


Aline Lissa Okita1; Samir Arbache2; Dirlene Melo Palmeira Roth1; Luciana Gasques de Souza1; Mariana Morais Tavares Colferai1; Denise Steiner1
Received on: 04/10/2017
Approved on: 09/03/2018
This study was performed at the Dermatology Department of the Universidade de Mogi das Cruzes - Mogi das Cruzes (SP), Brazil.
Financial support: None
Conflict of interests: The author Samir Arbache has links with the company Traderm, which markets products related to the MMP® technique. The authors Aline Lissa Okita, Dirlene Melo Palmeira Roth and Luciana Gasques de Souza teach classes in the MMP® technique course
Systemic oral medications – such as cyclosporine (CYA) or methotrexate (MTX) – for the treatment of psoriasis have limited bioavailability due to incomplete gastrointestinal absorption and first-pass hepatic metabolism. Moreover, they are associated with adverse effects. The application of CYA or MTX using the microinfusion of drugs into the skin method (MMP®) for the treatment of psoriasis vulgaris yielded a therapeutic response with significant reduction of lesions, and absence of side effects. In the present report, the authors describe 4 cases of psoriasis vulgaris treated using the MMP® method, with the application of CYA or MTX.
Keywords: Cyclosporine; Methotrexate; Psoriasis
Psoriasis is a chronic inflammatory and recurrent skin disease with a worldwide prevalence of approximately 2%. It is associated with a high degree of morbidity and impact on quality of life and the most common clinical presentation is vulgar psoriasis, which represents 85% to 90% of cases. 1-3 Due to its diverse clinical presentations, treatment should be individualized, taking into account the location of the lesions, the impact on the patient’s quality of life, and the coexistence of psoriatic arthritis.
Three modalities are mainly used, isolatedly or in combination: 1) topical agents, 2) phototherapy and 3) systemic medications. Both phototherapy and systemic medications are used in moderate to severe cases, which are defined as those with 10% or more of involvement of the body area (BSA Index - Body Surface Area); or a score equal or greater than 10 points in the Psoriasis Area Severity Index (PASI) or in the Dermatology Quality of Life Index (DQLI). The most commonly used systemic medications are methotrexate (MTX), acitretin and cyclosporine (CYA).4,5
Methotrexate is a teratogenic substance used orally, subcutaneously or intramuscularly. In addition to being associated with gastrointestinal intolerance, it presents a risk of myelosuppression and hepatotoxicity.6 Its bioavailability is limited by oral route due to incomplete absorption by the gastrointestinal tract (GIT) in addition to the hepatic first-pass metabolism, releasing only small concentrations of the drug in the systemic circulation despite the ingestion of high doses. The reduced folate carrier 1 (RFC1), a ubiquitous transmembrane carrier protein, may limit oral absorption of MTX when saturated, which occurs from 15mg MTX.7,8
Cyclosporine, a calcineurin inhibitor available for oral or intravenous use, has a rapid response as a treatment for psoriasis, however it can be nephrotoxic and increase blood pressure levels, in addition to being associated with side effects such as hydroelectrolytic disorders, hyperlipidemia, among others. Its bioavailability is also limited in the oral form due to low absorption and hepatic first-pass metabolism.9-14
In order to maintain and possibly improve therapeutic efficacy and at the same time decrease the side effects of systemic treatments, the authors propose the treatment of patients bearers of psoriasis vulgaris via the microinfusion of drugs through the skin (MMP®), which was described by Arbache15,16 with the use of MTX (25mg/ml sterile vial) (Thevametho®, Pharmachemie BV, Haarlem, The Netherlands) (imported by Teva Farmacêutica Ltda., São Paulo, Brazil) and CYA (50 mg/ml sterile vial) (Sandimmun®, Novartis, São Paulo, Brazil).
