


John Verrinder Veasey1; Barbara Arruda Fraletti Miguel1; Adriana Bittencourt Campaner2; Thiago da Silveira Manzione3
Received on: 22/08/2018
Approved on: 08/12/2018
This study was performed at Hospital da Santa Casa de São Paulo – São Paulo (SP), Brasil.
Financial support: None.
Conflict of interests: None.
INTRODUCTION: Extramammary Paget disease consists of a cutaneous adenocarcinoma in areas of apocrine glands. It is a rare neoplasia, and its surgical treatment yields satisfactory results. However, due to the high recurrence rates, surgeries are potentially disfiguring. Imiquimod is a topical immune-stimulant used for the treatment of anogenital warts and in situ carcinomas. Its use has been described in the scientific literature for the treatment of Extramammary Paget disease with satisfactory results.
OBJECTIVE: Describe the course of four cases of Extramammary Paget disease treated with imiquimod, to evaluate evolution and therapeutic response.
METHODS: A retrospective study was performed in a service of dermatology in the city of São Paulo, with the review of medical records of all patients diagnosed with Extramammary Paget disease and treated with imiquimod from January 2011 to July 2018.
RESULTS: Four patients were included, three with vulvar lesion and one with scrotal lesion. Two women presented completed resolution of the disease, one did not respond and the man progressed with 70% regression of the lesion, having undergone surgical excision of a considerably smaller area than the initial lesion.
CONCLUSIONS: Imiquimod presents as a valid therapeutic modality for the treatment of Extramammary Paget disease.
Keywords: Paget disease, extramammary; Neoadjuvant therapy; Gynecology; Urogenital neoplasms, female; Genital neoplasms, male; Neoplasm recurrence, local; Skin neoplasms; Therapeutics; Vulvar neoplasms;
Extramammary Paget disease (EMPD) is represented by cutaneous adenocarcinoma with similar histology to mammary Paget disease. It affects the skin regions with apocrine glands, more frequently the vulva, followed by the perianal area, scrotum and axilla. It is classified into primary, when it affects the skin only, and secondary, when there is an underlying or distant carcinoma.1
Its clinical aspect can be similar to other diseases such as tineas, contact dermatitis, seborrheic dermatitis, psoriasis and Bowen's disease, making the clinical diagnosis difficult. Diagnostic confirmation is through histopathology, and lately, reflectance confocal microscopy has also been used as an in vivo diagnostic tool.2 After confirmation of the diagnosis, it is crucial to define if EMPD is exclusively cutaneous (primary) or if there is an underlying disease (secondary) by looking for malignancy in pelvic and intra-abdominal organs, such as gallbladder, liver and colon, and breasts.1
Treatment is challenging for many reasons. The centrifugal growth of the tumor with subclinical lesions in the periphery is one of them, which can conceal the right area to be treated. The diagnostic delay due to the similarity to other skin conditions allows for the progressive growth of the disease, and the location of the neoplasia in areas that are difficult to reach.3 Many treatments are described for EMPD: surgical excision, radiotherapy,4 photodynamic therapy and topical treatments,5 and out of those, Mohs micrographic surgery provides the best results. However, the recurrence rate is around 30%, which can lead to mutilanting surgical outcomes.6
Imiquimod (IQM) is a substance that activates the epithelial immune response where it is applied. During this process, IQM induces keratinocytes to release cytokines that trigger the innate response of the epithelium at the same time that it stimulates the migration of Langerhans cells, that in turn start the process of acquired response when identifying the foreign agent to be attacked. In face of this combined immunobiologic stimulation, IQM demonstrates antiviral and antitumor activity.7 Recent studies have demonstrated good therapeutic response of EMPD to IQM.
In this study, we present the experience of the dermatology clinic of the only public service of the city of São Paulo on the use of IQM as monotherapy for EMPD.
A retrospective study with files from all patients seen at the dermatology clinic of Santa Casa de São Paulo, SP, Brazil, who were diagnosed with EMPD and treated with IQM from January 2011 to July 2018 was conducted.
