinic of the Department of Dermatology at UNIFESP during 2019 (Box 1).
The procedure is contraindicated in pregnancy, uncontrolled diabetics, and infection at the application site.2-3
Most patients were women (7/10) and over 50 years old (9/10). The venous lake was observed in the lower lip in 6/10 patients, in the upper lip in 1/10 patients, and in the oral mucosa in 3/10 patients. The size varied between 3 mm to 10 mm in diameter. The patients reported asymptomatic lesions with an onset time greater than five years. Some individuals described accidental local trauma with mild bleeding.
Most patients (6/10) needed only one application of OE5% (Figure 1), while other patients required two or three monthly sessions. We observed complete regression of the lesions in the vast majority of cases (9/10), and in one case, the patient was satisfied with only a partial regression.
Most patients reported discomfort after applying the sclerosing agent, such as pain, edema, redness, and burning (Figure 2). These symptoms lasted from one to three days. In one case, ulceration and local necrosis occurred due to the application being more superficial, resolving in seven to ten days without leaving scars (Figure 3).
The diagnosis of the oral venous lake is based on the clinical characteristics and history of the lesion. Vitro pressure, polarized light dermoscopy, aspiration, and imaging exams can also constitute accessory resources for diagnosis and treatment planning in some cases. 3,6,8
Histologically, dilated, thin-walled venules located close to the epithelial tissue can be observed. The differential diagnosis includes melanocytic nevus, melanotic macule, malignant melanoma, pyogenic granuloma, and Kaposi’s sarcoma.2,4,6
The treatment modalities for venous lake include electrocoagulation, surgical excision, laser therapy, infrared coagulation, cryotherapy, and sclerotherapy.5-8 OE5% is one of the most widely used sclerosing agents in treating vascular lesions. The literature describes it as a safe and effective method for injuries located in different body regions.7-10
Our outpatient clinic has used sclerotherapy to treat the oral venous lake for more than ten years with good results. We presented ten patients treated consecutively and who reached a complete resolution in 90% of cases. We suggest this protocol can guide the definition of the drug’s necessary amount regarding the lesion’s size. The application is performed in the outpatient clinic, and it does not require the use of the operating room. The technique is quick and does not require block anesthesia. The most uncomfortable adverse event was the temporary swelling after application, which usually occurs in all cases. It is easily explained considering the inflammatory process caused by the sclerosing agent.
The most observed complication was the ulceration’s appearance due to a very superficial application, which also occurred in some cases throughout our experience. The resolution occurred in 15 days without leaving a scar. The injection technique must be deep in the vascular lesion center to avoid this complication. Using a greater quantity of the sclerosing agent than what is recommended or its overflow may cause ulceration.
The recommended OE5% limit dose for sclerotherapy is up to 2 ml per application. Other complications reported in the literature include hemoglobinuria and hemolytic renal failure cases, but their occurrence was limited to the use of doses greater than 9.6 ml of OE5%.8,10
This protocol’s description aims to share the authors’ experience and the best practices accumulated in the last ten years in a specialized Stomatology service. The protocol can help professionals maximize the chances of success and minimize the appearance of adverse events in the oral venous lake treatment.
The oral venous lake treatment with OE5% is a safe and effective technique that can be used in the dermatologist’s clinical practice.
Dalva Regina Neto Pimentel | 0000-0001-7783-4810
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Rafael Tomaz Gomes | 0000-0001-8775-2173
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Cleonice Hirata | 0000-0002-6336-961X
Study design and planning; data collection, analysis, and interpretation; critical revision of the manuscript.
1. Hyodoh H, Hori M, Akiba H, Tamakawa M, Hyodoh K, Hareyama M. Peripheral vascular malformations: imaging, treatment approaches, and therapeutic issues. Radiographics. 2005;25:S159–S171.
2. Ribeiro MC, de Mattos Camargo Grossmann S, do Amaral MBF, de Castro WH, Navarro TP. Effectiveness and safety of foam sclerotherapy with 5% ethanolamine oleate in the treatment of low-flow venous malformations in the head and neck region: a case series. Int J Oral Maxillofac Surg. 2018;47:900-7.
3. Manzano BR, Premoli AM, Santaella NG, Ikuta CRS, Rubira CMF, Santos PSDS. Sclerotherapy as an esthetic indication in oral vascular malformations: a case series. An Bras Dermatol. 2019;94:521-6.
4. Gomes CC, Gomez RS, do Carmo MA, Castro WH, Gala-García A, Mesquita RA. Mucosal varicosities: case report treated with monoethanolamine oleate. Med Oral Patol Oral Cir Bucal. 2006;11:E44-6.
5. Johann AC, Aguiar MC, do Carmo MA, Gomez RS, Castro WH, Mesquita RA. Sclerotherapy of benign oral vascular lesion with ethanolamine oleate: an open clinical trial with 30 lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100:579-84.
6. Lee JS, Mun JH. Dermoscopy of venous lake on the lips: a comparative study with labial melanotic macule. PLoS One. 2018;13:e0206768.
7. Costa JR, Torriani MA, Hosni ES, D'Avila OP, de Figueiredo PJ. Sclerotherapy for vascular malformations in the oral and maxillofacial region: treatment and follow-up of 66 lesions. J Oral Maxillofac Surg. 2011;69:e88-e92.
8. Fernandes DT, Elias RA, Santos-Silva AR, Vargas PA, Lopes MA. Benign oral vascular lesions treated by sclerotherapy with ethanolamine oleate: a retrospective study of 43 patients. Med Oral Patol Oral Cir Bucal. 2018;23:e180-7.
9. Fernandes DT, Hebling E, Santos-Silva AR, Lopes MA. A series of 33 older patients with lip venous lake treated by sclerotherapy. Int J Dermatol. 2019;59:42-6.
10. Nishikawa M, Sakamoto K, Hidaka M, Yamashita A, Yamamoto G. Venous malformation of the tongue in a child treated by sclerotherapy with ethanolamine oleate: a case report. J Pediatr Surg. 2006;41:599–600.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}