


Luisa Preisler1; Luciana Gasques de Souza2; Marisa Gonzaga da Cunha2
Received on: 10/09/2020
Approved on: 01/12/2020
Financial support: None
Conflict of interest: None
Trabalho realizado em Clínica Privada, São Paulo (SP), Brasil
Acknowledgment: We thank Dr. Ludmilla Cardoso Gomes for reading and reviewing the article
Microinfusion of drugs into the skin (MMP®) is a technique described by Arbache in 2013. It uses a tattoo machine to infuse drugs to treat skin diseases. This study aims to review the literature and list the indications already published on this technique, the medications used in the procedure, and this technique’s safety profile. Despite being widespread among dermatologists, microinfusion of drugs into the skin (MMP®) requires careful analysis, as many indications lack scientific literature. Even though it is a promising technique, it needs further studies to consolidate its indications and assess its safety profile.
Keywords: Infusions, Intralesional; Research and New Techniques; Tattooing
The introduction of active ingredients in the dermis is still an obstacle. Topical medications have variable penetration according to the thickness of the corneal layer. Although intralesional infiltration is an efficient method (as it breaks the skin barrier and delivers the substances directly to the desired location), it has some downsides, such as technology-dependent application (difficulty in microdosing and in standardizing the quantity and depth of application of the active ingredient), challenging treatment of large or very superficial areas, and pain.1
Some authors have proposed methods aimed at solving these adversities. Shelley in the 90s suggested the treatment of warts with the application of bleomycin followed by multiple needle punctures at the site with good therapeutic response.2 España and later Naeini suggested the use of bleomycin followed by needle punctures on keloids and hypertrophic scars,3,4 also with good result. Sadeghinia in 2012 was successful in the treatment of keloids with the application of 5-fluorouracil pre and post-punctures with needle.5
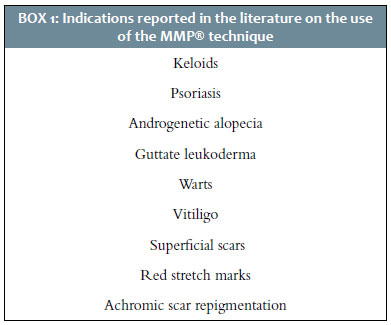
The first case describing the use of the MMP® technique used bleomycin microinfusion in keloid lesions.1 After that, several other reports emerged, such as using the technique to treat androgenetic alopecia,6 leukoderma punctata (guttata),7 and psoriasis,8 among others (Chart 1).
This study aims to review the literature on the already published indications, drugs used, and safety profile of this new treatment modality.
The microinfusion of drugs into the skin (MMP®) is a technique described by Arbache and Godoy in 2013, which uses tattoo equipment to infuse medications into the skin to treat several diseases. Its performance requires the use of tattoo equipment, tips, and needles. There are hundreds of models, one of them with ANVISA certification for medical use. Simple energy sources power them, and many of them have adjustable operating speeds. The needles are available in sealed and sterilized packaging. They are made up of a variable number of solid microneedles of fine diameter, arranged parallel to each other or in a circular shape. The needles’ length is adjustable from 0.1 mm to 2 mm, depending on the epidermis’s thickness and the condition to be treated. When the equipment is turned on, the needles rotate in a “back and forth” motion allowing the medication’s aspiration. The capillarity tangles the drug, and a container above the application tip accumulates it. The distal end of the needles’ design allows the medical practitioner to precisely treat small and rounded areas or large linear areas. When the needles, soaked by the medication, penetrate the skin, the drug is “pushed” into the intercellular medium, tangled by the shearing force. The space between the needles allows healthy skin areas to exist between treated skin sites, favoring re-epithelialization, similar to what occurs in delicate fractionation.1
The percutaneously injected drug has a potent local effect and obtains a therapeutic response, avoiding first-pass hepatic metabolism and reaching the systemic circulation at low undetectable concentration.8
Arbache and Godoy published in 2013 a study for the treatment of keloids comparing MMP® with saline and bleomycin. The first case divided the lesion into three segments: they infused bleomycin on the left, performed no therapy on the center, and introduced saline on the right. The study performed two infusions in 30 days. The second case divided the lesion into two segments: they infused bleomycin on the right, and introduced saline 0.9% on the left, with only one infusion. In both cases, it was possible to observe, visually and on palpation, the improvement in the lesions’ thickness. In the area treated with bleomycin, the reduction was more significant. The treated areas’ biopsies showed microscopical superiority in reducing the keloid thickness in the areas treated with bleomycin compared to those treated with saline.1
Contin in 2016 described two cases of androgenetic alopecia treatment with the MMP® technique. One case infused minoxidil 0.5% (sterile water for injection), and the other performed only micropuncture. The procedures used the Cheyenne® tattoo equipment (Germany Anvisa: 80281110016), with a cartridge with 17 microneedles in a row. The authors adjusted the depth manually at 1.5 mm and completed the procedure with the observation of bloody dew in the entire treated area. The patient who received MMP® combined with minoxidil underwent four monthly sessions, and the patient who received only MMP® underwent three sessions. There was a partial and cosmetically satisfactory response in both cases, without statistical significance.6
