


Mariana Sousa Batista1; Luís Galante Santiago1; André Castro Pinho2; Ana Maria Carvalho Brinca2; Ricardo José David Costa Vieira2
Received on: 12/05/2019
Approved on: 06/06/2019
This study was performed at the Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal.
Financial support: None
Conflict of interests: None
The reconstruction of defects involving up to 2/3 of the lip extension is challenging, considering the functional and aesthetic importance of this structure. There are several surgical techniques described for this purpose, highlighting the Abbé-Estlander flap, the Karapandzic flap, and the Bernard-Burrow- Webster flap. The choice of the best approach should consider the size and location of the defect as well as the comorbidities of the patient. The reverse Yu flap is an alternative to be considered in relation to other methods, allowing obtaining excellent cosmetic-functional results in general.
Keywords: Surgical flaps; Reconstruction; Lip
Considering the functional and aesthetic importance of the lips, many techniques have been described for the reconstruction of surgical defects in this region. The most relevant factors for the choice of the reconstructive approach are the labial defect's size and location, taking into consideration the limitations imposed by the patient's general state and comorbidities.
Yu et al. described an innovative flap in 19891 aimed at reconstructing surgical defects in the lower lip. This flap can also be used in a reverse way for reconstructing defects in the upper lip.
The Yu's flap is in fact the result of the combination of three local flaps:
a) a first sliding rhomboid flap that advances towards the labial defect, starting from the buccinator muscle area (its base located superiorly when the defect is in the upper lip, and vice-versa);
b) a second sliding rotation flap, roughly triangular in shape, used to cover the first flap donor area;
c) a jugal mucosa flap aimed at reconstructing the vermilion of the lip.
The surgical strategy can be summarized as follows2 (Figures 1-3):
1. Curvilinear incision carried out along the nasolabial sulcus, extending by 1cm below the commissure.
2. Horizontal incision from the labial commissure up until to the previously performed labial incision. The length of this incision should be identical to that of the surgical defect's width when the Yu's flap is performed unilaterally. When performed bilaterally, the length of the incision should be half of the defect's width.
3. The first flap is raised in the subcutaneous plane observing the limits of the previous incisions, and advanced to the midline so as to cover the surgical defect. The second flap is subsequently dissected in a way that the skin and subcutaneous tissue of the nasolabial region rotates and advances to reconstruct the remaining defect of the first flap's donor zone. A discharge incision is carried out perpendicularly to the nasolabial groove in order to allow the rotation of the flap.
4. A third flap prepared from the jugal mucosa and roughly triangular in shape is raised in a submucosal plane aimed at reconstructing the vermilion of the lip.
The Yu's flap is a good option when the surgical defect covers more than 1/3 of the lip's length. Thus, when applied unilaterally, it can cover defects of up to 2/3 of the lip's extension. If performed bilaterally, it is able to repair defects covering 2/3 of the lip's length or even subtotal defects. 2, 3
The authors of the present study applied this technique in the reconstruction of three extensive labial defects, all of which originated from radical excisions of squamous cell carcinomas.
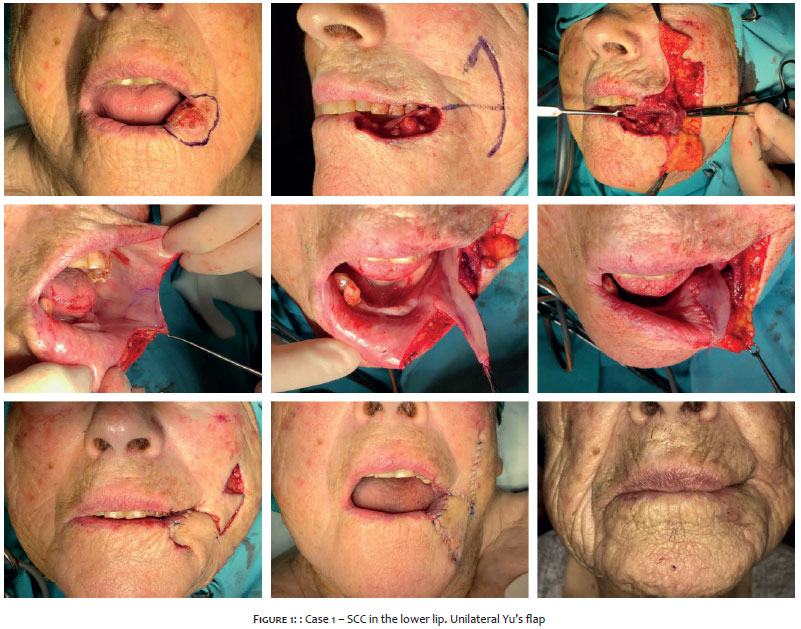
Case 1: A 90-year-old woman bore a tumor with 2cm and erosive-crusted surface, located at the lower left 1/3 of the lower lip, that had emerged seven months before. Tumor resection resulted in a surgical defect covering more than 1/3 of the lip's extension. A left unilateral Yu's flap was implemented under left infraorbital and mental nerve block (Figure 1).
Case 2: A 82-year-old man bore a squamous cell carcinoma measuring 3cm on the longest axis, covering the middle third of the upper lip. Radical excision of the tumor led to a total thickness defect of the lip that reached almost half of its extension (Figure 2). An inverted unilateral Yu's flap was performed under bilateral infraorbital nerve block.
