


Karisa Farias Miksza Thölken1; Fabiane Mulinari Brenner2; Betina Werner3; Murilo Calvo Peretti4; Luciana Menezes Azevedo1
Sarcoidosis is a non-infectious granulomatous disease of unknown etiology in which environmental, infectious, immunological, and genetic factors appear to be correlated. Clinical manifestations can occur in any organ, however there is predominance in the lungs and in intrathoracic lymph nodes. The cutaneous involvement of the disease occurs in roughly 25% of cases, with cutaneous filling procedures figuring as a potential trigger. The authors of the present article report a case of a patient who had granulomatous lesions on the face following cutaneous filling with hyaluronic acid. In the investigation of cutaneous lesions, the patient presented diagnostic criteria for sarcoidosis, with extensive pulmonary involvement.
Keywords: sarcoidosis; granuloma; hyaluronic acid
Sarcoidosis is a disease that involves multiple organs, usually affects adults, with predominance in dark skin individuals and women. Its etiology remains unknown, however different factors have been implicated: polygenic inheritance, microorganisms (Mycobacterium tuberculosis, bacteria, herpes virus), exposures to mold, birds, insecticides, metals (aluminum, zirconium) and drugs such as interferon alpha. The interaction between genetic and environmental factors is probably responsible for the condition’s pathogenesis. Diagnosis is established in the presence of clinical and radiological findings, and histological evidence of non-caseous epithelioid granulomas in the involved organs, after the exclusion of other causes. Any organ can be affected by sarcoidosis’ granulomas, however pulmonary and / or intrathoracic lymph nodes involvement occur in more than 90% of cases, which are classified according to the Scadding criteria into: I) Hilar lymphadenopathy or mediastinal; II) Hilar lymphadenopathy or mediastinal and lesions of the pulmonary parenchyma; III) Lesions of the pulmonary parenchyma without adenomegalies and signs of pulmonary fibrosis; IV) Fibrosis signs in the pulmonary parenchyma. Cutaneous involvement occurs in a percentage that varies from 10 to 25% of cases. The most common cutaneous lesion is the erythema nodosum, which generally suggests a better prognosis. Clinical polymorphism, however, is a feature of sarcoidosis. Macules, papules, plaques, nodules, erythroderma, alopecia, lupus pernio, and infiltrations in tattoos or scars might be cutaneous manifestations of sarcoidosis.1,3
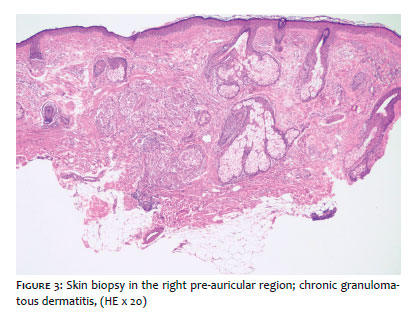
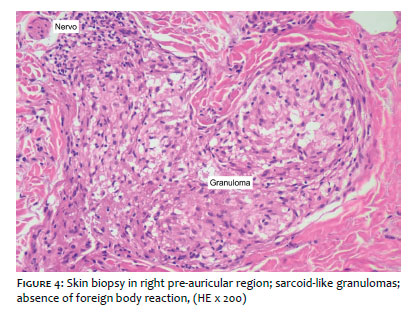
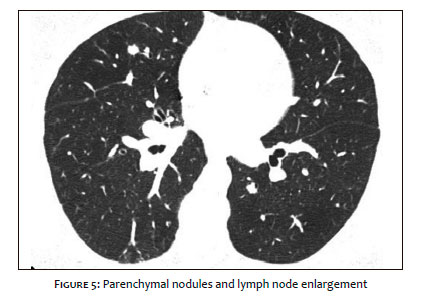
Five months after undergoing a cutaneous filling procedure with hyaluronic acid in the glabellar area, a 58-year-old female patient presented erythematous lesions infiltrated in both malar, left frontal and right pre-auricular regions (Figures 1, 2). Systemic symptoms (dry cough and polyarthralgia, without criteria for arthritis in the previous 4 to 6 months) were described in the initial evaluation only in the medical records and had not been a reason to seek medical attention previously, since they were non-significant and occasional. The anatomopathological examination of the skin of the right pre-auricular region demonstrated chronic granulomatous dermatitis with sarcoid-like granulomas (Figures 3 and 4). A computerized tomography scan of the thorax demonstrated multiple parenchymal nodules and lymph node enlargement in the middle mediastinum (Figures 5). Radiography of hands, echography/ultrasound of abdomen, electrolytes as well as the dosage of angiotensin converting enzyme were normal. Thus, based on clinical, radiological and histological data, the diagnosis of sarcoidosis was established. The patient started to use prednisone (0.5mg day / kg). Three weeks later, with improvement of the lesions, a decision was made for gradually decrease the use of prednisone. Three months after the suspension of prednisone, the patient maintained improvement of the cutaneous condition and stabilization of the pulmonary condition. One year later, however, she reported a new outbreak, with similar development and treatment.