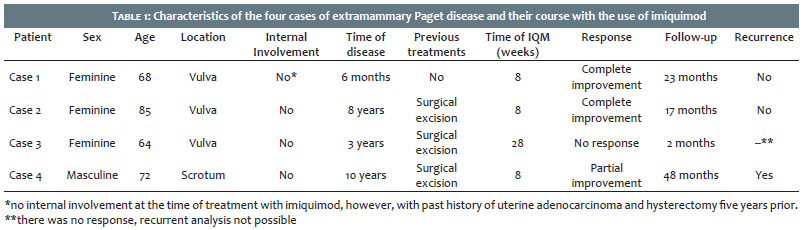
The characteristics analyzed from each case were: clinical profile of the patient (sex, age, comorbidities), location of the lesion, time of disease before treatment with IQM, previous treatments, time of treatment with IQM, treatment response (total, partial or lack of improvement) and time of follow-up after treatment for analysis of recurrence.
Four patients were included in this study: three women with vulvar lesions and one man with lesion on the scrotum. They were investigated regarding the presence of concurrent malignancies, however, there were no abnormalities. The details for each case are presented on table 1. All patients had their diagnosis of EMPD by skin biopsy and histopathology, and screening for systemic involvement through imaging studies: mammogram, abdominal and pelvic tomography. In all cases, IQM application was done on five consecutive days at night, with two days rest on the weekend without using the product.
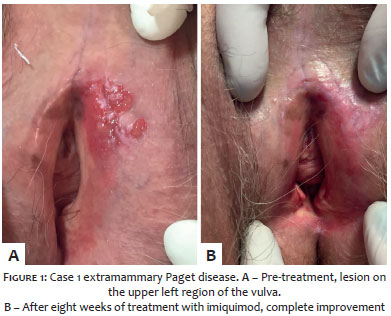
Patient 1, 68 years old and history of systemic hypertension (HTN) and diabetes mellitus (DM), underwent hysterectomy in 2011 due to endometrial adenocarcinoma and was diagnosed with EMPD in 2016. She had a progressively growing vulvar lesion for six months, with no previous treatment. At the time of the EMPD diagnosis, she had no systemic involvement of the disease, so IQM was prescribed for eight weeks, with complete response and no recurrence after 23 months of follow-up (Figure 1).
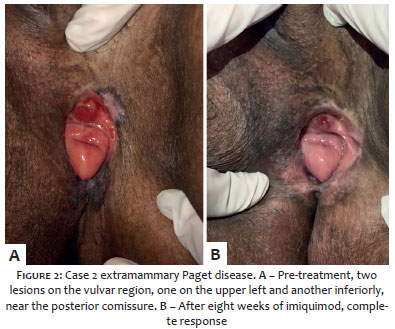
Patient 2, 85 years old, had history of HTN, following-up vulvar EMPD since 2009, with no systemic involvement of the disease. She underwent five surgical interventions between 2009 and 2016, all of them with recurrence of the lesion. After this period, she started treatment with IQM, finishing eight weeks of application. She progressed with complete improvement of the lesion, with no recurrence 17 months after finishing the treatment (Figure 2).