Okita et al. described in 2018 four psoriasis treatment cases with MMP® using methotrexate or cyclosporine (two with each medication). The study assessed patients with moderate to severe psoriasis and lesions resistant to other therapies. The results demonstrated good tolerability with no adverse events, and quick and effective response in both treated and distant lesions (those that did not receive the application).8
Arbache et al. in 2018 reported the preliminary analysis of eight patients who completed the randomized clinical trial for the treatment of guttate leukoderma with MMP® and 5-fluorouracil (5-FU). The intervention used the Cheyenne® tattoo equipment. The study treated the lesions on one leg with the MMP® technique combined with placebo (saline) and the other leg with the technique associated with 5-FU. The authors observed repigmentation in the lesions of both legs. However, in the leg treated with 5-FU, the repigmentation was statistically more significant (75.3% of repigmentation in the 5-FU group versus 33.8% in the placebo group, p<0.001). Two patients underwent a biopsy 40 days after the procedure, which demonstrated numerous melanocytes in the area treated with 5-FU.7
Wambier in 2018 also described a series of cases treated with tattoo equipment and disposable needle cartridges, ranging from the use of double-row needles (magnum-27) for large surfaces to a single needle for more accurate treatment. The energy unit was set to 140 Hz, and the needles were kept moist by repeated insertion into the liquid used for each case. This article reported the use of MMP® combined with different medications for the treatment of several pathologies: five cases used 5-FU to treat guttate leukoderma (one session, with evaluation two months later); two cases treated warts with bleomycin (one session, with evaluation two months later); two cases treated vitiligo using triamcinolone acetate (one session, with evaluation two months later); five cases used dutasteride and minoxidil to treat androgenetic alopecia (three monthly sessions, with evaluation after three months); three cases treated superficial scars with 5-FU (one session, evaluation two months later); two cases used hyaluronic acid to treat red stretch marks triggered by a breast prosthesis (three monthly sessions, after three months). All of them presented good response.9
Arbache et al. described in 2019 a case of achromic scar repigmentation resulting from laser tattoo removal using MMP® combined with 5-FU. The study held five sessions, with monthly intervals, achieving complete scar repigmentation and sustained response in the case reassessment after three years.10
One of the main issues regarding the MMP® technique safety is the quantity of the medication that is delivered when using this procedure. Despite differences reported in the literature, a recent study (2019) by Arbache et al. estimated that the mean value is 1,175µg/cm2. This demonstrates the superiority of the technique by allowing the injection of such a small amount of medication in a 1 cm2 surface, in relation to the use of syringes. Regarding the pharmacokinetics of drugs injected into the skin, whether by syringes, tattoo devices, rollers, or fractional CO2 laser, their systemic absorption is undeniable, although there may be differences in the path they take (blood or lymphatic), which depends on the technique, chemical nature, and molecular weight of the drug. A fundamental criterion to be considered when choosing a medication to be used in drug delivery is whether it and its respective vehicle have support for systemic and intradermal application.11
A new drug delivery technique is becoming popular in dermatological practice today: MMP® . In this technique, the needles of the tattoo equipment transfer drugs, instead of ink, into the skin. Thus, microneedling and infusion co-occur. The needle depth is gradually adjusted until a mild bloody dew is obtained, which is an indication that the dermis has been reached.7 This promising technique is suitable for treating various dermatological conditions, overcoming the mechanical corneal barrier that impairs the topical application of the drug (superficial spreading) and the unwanted effects of the drug bolus obtained with intralesional infiltration.9 The literature describes the treatment of pathologies such as leukoderma punctata (guttata), xanthelasma, viral warts, vitiligo, androgenetic alopecia, superficial scars, stretch marks, and psoriasis with results that motivate future studies.8,9
Despite widespread among dermatologists today, microinfusion of drugs into the skin (MMP®) requires careful analysis since some indications routinely performed in practice lack literature with scientific evidence. There are case reports on the treatment of keloids, viral warts, vitiligo, androgenetic alopecia, psoriasis, stretch marks, superficial scars, and achromic scars, as well as the preliminary analysis of a randomized clinical study7 for the treatment of guttate leukoderma with eight patients.