Cutaneous filling substances have been increasingly used for the correction of unaesthetic dermatoses. Products based on collagen, autologous fat, poly-L-lactic acid, calcium hydroxyap-atite, polymethylmethacrylate and hyaluronic acid are approved for esthetic use. 4 Despite the fact that hyaluronic acid is a component of the extracellular matrix — and thus less immunogenic and more biocompatible - adverse effects occur in 0.05-0.15% of cases. The main adverse events described are hypersensitivity and inflammation at the injection site, however bacterial infection, herpes reactivation, generalized scleromyxedema, and embolization with livedoid pattern, scar sarcoidosis, and systemic sarcoidosis have also been reported. 5,6 Local complications usually arise between 6 and 24 months after the implantation of the filling material. Cutaneous sarcoidosis has been reported in scars, tattoo sites, venipuncture, intramuscular and hyaluronic acid injections after a variable period of a few months to 38 years. 7 Regarding the onset of sarcoidosis following the use of cutaneous fillers, it is known that the longer the time interval between the two events, the lesser is the possibility of it being a foreign body granuloma — an important differential diagnosis vis a vis pure cutaneous sarcoidosis.8,9 According to the literature review, it is postulated that the application of the filler can evidence signs of a subjacent sarcoidosis or even trigger the clinical picture in a previously predisposed patient.10 In the present case, the procedure was the probable triggering factor for the clinical manifestation of the systemic disease, characterized by cutaneous lesions and pulmonary involvement rather than the isolated involvement of the skin after use of the local injection. The following features corroborated for the diagnosis: radiological characteristics typical of pulmonary involvement; granulomatous cutaneous manifestations on the face, but not exactly where the previous application of the filler was carried out; histology compatible with sarcoidal granuloma rather than with the foreign body type or other granulomatous disease form.
In this manner, performing the clinical evaluation of symptoms that indicate involvement of the lung or other organs in sarcoidosis is crucial before carrying out cutaneous fillings, given that this procedure could trigger or exacerbate this disease in susceptible individuals.
Karisa Farias Miksza Tholken:
Manuscript planning, drafting, writing and discussion
Fabiane Mulinari Brenner:
Manuscript supervision, guidance, discussion and correctionBetina Werner:
Clinical-anatomopathological correlation and diagnostic analysis
Murilo Calvo Peretti:
Clinical follow-up of the patient
Luciana Menezes Azevedo:
Clinical follow-up of the patient
1. Kirsten, D. Pulmonary sarcoidosis: current diagnosis and treatment. Dtsch Med Wochenschr. 2013; 138(11):537-41
2. Zhou Y, Lower EE, Li H, Baughman RP. Clinical management of pulmonary sarcoidosis. Expert Rev Respir Med. 2016;10(5):577-91
3. Wanat KA, Rosenbach M. Cutaneous Sarcoidosis. Clin Chest Med. 2015; 36(4):685-702.
4. Talarico S, Hassun KM, Monteiro EO, Parada MOB, Buratini LB, Arruda L, et al. Safety and efficacy evaluation of a new hyaluronic acid based filler in the treatment of nasolabial folds and lips outline. Surg Cosmet Dermatol. 2010; 2(2):83-6
5. Cheng LY, Sun XM, Tang MY, Jin R, Cui WG, Zhang YG. An update review on recent skin fillers. Plast Aesthet Res 2016; 3:92-9.
6. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune--mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013; 43(2):241-58
7. Lowe NJ, Maxwell CA, Lowe P, Duick MG, Shah K. Hyaluronic acid skin fillers: adverse reactions and skin testing. J Am Acad Dermatol. 2001; 45(6):930-3
8. Fitzgerald R, Bertucci V, Sykes JM, Duplechain JK. Adverse Reactions to Injectable Fillers. Facial Plast Surg. 2016; 32(5):532-55.
9. Edwards PC, Fantasia JE. Review of long-term adverse effects associated with the use of chemically-modified animal and nonanimal source hyaluronic acid dermal fillers. Clin Interv Aging. 2007;2(4):509-19.
10. Marcoval J, Mañá J, Penín RM, Figueras I, Labori M, Llatjos R. Sarcoidosis associated with cosmetic fillers. Clin Exp Dermatol. 2014; 39(3):397-9.
This study was performed at the Hospital de Clínicas da Universidade Federal do Paraná (UFPR) - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}