


Giovana Larissa Prado Leite Agostinho1; Renan Tironi Giglio de Oliveira1; Ana Paula da Silva Urzedo2; Marisa Gonzaga da Cunha2; Carlos D'Apparecida Santos Machado Filho3
Received on: 30/04/2019
Approved on: 14/07/2019
Study conducted at the Dermatology Service, Faculdade de Medicina do ABC - Santo André (SP), Brazil.
Financial support: Importderm Ltda. (Rio de Janeiro, Brazil) donated the asset Md: complex melanoceuticals® and the company LMG Ltda. (Minas Gerais, Brazil) supplied the Solon® platform and disposable tips free of charge.
Conflict of interest: Importderm Ltda. and LMG Ltda. provided inputs for the research; however, the researchers carried out the methodology, execution, and analysis of the results obtained, without any interference from the.
INTRODUCTION: Melasma is an acquired pathology secondary to hypermelanosis, recurrent, and often refractory to therapy, despite several treatment options. Microneedling is mainly indicated for refractory cases since it is an invasive method with the mechanism of action not yet fully understood for this indication.
OBJECTIVE: To compare the response to melasma treatment between a group that received only microneedling and another treated with microneedling combined with drug delivery.
METHODS: Twenty patients participated in the study: seven received only microneedling and 13 received microneedling followed by drug delivery of lightening serum in three sessions, with monthly intervals. The results between the groups were compared regarding improvement of the Melasma Area and Severity Index (MASI), texture and reduction of skin pore diameter; presence of erythema, crusting and peeling; improvement of melasma extension and tone.
RESULTS: The group that received microneedling combined with drug delivery had the most favorable results in improving texture, decreasing skin pore diameter, and improving melasma extension and tone. MASI improvement occurred in both groups, in similar percentages.
CONCLUSIONS: According to the present study, both therapies are promising for melasma treatment.
Keywords: Comparative study; Therapeutic approachs; Treatment outcome; Evaluation of results of therapeutic interventions
Melasma is an acquired chronic condition secondary to hypermelanosis. It is characterized by brownish macules, with well-defined and irregular borders in photoexposed areas of the skin, such as the malar and frontal regions. It affects both sexes, with a predominance of women of childbearing age. Also, it affects all races, most often Asian and Hispanic, and is more prevalent in intermediate phototypes.1 Studies show that its pathophysiology has involvement with sun exposure, genetic alteration, hormonal and vascular disorders, pregnancy, use of oral and topical cosmetic medications. However, it is known that further research is still needed to elucidate its etiopathogenesis fully.1 Ultraviolet radiation is the main factor in the genesis and maintenance of melasma. It causes lipids peroxidation of basal cell membrane, leading to free radicals release, with consequent stimulation of melanocytes.2 It can be treated only clinically and/or with a combination of cometic procedures.
Due to its relapsing and refractory characteristics, the association is often necessary to obtain a satisfactory response. Topical agents commonly used are hydroquinone-based skin-lightening products, such as the triple formula composed of the combination of this substance with tretinoin and corticosteroids. It is the established therapeutic option, usually indicated early in treatment, associated with intensive photoprotection. Other lightening substances are also effective, such as azelaic, retinoic, ascorbic, tranexamic, and kojic acids, corticosteroids, resorcinol, arbutin, and belides, which act directly and indirectly in the melanogenesis stages. Regarding the procedure options, we can mention chemical and physical peels and laser applications (QSwitched, Nd:YAG 1064, CO2, Erbium YAG 2940), intense pulsed light, and microneedling.3
Microneedling consists of multiple perforations of the epidermis and dermis with the aid of microneedle devices. Its use is established for the treatment of skin laxity, as it stimulates neocollagenesis by activating fibroblasts. However, recently, this technique has also been attributed to a whitening action. It is usually indicated in recalcitrant cases of melasma, although its mechanism of action in this condition is not yet fully understood. Nonetheless, studies show that its use alone or in combination with drug delivery of lightening substances has shown satisfactory results.4 As microneedling has lately been introduced in medical practice, there is a scarcity of scientific work on the subject, mainly in the scope of assessing its effectiveness as a lightening method. Thus, this study aimed to compare the response of melasma treatment between the group that received microneedling alone and the group that received the same procedure associated with drug delivery with serum composed mainly of lightening substances.
A randomized clinical trial was conducted with patients from the Dermatology Outpatient Clinic of the Faculdade de Medicina do ABC, after approval by the Research Ethics Committee of this institution (CAAE: 93551518.7.0000.0082). For initial selection of participants, we considered the following inclusion criteria: characteristic clinical presentation of facial melasma; men and women aged over 18 years old; be without the following melasma-specific treatments for at least six months: topical use of hydroquinone-based skin-lightening products and their derivatives, performing procedures such as chemical peels, lasers (QSwitched, Nd:YAG 1064, CO2, Erbium YAG 2940) and intense pulsed light. The exclusion criteria adopted were: ongoing pregnancy; hypersensitivity to any component of the applied lightening formula; presence of facial scars or active facial dermatoses at the time the microneedling sessions were performed. The patients signed the informed consent form, which detailed the risks, and consequences of the procedures, such as pain, skin infection, blister formation, facial erythema and paradoxical worsening of the pigmentation. They also signed a document authorizing to make photographic records throughout the study.