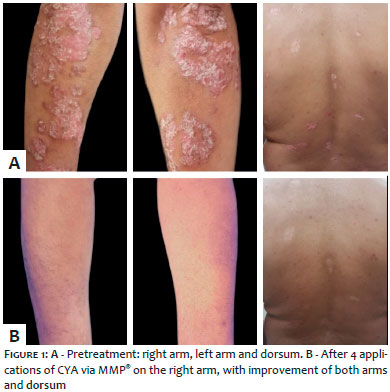
Case 1: Thirty-eight-year-old male patient, frequent consumption of alcoholic drink, bearer of psoriasis vulgaris with lesions in the upper limbs and trunk for nine years. The patient reported previous use of acitretin and MTX, which were suspended due to side effects. The patient received 4 applications of MMP® with 12.5 mg/ml CYA in the lesions located in the right forearm, with a two-week interval. Serum cyclosporinemia was not detectable at 8 hours after the intervention, and laboratory tests and blood pressure levels were kept within normal range. There was no complaint of adverse effects by the patient. All the lesions, both those treated on the right forearm and those not treated on the left arm and on the back, receded (Figure 1).
Case 2: Twenty-seven-year-old male patient, bearer of psoriasis plaques for 5 years. Lesions located in the anterior and posterior regions of the right leg were resistant to topical therapy. The patient underwent 3 MMP® sessions with 25 mg/ml MTX distributed among the lesions. There was a decrease in desquamation and thickness, and remission of pruritus 2 weeks after the first application (Figure 2). After a series of 3 applications every 2 weeks, there was complete remission of the lesions. No methotrexate serum levels were detected the day after the application, nor there were complaints of side effects.
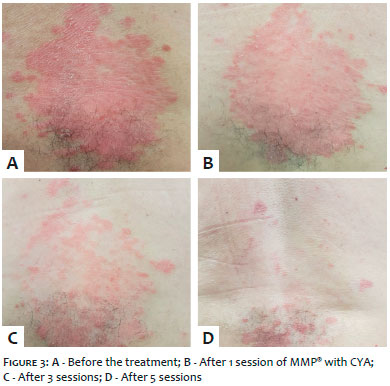
Case 3: Fifty-eight-year-old male patient, hypertensive, history of stroke with left hemiparesis for 12 years, under continuous use of captopril, aspirin, atenolol and amlodipine. Bearer of psoriasis in localized plaques for 17 years, resistant to topical treatment. The patient underwent 5 MMP® sessions with 12.5 mg/ml CYA every 2 weeks in the lesion located in the dorsum, with improvement of approximately 90% of the lesion (Figure 3). The patient had good tolerance to the procedure, without need for topical analgesia. Serum cyclosporinemia after 6 hours was undetectable. Laboratory tests and blood pressure levels were unchanged. The patient is still under treatment.
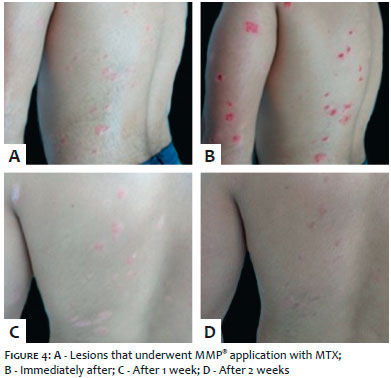
Case 4: Twenty-two-year-old male patient, with plaques of psoriasis for 2 years, having previously improved with oral MTX, having nevertheless not adhered to the treatment, experiencing recurrence of the lesions. Initial PASI: 10.4. An application of MMP® with MTX was performed in the lesions located on the dorsum and left arm (Figure 4). After 1 week, the lesions became less thick and scaly, and only macules were observed at the site of the treated lesions after 2 weeks, improving the appearance of the lesions when looked at from distance (Figures 5 and 6). The patient remains under treatment.
The patients were duly informed about the treatment and signed a Free and Informed Form of Consent.
