


Patrícia Pinheiro Montalvão1; Amanda Soares Teixeira1; Isadora Barreto Michels1; Ingrid Stresser Gioppo1; Anna Carolina Miola1,2
Received on: 30/11/2018 Approved on: 18/08/2020
Financial support: None Conflict of interest: None
Acknowledgment: We would like to thank Dr. Cleverson Teixeira Soares, pathologist at the Lauro de Souza Lima Institute, for providing the PAAF photographic documentation and the anatomopathological examination
Study conducted at the Lauro de Souza Lima Institute, Bauru (SP), Brazil
Nodular fasciitis is a benign tumor resulting from the reactive proliferation of fibroblastic or myofibroblastic cells presenting rapid growth and rich cellularity. In adults, the extremities’ involvement is more frequent; however, other regions can be affected. In this report, we present the case of a 40-year-old woman with a nodular lesion on the forehead. The histopathology confirmed the diagnosis of nodular fasciitis. The reported case highlights its rare location and alerts the clinical dermatologist in its inclusion among the differential diagnoses of tumor lesions on the face.
Keywords: Facial Dermatoses; Fasciitis; Forehead
Nodular fasciitis (FN) is a benign tumor derived from the proliferation of fibroblasts and myofibroblasts that can affect hypodermis, muscle, and fascia. In 1955, Konwaler described the FN as pseudosarcomatous fasciitis or infiltrative fasciitis, because of its strong resemblance to sarcoma. 1 The etiology of the FN is still uncertain, but there are reports of previous trauma in about 10 to 15% of cases.2 Clinically, the lesion presents as a solitary, fast-growing nodule measuring 1 to 5 cm and more frequently affecting the extremities of the upper limbs. Some presentations can be confused with sarcoma due to its rapid growth, rich cellularity, and high mitotic activity, being of fundamental importance the distinction of the FN with malignant neoplastic diseases.
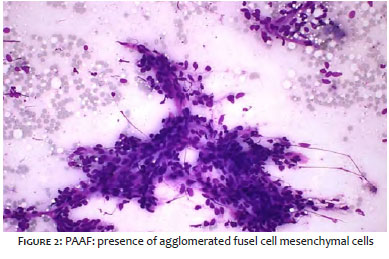
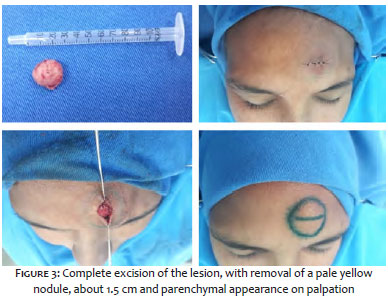
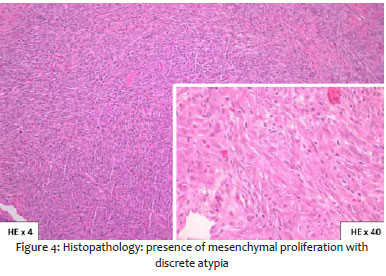
A 40-year-old hypertensive female patient with a history of onset of tumor in the forehead for 4 years, with progressive increase and mild local pain. On physical examination, the tumor of the patient had a 2 cm diameter, mobile, fibroelastic consistency, well-delimited, and not adhered to deep planes on the left forehead (Figure 1). With the diagnostic hypotheses of schwannoma, lipoma, and epidermoid cyst, and due to unavailability of ultrasonography exam (USG), fine needle aspiration (FNA) was performed, which showed fusocellular mesenchymal proliferative lesion suggestive of FN (Figure 2). We chose to perform surgical excision, with the removal of a 2cm-diameter tumor, with a light yellow color, well-delimited and parenchymal consistency (Figure 3). In the histopathological examination, the presence of mesenchymal proliferation with discrete atypias was noted (Figure 4), which, associated with FNAB and clinical presentation, confirmed the diagnosis of FN in the absence of immunohistochemistry.