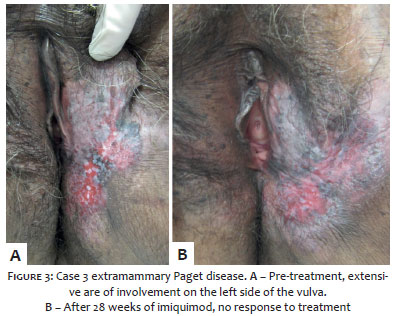
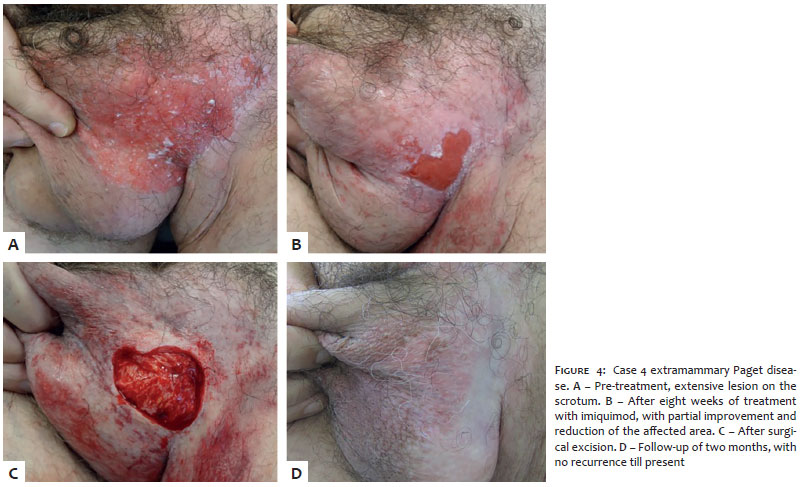
Patient 3, 64 years old, diagnosed with Paget disease in the vulva with no systemic involvement, underwent surgical treatment between 2014 and 2016, with recurrence. She started treatment with IQM in 2016, finishing 28 weeks of application; however, there was no satisfactory response, and she had to undergo a new surgical excision of the lesion in 2017, that yielded margins free of the tumor. Two months after the surgery she developed recurrence (Figure 3). Patient 4, male and 72 years old, had past history of HTN, acute myocardial infarction with myocardial revascularization, cardiac failure and thrombus on anticoagulant. He was diagnosed with EMPD of the scrotum in 2013, with no systemic involvement. He initially underwent two surgical interventions, with recurrence of the lesion between 2013 and 2016. He started treatment with IQM for eight weeks in 2016, with partial response and reduction of the lesion. He underwent a new surgical intervention, progressing with improvement; he is under follow-up for two years, with no signs of recurrence till present (Figure 4).
EMPD is an extremely rare malignancy, corresponding to 0.7% to 4.3% of the cases of breast malignancies8 and less than 1% of vulvar malignancies.9 Studies on this malignancy are rare, and report years of medical assistance to group the few cases, as we presented here. In seven years of dermatology assistance in a tertiary public hospital in the capital of São Paulo, there were only four cases of EMPD.
Regarding the use of IQM as treatment for EMPD cases, Luyten et al. observed a rate of complete response of 80% of the cases treated with this substance, and believe that the time of IQM could be related to the final result of the treatment.6 H. Machida et al. conducted a systematic review and demonstrated a rate of complete response to treatment of 52 to 80%, with recurrence rate of 19%, however, they highlighted that besides being retrospective, the studies were limited regarding the sample size. In their review, they mentioned other forms of treatment and their recurrence rates: 58% for surgical excision, 0-35% for radiotherapy, 25% for chemotherapy with 5 fluouracil and bleomycin, 38% to 56% for photodynamic therapy, 67% for treatment with ablative laser.10 Thus, thee choice for the appropriate treatment for these patients is extremely important, since these therapies can cause side effects and consequences in the quality of life of the patients.
In this study we report only four cases, what represents an extremely small sample and with little statistical relevance of the data when analyzed in isolation. Of these four cases, two patients (50%) showed complete response to IQM use, while one (25%) showed partial response and another (25%), lack of response. We believe that, despite the rate of complete improvement in our study being of 50%, achieving partial response with the use of imiquimod was also beneficial. The patient had a reduction in the initial size of the lesion, which allowed for a surgical excision with disease-free margins of a considerably smaller lesion, reducing the size of the tumor before the surgery and allowing for a more conservative surgical approach, with less areas for reconstruction, shorter healing time and better cosmetic and functional outcomes. Extensive excisions in the anogenital region can be disfiguring and cause serious functional problems.
One must also consider that, even after surgery, there is a high recurrence rate for EMPD due to its multifocal nature with the presence of tumor in clinically undetectable areas. Of the cases here presented, three underwent previous surgeries and had recurrence of the disease. The two patients that had complete response with IQM progressed recurrence-free during the clinical follow-up period.