The treatment of moderate to severe psoriasis involves drugs that might lead to possible side effects.4 Some studies have investigated the possibility of using topical MTX as an alternative, which would reduce the occurrence of such effects. Due to the fact it is a water-soluble molecule, it has limited ability to permeate the stratum corneum, and its use in untouched skin is ineffective.17,18 Therefore, techniques such as electroporation, iontophoresis and ablative lasers were used aimed at increasing its permeation through the skin, with therapeutic response in the treatment of psoriasis.18-20
Similarly, studies on topical use of CYA suggested ineffectiveness on untouched skin.21-25 Griffiths et al. obtained therapeutic response following intralesional injection of 2 ml of 17 mg/ml CYA in psoriasis lesions 3 times per week with undetectable levels of serum cyclosporinemia. Despite the application of considerable amount of medication, due to the CYA’s lipophilic characteristic, it would rapidly redistribute through the tissues, becoming undetectable at plasma levels. The main side effect observed in the study was pain caused by the procedure.26 Using the MMP® technique 27 it was possible to infuse the drug directly in the lesions with excellent patient tolerance after topical anesthesia. The percutaneous injection of the drug has a powerful local effect and is capable of avoiding hepatic first pass metabolism, reaching the systemic circulation in a low and undetectable concentration, nevertheless enough to obtain therapeutic response, meaning that treatment of patients with moderate to severe psoriasis, as well as of lesions resistant to other therapies can be carried out without side effects.
Treatment with the MMP® technique using MTX or CYA solution demonstrated good tolerability, lack of adverse effects, rapid response (already noticed within 2 weeks), and effectiveness both in lesions that have been treated isolatedly and in distant lesions that did not undergo the application.
MMP® performed with CYA or MTX can be a novel treatment modality for psoriasis that arise in resistant plaques, in difficult-to-treat locations, and in patients at risk of systemic treatment related complications. Further studies are needed aimed at defining protocols and randomized clinical trials in order to determine the effectiveness and efficiency of MMP® in the treatment of psoriasis with MTX and CYA.
Aline Lissa Okita | ORCID 0000-0002-3796-137x
Study design and production. Data collection and analysis. Writing of the manuscript, article review and final text approval.
Samir Arbache | ORCID 0000-0003-4409-4937
Study design, article review and approval of the final text.
Dirlene Melo Palmeira Roth | ORCID 0000-0003-1007-5498
Article review and approval of the final text.
Luciana Gasques de Souza | ORCID 0000-0001-5160-7572
Article review and approval of the final text.
Mariana Morais Tavares Colferai | ORCID 0000-0002-1667-4988
Production and data collection, article review and approval of the final text.
Denise Steiner | ORCID 0000-0001-6450-9234
Article review and approval of the final text.
1. Christophers E. Psoriasis - epidemiology and clinical spectrum. Clin Exp Dermatol. 2001; 26(4): 314-20.
2. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009; 361(5): 496-509.
3. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263-71
4. Menter A, Griffiths CE. Current and future management of psoriasis. Lancet. 2007; 370(9583): 272-84.
5. Sociedade Brasileira de Dermatologia. Consenso brasileiro de Psoríase 2012: guias de avaliação e tratamento. 2 ed. Rio de Janeiro: Sociedade Brasileira de Dermatologia; 2012. 172 p.
6. Kalb RE, Srober B, Weinstein G et al. Methotrexate and psoriasis: 2009 National Psoriasis Foundation Consensus Conference. J Am Acad Dermatol. 2009;60(5):824-37.
7. Schiff MH, Jaffe JS, Freundlich B. Head-to-head, randomised, crossover study of oral versus subcutaneous methotrexate in patients with rheumatoid arthritis: drug-exposure limitations of oral methotrexate at doses ≥15 mg may be overcome with subcutaneous administration. Ann Rheum Dis. 2014;73(8):1549-51.
8. Goodman SM, Cronstein B, Bykerk VP. Outcomes related to methotrexate dose and route of administration in patients with rheumatoid arthritis: a systematic literature review. Clin Exp Rheumatol 2015;33(2): 272-78.
9. Heydendael VM, Spuls PI, Opmeer BC, de Borgie CA, Reitsma JB, Goldschmidt WF, et al. Methotrexate versus ciclosporin in moderate-to-severe chronic plaque psoriasis. N Engl J Med. 2003; 349(7): 658-65.
