


Ana Carolina Krum dos Santos1; Renan Rangel Bonamigo1,2; Fernanda Poy Dondonis1; André da Silva Cartell3,4; Fernando Procianoy5,6
Received on: 21/09/2018
Approved on: 05/04/2019
This study was performed at the Departments of Dermatology and Ophthalmology, Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul, Porto Alegre (RS), Brazil.
Financial support: None
Conflict of interests: None
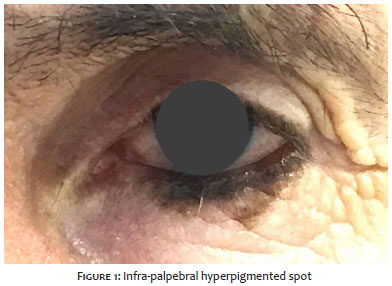
A 74-year-old male patient came to medical consultation presenting a hyperpigmented stain near the lower left eyelid edge, with varying colors, between different shades of brown; the biopsy confirmed the diagnosis of lentigo maligna. Its location on the eyelid edge is rare. There is some divergence in the literature regarding the best method for its treatment. Non-surgical therapeutic options, such as imiquimod, have been suggested, as well as different variants in surgical management and required margins. In the case described, it was chosen to manage with conservative margins, preserving, the functionality of the area.
Keywords: Lentigo; Melanoma; Eyelid Neoplasms; Dermoscopy; Pathology, Surgical; Surgery, Plastic
The lentigo maligna melanoma, an in situ lesion commonly found on the face and cervical region, may compromise sites where treatment is challenging, such as the palpebral region. Lentigo maligna in this location is rare, with rates less than 1% among melanomas and accounting for up to 1% of all palpebral malignancies.1,2 Lesions with conjunctival involvement characteristically have more aggressive behavior. The prognosis is generally good, however recurrences are frequent, depending on the treatment used. Considering its relative low aggressiveness and delicate topography, this type of melanoma's management persists as debatable. Many authors advocate the use of non-surgical therapies, even though potentially superior recurrence rates are considered.1,2 The authors of the present study describe the case of a patient whose lesion was located along the lower eyelid border, with excellent oncological, functional and aesthetic outcomes after surgical treatment.
A 74-year-old male patient attended a medical consultation complaining of a darkened lesion on the left lower ciliary border two years before, with progressive growth. He had previously been seen by an ophthalmologist due to bilateral entropion, with prescription of artificial tears eye drops and extraction of eyelashes, having been referred to the dermatologic evaluation of the pigmented lesion. The patient had previous history of excision of lesions in the face and left forearm ten years before, with clinical impression of skin cancer, without histological confirmation. The patient had previous diagnoses of systemic arterial hypertension, dyslipidemia and insomnia. He made continuous use of captopril, omeprazole and clonazepam. Also, he had previously undergone herniated disc surgery. He denied current or previous drug allergies, smoking habits, and alcoholism. He reported a history of ocular cancer in a first-degree cousin and denied a positive family history for skin cancer.
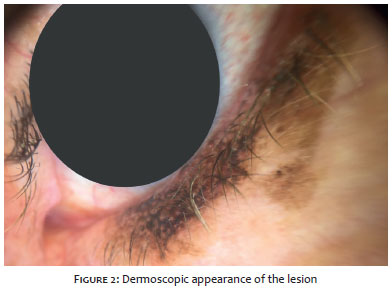
The clinical examination of the patient evidenced a hyperpigmented asymmetric macula, with various shades of brownish color, ranging from light to dark, with irregular borders, accompanying the left inferior palpebral rhyme (Figure 1). Dermoscopic examination revealed a thick pigmented network with eccentric pigmentation area in "blur" invading the follicular openings, as well as the presence of globules at the periphery of the lesion (Figure 2). The dermoscopic impression was of a cutaneous melanoma.