Case 3: An 88-year-old male patient bore a recurrent squamous cell carcinoma measuring roughly 3cm on the longest axis that covered the left inferior 2/3 of the lower lip. Its excision led to a total thickness defect covering between 1/2 and 2/3 of the lower lip's extension (Figure 3). Under general anesthesia, the patient underwent a bilateral Yu's flap.
There were no complications in any of the cases. The cosmetic-functional outcome was considered favorable in all cases, with preservation of oral continence and absence of microstomy.
The Yu's method is advantageous for allowing functional preservation of the lip by keeping the direction of the orbicularis muscle's fibers and preserving the oral continence. It preserves the location and shape of the labial commissure, maintaining asymmetry with the opposite side, even when performed unilaterally. This particularity is key for achieving a good aesthetic outcome. Owing to the fact it does not cause limitations for feeding and speech, it is a surgical procedure that allows a rapid return to normal life.
When compared to other flaps used for the same purpose – namely Karapandzic's4, 5, Bernard-Burrow-Webster's 6, 7 and Abbe-Estlander's 8 – the Yu's flap has advantages and rewarding cosmetic outcomes.
The Karapandzic's flap is associated with higher microstomy rates with risk of distortion of the labial commissures.9, 10 Despite not leading to microstomy, the Bernard-Burrow-Webster's flap usually results in some degree of incontinence of the oral sphincter, particularly at the commissures, and may also lead to a retraction of the lip relative to the expected position.10, 11 The main disadvantage of the Abbe-Estlander's flap is the need for two surgical times, in special when the surgical defect does not involve the commissure as well as risk of microstomy. 12
It is important to note that, when used for reconstruction of subtotal and total defects, the Yu's flap may also cause microstomy. 13 Despite its greater surgical complexity, this flap carries a very low risk of injury to important structures. Nevertheless, it is necessary to preserve the fibers of the orbicularis oris muscle due to the risk of impairing oral continence in case it is destroyed.
By preserving the oral competence and symmetrical opening of the mouth, the Yu's flap guarantees good aesthetic outcomes in a single surgical time. If and when implemented, it implies a short hospital stay with a rapid return of the patient to his or her activities and daily routine.
The Yu’s flap is an excellent alternative for the reconstruction of extensive defects of the lip, with a cosmetic-functional outcome that can be deemed advantageous over other procedures described for the same purpose.
Mariana Sousa Batista | ORCID 0000-0003-3442-615X
Preparation and drafting of the manuscript; critical review of the literature.
Luís Galante Santiago | ORCID 0000-0003-2587-5535
Data collection, analysis and interpretation.
André Castro Pinho | ORCID 0000-0001-6433-311X
Critical review of the manuscript.
Ana Maria Carvalho Brinca | ORCID 0000-0002-7539-9912
Critical review of the manuscript.
Ricardo José David Costa Vieira | ORCID 0000-0002-5914-9171
Approval of the final version of the manuscript; critical review of the manuscript.
1. JM Y. A New Method for Reconstruction of the Lower Lip After Tumor Resection Eur J Plast Surg 1989;12:155-9.
2. Casanas Villalba N, Redondo Gonzalez LM, Peral Cagigal B, Perez Villar A. Yu's Technique: An Optimal Local Flap for Lower Lip Reconstruction. J Oral Maxillofac Surg. 2017;75(1):207-213.
3. Li ZN, Li RW, Tan XX, Xu ZF, Liu FY, Duan WY, et al. Yu's flap for lower lip and reverse Yu's flap for upper lip reconstruction: 20 years experience. Br J Oral Maxillofac Surg. 2013;51(8):767-72.
4. Karapandzic M. Reconstruction of lip defects by local arterial flaps. Br J Plast Surg. 1974;27(1):93-7. 7.
5. Ethunandan M, Macpherson DW, Santhanam V. Karapandzic flap for reconstruction of lip defects. J Oral Maxillofac Surg. 2007 Dec;65(12):2512-7.
6. Williams EF, 3rd, Setzen G, Mulvaney MJ. Modified Bernard-Burow cheek advancement and cross-lip flap for total lip reconstruction. Arch Otolaryngol Head Neck Surg. 1996;122(11):1253-8.
7. C B. Cancer de la levre inferieure: restauratio a l'aide de lembeaux quadrilataires-lateraux querison. . Scalpel. 1852;5:162-4.
8. Kumar A, Shetty PM, Bhambar RS, Gattumeedhi SR, Kumar RM, Kumar H. Versatility of abbe-estlander flap in lip reconstruction - a prospective clinical study. J Clin Diagn Res. 2014;8(10):NC18-21.
9. Closmann JJ, Pogrel MA, Schmidt BL. Reconstruction of perioral defects following resection for oral squamous cell carcinoma. J Oral Maxillofac Surg. 2006;64(3):367-74.
10. Brinca A, Andrade P, Vieira R, Figueiredo A. Karapandzic flap and Bernard-Burrow-Webster flap for reconstruction of the lower lip. An Bras Dermatol. 2011;86(4 Suppl 1):S156-9
11. Konstantinovic VS. Refinement of the Fries and Webster modifications of the Bernard repair of the lower lip. Br J Plast Surg. 1996;49(7):462-5.
12. Krunic AL, Weitzul S, Taylor RS. Advanced reconstructive techniques for the lip and perioral area. Dermatol Clin. 2005;23(1):43-53, v-vi.
13. Bai S, Li RW, Xu ZF, Duan WY, Liu FY, Sun CF. Total and near-total lower lip reconstruction: 20 years experience. J Craniomaxillofac Surg. 2015;43(3):367-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}