Participants were randomly divided into groups A and B. Group A received microneedling on the entire face with a 7x7mm gold-plated microneedle device, of the Solon® (LMG - Laser Medical Group Ltda; Guaxupé, MG - Brazil) platform, with the following programming: radiofrequency: zero W, pulse duration: 80ms, needle depth: 1.5mm. The needle tips were discarded at each session. Three sessions were held, with an interval of 30 days between them. One hour before each procedure, a topical local anesthetic (lidocaine and tetracaine Cream 7%/7%) was applied to the entire face. Group B received microneedling identical to group A, both regarding the device used and its programming, and the number of sessions, interval between them, and time of topical anesthetic use of before the procedure. However, in group B participants, the whole-face drug delivery method was associated immediately after the microneedling, consisting of the topical application of 0.8 ml of industrialized lightening product Md: complex melanoceuticals®, which combines kojic acid, tranexamic acid, azeloglycine, arbutin, glycolic acid, ascorbic acid, citric acid, and glutathione in undisclosed concentrations (Md: ceuticals, imported by Importderm Ltda; Rio de Janeiro, RJ - Brazil). The patients were instructed to apply a high sun protector factor sunscreen (SPF 60) daily, starting 24 hours after the procedure, and to avoid sun exposure throughout the entire treatment period.
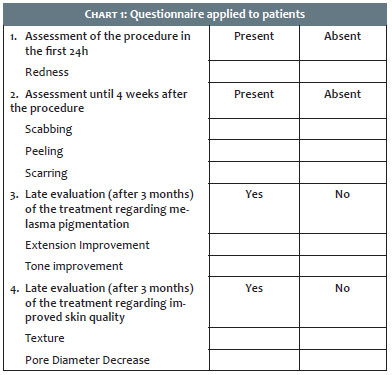
The results were obtained by a pooled analysis of the data from the self-assessment questionnaire (Chart 1) designed by the project organizers and applied to the patients after three months of the last session of the procedure. In addition to these evaluations, the Melasma Area and Severity Index (MASI) was calculated for each patient before the procedures and three months after the end of treatment. This score was conducted by three dermatologist examiners using the photographic analyzes of the patients. All photographic records were standardized, performed by a skilled technician with a professional camera, and under conventional light. The information collected from all questionnaires were compared between groups A and B. For statistical analysis, the chi-square test, Stata 11.0 program, with a significance level of 5% was used.
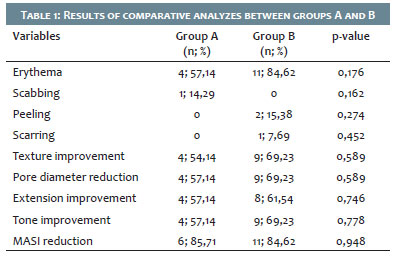
Of the 55 patients selected, 35 were lost to follow-up. Therefore, the total number of participants who completed the study was 20. Group A (microneedling alone) consisted of seven patients and group B (microneedling with drug-delivery) of 13 patients. Table 1 describes the comparative analyzes. Of the participants in group A, only one mentioned scabbing, none reported scaling or scarring, and there were fewer cases of rash after the procedure regarding the other group. Group B reported the highest number of improved melasma extension and tone, decreased pore diameter - open channels during microneedling - and improved skin texture, and no mention of scabbing. Only one patient reported facial scarring with the treatment. Regarding the comparative evaluation of MASI, there was a reduction in the score for both groups in a similar percentage, with a slight advantage for the one that received microneedling alone. The analyses showed no statistically significant differences between the two groups.