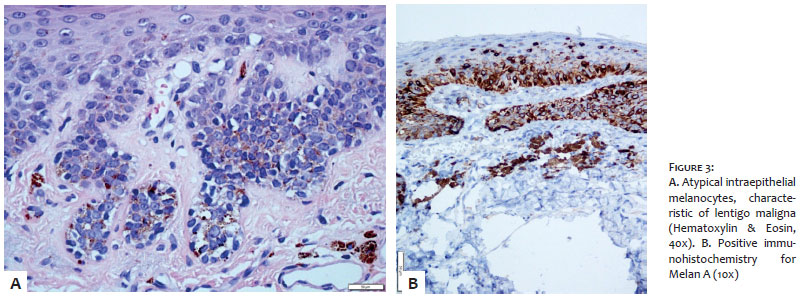
The patient was referred to the Oculoplastics department of the Ophthalmology Service for diagnostic surgical intervention. Since there was presence of trichiasis in the central region of the lower left eyelid, a total thickness resection of the central region of the left lower eyelid, in the shape of a pentagon, was carried out aiming at removing the area of poorly positioned eyelashes and obtaining material for histological analysis of the lesion. In the face of the anatomopathological diagnosis of lentigo maligna (Figure 3A), which was corroborated by the positive immunohistochemistry for Melan A (Figure 3B) and HMB-45, the safety margin was widened to 5mm, which corresponded to the total resection of the left lower eyelid. The reconstruction of the lower eyelid was performed with a Mustardé rotation flap. Considering aspects of the surgical treatment of the neoplasia, the ocular apparatus' functionality, and facial aesthetics, the therapeutic outcome was outstanding (Figure 4).
Unlike in other body regions, margin expansion in periocular melanocytic lesions is challenging, since small amounts of resected tissue can lead to significant functional and aesthetic impairment. Often, it is necessary to limit the expansion of the margin to what is considered surgically acceptable in terms of resection and reconstruction. In the present case, a total thickness eyelid resection was chosen due to the involvement of the palpebral skin up until the mucocutaneous junction, even if there was no involvement of the palpebral conjunctiva.
Interestingly, there is no consensus as to the necessity and/or extent of expansion of safety margins in the conjunctival face when there is no compromise beyond mucocutaneous junction. Although surgical resection is the gold standard method, non-surgical options, such as the use of imiquimod, have been introduced with interesting outcomes in the treatment of in situ lesions of the periocular region.3, 5
However, following the principle of oncologic surgical treatment for the management of primary cutaneous melanomas seems to grant primordial safety, with unprecedented cure rates. The observation of oncological principles must be associated to the concern about the functionality and aesthetics resulting from the intervention.4
For obtaining the best results from complex situations, specialized teams are crucial and should join forces in productive interaction.
The Authors of the present study would like to thank the Dermatology Service team of the Hospital de Clínicas de Porto Alegre, (RS), Brazil.
Ana Carolina Krum dos Santos | ORCID 0000-0001-9863-1836
Approval of the final version of the manuscript; study design and planning; manuscript preparation and drafting; data collection, analysis and interpretation; intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied; critical review of the literature; critical review of the manuscript.
Renan Rangel Bonamigo | ORCID 0000-0003-4792-8466
Approval of the final version of the manuscript; study design and planning; manuscript preparation and drafting; data collection, analysis and interpretation; research guidance; intellectual participation in the therapeutic and / or therapeutic approach of the the cases studied; critical review of the literature; critical review of the manuscript.
Fernanda Poy Dondonis | ORCID 0000-0002-8307-2098
Approval of the final version of the manuscript; study design and planning; intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied; critical review of the manuscript.
André da Silva Cartell | ORCID 0000-0003-1436-9418
Approval of the final version of the manuscript; data collection, analysis and interpretation; intellectual participation in therapeutic and / or therapeutic approach of the cases studied.
Fernando Procianoy | ORCID 0000-0003-3365-8813
Approval of the final version of the manuscript; manuscript preparation and drafting; intellectual participation in propaedeutic and / or therapeutic approach of the cases studied; critical review of the literature; critical review of the manuscript.
1. Vaziri M, Buffam FV, Martinka, M, Oryschak A, Dhaliwal H, White VA. Clinicopathologic Features and Behavior of Cutaneous Eyelid Melanoma. Ophthalmology. 1991;98(12):1867-73.
2. Chan FM, O'Donnell BA, Whitehead K, Ryman W, Sullivan TJ. Treatment and Outcomes of Malignant Melanoma of the Eyelid; A Review of 29 Cases in Australia. Ophthalmology. 2007;114(1):187-92.
3. Elia MD, Lally SE, Hanlon AM, Choi JN,Servat JJ, Shields JA et al. Periocular Melanoma In Situ Treated With Imiquimod. Ophthal Plast Reconstr Surg. 2016;32(5):371-3.
4. Piazza CD, Sampaio SAP. Remission of extensive lentigo maligna after treatment with imiquimod*. An Bras Dermatol. 2009;84(1):82-4.
5. Mutlu OO, Egemen O, Dilber A, Üsçetin I. Aesthetic Unit-Based Reconstruction of Periorbital Defects. J Craniofac Surg. 2016;27(2):429-32.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}