10. Griffiths CEM, Clark CM, Chalmers RJ, Li Wan Po A, Williams HC. A systematic review of treatments for severe psoriasis. Health Technol Assess 2000; 4(40): 1-125.
11. Zachariae H, Kragbelle K, Hansen HE, Marcussen N, Olsen S. Renal biopsy findings in long-term ciclosporin treatment of psoriasis. Br J Dermatol. 1997; 136(4): 531-35.
12. Lowe NJ, Wieder JM, Rosenbach A, Johnson K, Kunkel R, Bainbridge C, et al. Long-term low-dose ciclosporin therapy for severe psoriasis: effects on renal function and structure. J Am Acad Dermatol. 1996; 35(5 Pt1): 710-19.
13. Paul CF, Ho VC, McGeown C, Christophers E, Schmidtmann B, Guillaume JC, et al. Risk of malignancies in psoriasis patients treated with ciclosporin: a 5 y cohort study. J Invest Dermatol. 2003; 120(2): 211-16.
14. Kolars JC, Awni WM, Merion RM, Watkins PB. First-pass metabolism of cyclosporin by the gut. Lancet. 1991; 338(8781):1488.
15. Arbache S, Godoy CE. Microinfusion of drugs into the skin with tattoo equipment. Surg Cosmet Dermatol. 2013;5(1):70-4.
16. Arbache S, Roth D, Steiner D, Breunig J, Michalany NS, Arbache ST, et al. Activation of melanocytes in idiophatic guttate hypomelanosis after 5-fluorouracil infusion using a tattoo machine: preliminary analysis of a randomized, split-body, single blinded, placebo controlled clinical trial. J Am Acad Dermatol. 2018;78(1):212-15.
17. Su YH, Fang JY. Drug delivery and formulations for the topical treatment of psoriasis. Expert Opin Drug Deliv. 2008; 5(2):235-49.
18. Alvarez¬Figueroa MJ, Blanco¬Mendez J. Transdermal delivery of methotrexate: Iontophoret delivery from hydrogels and passive delivery from microemulsions. Int J Pharm. 2001; 215(1-2):57-65.
19. Taudorf EH, Lerche CM, Vissing AC, Philipsen PA, Hannibal J, D'Alvise J, et al. Topically applied methotrexate is rapidly delivered into skin by fractional laser ablation. Expert Opin. Drug Deliv 2015; 12(7):1059-69.
20. Lee WR, Shen SC, Fang CL, Zhuo RZ, Fang JY. Topical delivery of methotrexate via skin pretreated with physical enhancement techniques: low fluence Erbium:YAG laser and electroporation. Lasers Surg Med. 2008; 40(7): 468¬-76.
21. Hermann RC, Taylor RS, Ellis CN, Williams NA, Weiner ND, Flynn GL, et al. Topical cyclosporine for psoriasis: in vitro and clinical study. Skin Pharmacol. 1988; 1:246¬-9.
22. Heule F, Laijendecker R, van Joost T. Topical cyclosporin A treatment in psoriasis and other dermatological diseases: theoretical and practical aspects, J Dermatol Treat. 1992; 2:149-53.
23. Griffiths CEM, Powles AV, Baker BS, Fry L, Valdimarsson H. Topical cyclosporin and psoriasis. Lancet. 1987; 329(8536):806.
24. Gilhar A, Winterstein G, Golan DT. Topical cyclosporine in psoriasis. J Am Acad Dermatol. 1988;18(2 Pt 1):378-¬9.
25. Schulze HJ, Mahrle G, Steigleder GK. Topical cyclosporin A in psoriasis. Br J Dermatol. 1990; 122(1): 113-4.
26. Ho VC, Griffiths CE, Ellis CN, Gupta AK, McCuaig CC, Nickoloff BJ, et al. Intralesional cyclosporine in the treatment of psoriasis. A clinical, immunologic, and pharmacokinetic study. J Am Acad Dermatol. 1990;22(1):94¬-100
27. Contin LA. Male androgenetic alopecia treated with microneedling alone or associated with injectable minoxidil by microinfusion of drugs into the skin. Surg Cosmet Dermatol. 2016; 8(2):158-61.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}