NF is a benign fibroproliferative disease of unknown etiology that affects men and women between the ages of 20 and 40. Reports of spontaneous remission and frequent location on bony prominences suggest the etiological hypothesis of previous trauma at the site of lesion.2 In adults, the extremity involvement is more frequent in the upper extremities (43%), followed by the trunk (25%) and lower extremities (22%), while only 10% of the FN occurs in the face and neck.3,4 Most cases of NF in the face and neck occur in children.5
Clinically, FN manifests as a tumor lesion, well delimited, about 2 to 5 cm in size, with subcutaneous nodular growth fast and self-limited, and may present painful sensitivity at the site. The main differential diagnoses include pyogenic granuloma, cysts, lipoma, dermatofibroma, neurofibroma, and sarcoma.6,7 Because it is infrequent, it is usually a neglected entity in the evaluation of benign tumor lesions, with other diagnostic hypotheses raised prior to FN. Many cases are usually confirmed by histopathological examination.8
USG can be performed and may show well-defined, hypoechoic, dermal nodular lesions, with or without the presence of a heterogeneous hyperechoic center, and may therefore make a differential diagnosis with malignant nodular lesions. Consequently, anatomopathological examination is necessary in these cases.9
Histopathology demonstrates a well-circumscribed, fascial or intramuscular subcutaneous nodule with a star-like appearance. A proliferation of rounded and fusiform fibroblast and oval nucleus myofibroblasts with thin chromatin and prominent nucleolus is seen. In newly-onset lesions, the cells are loosely arranged in an edematous and myxomatous stroma, while the older lesions show hyalinized collagen bundles.10 Fibroblasts and myofibroblasts react positively to vimentin and specific muscle actin and some cells are CD68 positive.11 The histological differential diagnosis includes fibrosarcoma and malignant fibrous histiocytoma.
The treatment consists of complete surgical excision of the lesion, with a variable recurrence rate according to the literature, probably due to the incomplete excision of the lesion. Other types of treatment may be considered conforming to the location of the lesion, such as CO2 ablative laser and intralesional infiltration with triamcinolone.12
The main objective of this study was to highlight the unusual location of the case and alert the dermatologist for the diagnosis and inclusion of NF as a differential diagnosis of other facial tumors, in order to define the best therapeutic approach of the lesion, avoiding diagnostic errors and possible local recurrences.
Patrícia Pinheiro Montalvão | 0000-0001-6067-0426
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Isadora Barreto Michels | 0000-0002-9393-9724
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical revision of the manuscript.
Amanda Soares Teixeira | 0000-0002-9072-8913
Approval of the final version of the manuscript; critical literature review; critical revision of the manuscript.
Ingrid Stresser Gioppo | 0000-0001-9520-7888
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review.
Anna Carolina Miola | 0000-0001-8926-734X
Approval of the final version of the manuscript; critical literature review; critical revision of the manuscript.
1. Konwaler BE, Keasbey L, Kaplan L. Subcutaneous pseudosarcomatous ¿bromatosis (fasciitis). Am J Clin Pathol. 1955;25(3):241-52.
2. Botton A, Bière A, Galakhoff C. Rôle inducteur du piercing dans une fasciite nodulaire faciale. Presse Med. 2006;35(2 Pt 1):237-8.
3. Shibata Y, Yanaba K, Ito K, Nishimura R, Miyawaki T, Nakagawa H. Nodular fasciitis on the face. J Dermatol. 2016;43(10):1235-6.
4. Gelfand JM, Mirza N, Kantor J. Nodular fasciitis. Arch Dermatol. 2001;137:719-721.
5. Morales DV, Cabrales ES. Nodular fasciitis present in facial area in children. Rev Cuba Estomatol. 2009;46:78-87.
6. Chemmanam JJ. Nodular fasciitis in the tongue- a mimicker of malignancy: case report and review of literature. Indian J Surg Oncol. 2017;8:214-6.
7. Almeida F, Picón M, Pezzi M, Sánchez-Jaúregui E, Carrillo R, Martínez-Lage JL. Nodular fascitis of the maxillofacial region. Two case reports and a review of the literature. Rev Esp Cir Oral y Maxilofac. 2007;29:43-7.
8. Luna A, Molinari L, Bollea Garlatti LA, Ferrario D, Volonteri V, Roitman P, et al. Nodular fasciitis, a forgotten entity. Int J Dermatol. 2019;58(2):190-3.
9. Fujioka K, Fujioka A, Oishi M, Eto H, Tajima S, Nakayama T. Ultrasonography findings of intradermal nodular fasciitis: a rare case report and review of the literature. Clin Experiment Dermatol 2017;42(3):335-6.
10. Weinreb I, Shaw AJ, Perez-Ordoñez B, Goldblum JR, Rubin BP. Nodular fasciitis of the head and neck region: a clinicopathologic description in a series of 30 cases. J Cutan Pathol. 2009;36:1168-73.
11. Souza IS, Vieira BB, Rochael MC, Vieira JST, Farias RE, Schimidt NC. Nodular fasciitis on the zygomatic region: a rare presentation. An Bras Dermatol. 2013;88(6):89-92.
12. Oh BH, Kim J, Zheng Z, Roh MR, Chung KY. Treatment of nodular fasciitis occurring on the face. Ann Dermatol. 2015;27:694-701.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}