There is no consensus regarding duration of treatment, since most studies are retrospective and not standardized. Machida et al. recommend in their review to initiate treatment with IQM three to four times per week for six months, since this treatment seems to be time-dependent. They suggest reducing the frequency of applications in case there are side effects until the therapeutic dose is tolerated.10
The use of IQM in the cases presented was indicated as daily application five times a week, because it is similar to that suggested to treat basal cell carcinoma, another malignancy that can be treated with IQM.11
We believe IQM is a valid treatment for EMPD, and can lead to complete or partial resolution of the disease and avoid mutilating procedures.
John Verrinder Veasey | ORCID 0000-0002-4256-5734
Approval of the final version of the manuscript; study conception and planning; preparation and drafting of the manuscript; data collection, analysis and interpretation; effective participation in research guidance; intellectual participation in propaedeutic and / or treatment of the cases studied; critical review of the literature, critical review of the manuscript
Barbara Arruda Fraletti Miguel | ORCID 0000-0002-0448-0369
Approval of the final version of the manuscript; study conception and planning; preparation and drafting of the manuscript; data collection, analysis and critical review of the literature, critical review of the manuscript
Adriana Bittencourt Campaner | ORCID 0000-0002-3044-3019
Study conception and planning; intellectual participation in propaedeutic and / or treatment of the cases studied
Thiago da Silveira Manzione | ORCID 0000-0003-1914-0129
Study conception and planning; intellectual participation in propaedeutic and / or treatment of the cases studied;
1. Lopes Filho LL, Lopes IMRS, Lopes LRS, Enokihara MMSS, Michalany AO, Matsunaga N. Mammary and extramammary Paget's disease. An Bras Dermatol. 2015;90(2):225-31.
2. Pan Z-Y, Liang J, Zhang Q-A, Lin J-R, Zheng Z-Z. In vivo reflectance confocal microscopy of extramammary Paget disease: Diagnostic evaluation and surgical management. J Am Acad Dermatol. 2012;66(2):e47-53.
3. Sanderson P, Innamaa A, Palmer J, Tidy J. Imiquimod therapy for extramammary Paget's disease of the vulva: A viable non-surgical alternative. J Obstet Gynaecol. 2013;33(5):479-83.
4. Dilmé-Carreras E, Iglesias-Sancho M, Márquez-Balbás G, Sola-Ortigosa J, Umbert-Millet P. Radiotherapy for extramammary Paget disease of the anogenital region. J Am Acad Dermatol. 2011;65(1):192-4.
5. Hanna E, Abadi R, Abbas O. Imiquimod in dermatology: an overview. Int J Dermatol. 2016;55(8):831-44.
6. Luyten A, Sörgel P, Clad A, Gieseking F, Maass-Poppenhusen K, Lellé RJ, et al. Treatment of extramammary Paget disease of the vulva with imiquimod: A retrospective, multicenter study by the German Colposcopy Network. J Am Acad Dermatol. 2014;70(4):644-50.
7. Suzuki H, Wang B, Shivji GM, Toto P, Amerio P, Sauder DN, et al. Imiquimod, a Topical Immune Response Modifier, Induces Migration of Langerhans Cells11The authors have declared a conflict of interest. J Invest Dermatol. 2000;114(1):135-41.
8. Wagner G, Sachse MM. Extramammary Paget disease - clinical appearance, pathogenesis, management. J Dtsch Dermatol Ges. 2011;9(6):448-54.
9. Cowan RA, Black DR, Hoang LN, Park KJ, Soslow RA, Backes FJ, et al. A pilot study of topical imiquimod therapy for the treatment of recurrent extramammary Paget's disease. Gynecol Oncol.2016;142(1):139-43.
10. Machida H, Moeini A, Roman LD, Matsuo K. Effects of imiquimod on vulvar Paget's disease: A systematic review of literature. Gynecol Oncol. 2015;139(1):165-71.
11. Micali G, Lacarrubba F, Nasca MR, Ferraro S, Schwartz RA. Topical pharmacotherapy for skin cancer. J Am Acad Dermatol. 2014;70(6):979.e1- 979.e12.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}