When it comes to the technique safety, there is only one study11 published by Arbache et al. in 2019, which discusses the volume of medication delivered every cm2 by MMP® . However, but there are still no studies that demonstrate and quantify the drug’s safety and systemic pharmacokinetics.
Microinfusion of drugs into the skin (MMP®) is a promising technique, but further studies are needed to consolidate its indications. Few studies have been published so far, and there is no standardization of the drugs to be used, their total dose, and the depth of application. There is still a discussion of what works: whether it is merely the trauma caused by the punctures, the medication’s infusion, or both.
In addition to these questions, considerations about possible contraindications, complications related to the technique and medications, and systemic absorption and elimination of drugs used during the procedure are very relevant.
Luisa Preisler | 0000-0002-1600-9953
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Luciana Gasques de Souza | 0000-0001-5160-7572
Approval of the final version of the manuscript; critical literature review; critical revision of the manuscript.
Marisa Gonzaga da Cunha | 0000-0002-4186-0643
Contribuição no artigo: Concepção e planejamento do estudo.
1. Arbache S, Godoy C. Microinfusão de medicamentos na pele através de máquina de tatuagem. Surg Cosmet Dermatol. 2013;5(1):70-74.
2. Shelley WB, Shelley ED. Intralesional bleomycin sulfate therapy for warts. Arch Dermatol. 1991;127(2):234-6.
3. España A, Solano T, Quintanilla E. Bleomycin in the treatment of keloids and hypertrophic scars by multiple needles punctures. Dermatol Surg. 2001;27(1):23-7.
4. Naeini FF, Najafian J, Ahmadpour K. Bleomycin tattooing as a promising therapeutic modality in large keloids and hypertrophic scars. Dermatol Surg. 2006;32(8):1023-30.
5. Sadeghinia A, Sadeghinia S. Comparison of the efficacy of intralesional triamcinolone acetonide and 5-fluorouracil tattooing of the treatments of keloids. Dermatol Surg. 2012;38(1):104-9.
6. Contin LA. Alopecia androgenética masculina tratada com microagulhamento isolado e associado a minoxidil injetável pela técnica de microinfusão de medicamentos pela pele. Surg Cosmet Dermatol. 2016;8(2):158-61.
7. Arbache S, Roth D, Steiner D, Breunig J, Michalany NS, Arbache ST, et al. Activation of melanocytes in idiophatic guttate hypomelanosis after 5-fluorouracil infusion using a tattoo machine: preliminary analysis of a randomized, split-body, single blinded, placebo controlled clinical trial. J Am Acad Dermatol. 2018;78(1):212-15.
8. Okita AL, Arbache S, Roth DMP, Souza LG, Colferai MMT, Steiner D. Tratamento de psoríase vulgar pela microinfusão de medicamentos na pele (MMP®) usando ciclosporina e metotrexato. Surg Cosmet Dermatol. 2018;10(1):80-4.
9. Wambier C. Dermatologic treatments with microinfusion of drugs into the skin with tattoo equipment: teaser series. J Am Acad Dermatol. 2018;79(3 Suppl 1):AB103.
10. Arbache S, Roth D, Arbache ST, Hirata SH. Original method to repigment achromic laser tattoo removal scars. Case Rep Dermatol. 2019;11(2):140-4.
11. Arbache S, Mattos EDC, Diniz MF, Paiva PYA, Roth D, Arbache ST, et al. How much medication is delivered in a novel drug delivery technique that uses a tattoo machine? Int J Dermatol. 2019;58(6):750-5. Epub 2019 Mar 3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}