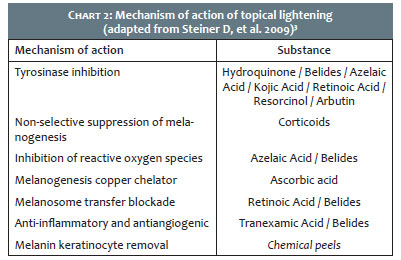
Melasma is a chronic condition, often resistant to treatment and stigmatizing. Despite the various therapeutic options, it is still a challenge to fully control the condition and maintain it in remission for long periods. Regarding the topical treatment modalities, there are several lightening substances, as shown in Chart 2. The combined use of these substances is known to increase the chance of treatment success.3,5D Different cometic procedures can assist in therapy, such as peelings, dermabrasion, lasers, intense pulsed light, and mesotherapy. Microneedling has been reported as a promising technique for recalcitrant melasma, but its mechanism of action as a lightener is not yet fully elucidated.6,7 Frabbocini et al.5 conducted a study with 20 patients with melasma, in which all participants received microneedling followed by drug delivery with lightening serum (rucinol and Sophora-alpha) in one hemiface, while in the other hemiface only the serum was applied. Two sessions were performed, with monthly intervals between them. In the hemifaces that received microneedling followed by drug delivery, there was a mean reduction in MASI from 19.1 to 9.2, while in hemifaces receiving only the topical lightening serum, the mean reduction in MASI was from 20.4 to 13.3. Budamaklunda et al.6 performed a comparative study with patients diagnosed with facial melasma, divided into two groups with 30 participants in each. One group received treatment with mesotherapy with tranexamic acid, and the other received microneedling with drug delivery of tranexamic acid. There were three monthly sessions. In the mesotherapy group, there was an improvement of 35.72% in the MASI compared to an improvement of 44.41% in the microneedling group associated with drug delivery. Lima8 conducted a study of 22 patients with recalcitrant melasma: all of them underwent a microneedling session and were instructed to use the Kligman formula (retinoic acid 0.05% + hydroquinone 4% + fluocinolone acetonide 1%) every night, for one month, associated with sunscreen SPF 60 with color during the day. The author reported improvement of MASI in all patients and a 24-month follow-up without melasma worsening in half of the group. Saraiva et al.9 selected 17 women to treat the melasma with robotic microneedling associated with drug delivery of tranexamic acid. There were four biweekly sessions. Regarding MASI, there was a mean reduction from 21.33% to 11.19%.
In the present study, the reduction in MASI occurred at a high and practically similar percentage between the two groups. There was a more significant benefit from the association with drug delivery concerning the absence of scabbing, improved texture, and decreased skin pore diameter, extension and tone of melasma. In contrast, there were more cases of peeling and erythema after the procedure, probably due to the presence of the acids of the lightening serum formula. Although these study results are promising, it has some limitations, such as the withdrawal of part of the patients for unclear reasons and the fact that it was performed in the summer in a tropical country (higher rate of ultraviolet radiation). One should also question the concentration of compounds present in the drug delivery product, which is not disclosed by the manufacturer. However, the findings of this study are similar to those of the literature cited, showing that microneedling, associated or not with the drug delivery, promotes melasma lightening. There is a need for a better understanding of the pathophysiology of this disease and prospective randomized studies comparing the efficacy of conventional therapies regarding the currently promising ones.
There was no statistical difference in MASI improvement between the group receiving melasma treatment with microneedling alone compared to the group that performed the same procedure associated with drug delivery. Therefore, according to the present study, both therapies are promising for the treatment of this condition.
We thank Dr. Daphine Tironi Giglio de Oliveira for the support and encouragement of this study.
Giovana Larissa Prado Leite Agostinho | 0000-0002-9973-4930
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Renan Tironi Giglio de Oliveira | 0000-001-5013-7660
Data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Ana Paula da Silva Urzedo | 0000-0002-7322-3278
Study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marisa Gonzaga da Cunha | 0000-0002-4186-0643
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases;critical revision of the manuscript.
Carlos D'Apparecida Santos Machado Filho | 0000-0003-4362-1563
Approval of the final version of the manuscript; critical revision of the manuscript.
1. Miot LDB, Miot HA, Silva MG, Marques MEA. Physiopathology of melasma. An Bras Dermatol. 2009; 84(6):623-35.
2. Handel AC. Fatores de risco para melasma em mulheres: um estudo caso- controle (Dissertação). Faculdade de Medicina de Botucatu - Universidade Estadual Paulista (UNESP); 2013.
3. Steiner D, Feola C, Bialesk N, Silva FAM. Treatment of Melasma: systematic review. Surg Cosmet Dermatol. 2009; 1(2):87-94.
4. Kalil C, Campos V, Reinehr CPH, Chaves CRP. Microneedling: a case series associated with drug delivery. Surg Cosmet Dermatol. 2017; 9(1): 96-9. 5.
5. Fabbrocini G, De Vita V, Fardella N, Pastore F, Annunziata MC, Mauriello MC, et al. Skin needling to enhance depigmenting serum penetration in the treatment of melasma. Plast Surg Int. 2011; 2011:158241.
6. Budamakuntla L, Loganthan E, Suresh DH, Shanmugams S, Suryanarayan S, Dongare A, et al. A randomised, open-label, comparative study of tranexamic acid microinjections and tranexamic acid with microneedling in patients with melasma. J Cutan Aesthet Surg. 2013; 6(3): 139-43.
7. Lima EVA, Lima MMDA, Paixão MP, Miot HA. Assessment of the effects of skin microneedling as adjuvant therapy for facial melasma: a pilot study. BMC Dermatol. 2017.17 (1):14.
8. Lima EA. Microneedling in facial recalcitrant melasma: report of a series of 22 cases. An Bras Dermatol. 2015; 90(6): 919-21.
9. Saraiva LPPG, Nascimento MB, Filippo AA, Gusmão PR. Treatment of facial melasma with robotic microneedling associated to drug delivery of tranexamic acid. Surg Cosmet Dermatol. 2018; 10(4):333-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}