


Guilherme Bueno de Oliveira1; Natália Cristina Rossi Bueno de Oliveira2; Bárbara Maria Tarraf Moreira3; Marcela Ferraz Awada3; Jonas Eduardo Nunes Franco Neto3
Introduction: Molluscum contagiosum is a dermatovirosis caused by a poxvirus. In the literature there are descriptions of different therapeutic approaches of this infection.
Objective: To evaluate the efficacy of imiquimod – isolated and associated with curettage – in the treatment of molluscum contagiosum.
Methods: Group A: 20 patients used 5% imiquimod cream 3 times a week for 6 weeks. Group B: 10 patients used a creamy base 3 times a week, for 6 weeks. After the initial 6 weeks, all patients underwent curettage.
Results: Group A: 31% decrease in the number of lesions in the 6th week, with a curettage effectiveness of 97.6%; Group B: 4.8% increase in the number of lesions in the 6th week, with a curettage effectiveness of 81.1%. The mean value for the pain level during curettage was 1.8 for Group A and 3.0 for Group B.
Conclusions: Due to the facts that the rate of cure of contagious molluscum lesions increased and the pain decreased when the curettage procedure was conducted after the use of the immunomodulator, it was possible to conclude that the association of 5% imiquimod cream to the curettage may be a therapeutic possibility.
Keywords: Molluscum Contagiosum; Dermatology; Dermatologic Surgical Procedures
Molluscum contagiosum (MC) is a viral skin infection caused by a poxvirus of the genus Molluscipox virus 1, that can affect any area of the body with a predilection for the upper trunk, axillae, antecubital and popliteal fossae and inguinal region.1-4 It is a universal infection, with higher prevalence in tropical areas and higher incidence in children, also affecting sexually active and immunodeficient adults.3 Transmission occurs by direct contact, contaminated fomites and auto-inoculation.3,5 Clinical presentation is with small, sessile, firm papules with umbilication. The diagnosis is clinical because of the appearance of the lesions and, when in doubt, histology can be useful.6-8 Although benign and usually self-limited, the lesions can present some complications such as inflammation, pruritus, eczematous inflammation, secondary bacterial infection and permanent scars. For these reasons, treatment of the lesions is recommended.2,3
Different approaches for this infection are described in the literature, including observation only, since it can have spontaneous resolution.5,9 Many studies mentioned curettage as the most effective technique, with lower rates of recurrence, considered as gold standard for the treatment of MC in many studies; however, there is no consensus on the best method.1,4,7,9,10 Regarding treatment choice, many aspects should be considered, including effectiveness and recurrence, secondary aspects such as physical and psychological tolerance to therapy, patient’s or guardian’s preference, financial situation of the family and the time availability and ease of access to the medical practice.11 The most commonly mentioned treatment techniques in the literature include cryotherapy, curettage, laser and the topical use of multiple substances, the most common ones being tretinoin, potassium hydroxide, imiquimod, cantharidin, trichloroacetic acid and a combination of salicylic and lactic acid.3,8
The objective of this study was to evaluate the efficacy of imiquimod for the treatment of MC alone and associated to curettage, highlighting the effectiveness of the treatment, rates of complications and assessment of the level of pain during the surgical procedure.
A prospective, longitudinal analytic, single center study of 30 patients submitted to treatment with imiquimod and curettage of MC of extra facial areas was carried out. The study followed the ethical guidelines from the Helsinki declaration. Treated patients were followed up on the system of the practice.
The patient selected for the study should have, compulsory, MC in extra facial areas. We included cases that were not treated for the condition for more than six months.
Any patient who had previous treatment for MC lesions less than six months before the beginning of the study, bacterial infection on the site, history of allergy to the formula component and patients who did not want to be treated with curettage at the end of the study were excluded from the study.
Patients were randomly divided into two distinct groups: Group A or Group Case Study was made of 20 patients using imiquimod 50 mg/g (Ixium®, Farmoquímica) sporadically and localized only over the MC lesions, applied with a cotton tip Cotonete® (Johnson & Johnson) and covered by micropore tape. The product should be in contact with the lesions for 8 hours and should be applied three times per week (defined as Monday, Wednesday and Friday), for 6 weeks, with a total of 18 applications; Group B or Control Group, made of 10 patients who used cream base in the same way, length of exposure and total applications as those selected in Group A.
In week 7, after using imiquimod or cream base for 6 weeks, patients were treated with curettage of the MC lesions. This was performed with curette 4 after topical anesthesia with lidocaine (70mg/g) and tetracaine (70mg/g) cream under occlusion for 30 minutes on each lesion. Over the curetted lesions, micropore tape dressings were applied.
The sociodemographic variables included were gender and age. The MC lesion count before beginning of the treatment, 6 weeks after imiquimod or cream base and 6 weeks after the curettage; description of the adverse effects during the use of imiquimod or cream base; level of pain reported by the patient during curettage were used for the evaluation of the study according to the following stratification:
Pain zero: absence of pain during the procedure
Pain 1: mild pain or discomfort
Pain 2: tolerable pain and would do it again if needed
Pain 3: unbearable pain and would not do it again
The level of pain was analyzed the t test for 2 independent samples, with equal variance and normal distribution
The study was conducted with 30 patients, 16 female and 14 males. Mean age in years of Group A, with 9 female patients and 11 male patients, was of 8.0 with a range between 6 and 11 years. Group B, with 7 female patients and 3 male patients, the mean age was 8.5 ranging between 5 and 12 years. The distribution of the lesions was: 52% on the trunk, 37% on the thighs and buttocks and 11% on the arms.
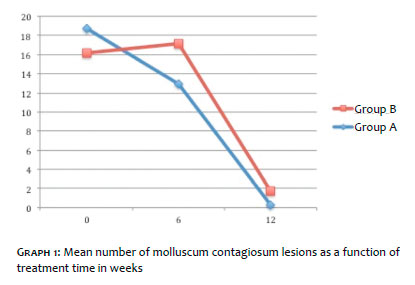
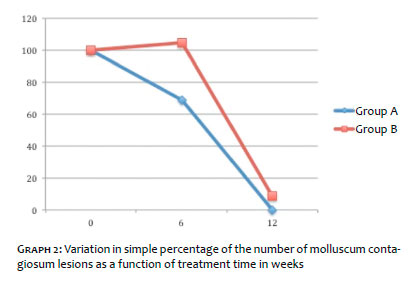
After statistical analysis of the data by total number of MC lesions and plain percentages, we highlight the following findings after comparison of the 2 groups: the mean number of MC lesions ( Graph 1) in Group A in week zero was 18.75 lesions, 12.95 lesions after 6 weeks using imiquimod and in the 12th week (6 weeks after curettage) 0.3 lesions; in Group B in week zero was 16.4 lesions, 17.2 after using cream base for 6 weeks and in the 12th week (6 weeks after curettage) 1.4 lesions. Results in graph 2 show the percentage of variation of MC lesions by time: Group A had a reduction of 31% in the number of lesions in the 6th week, with a remaining 1.6% of the total lesions of the beginning in the 12th week, with an efficacy of 97.6% for curettage; Group B had an increase of 4.8% in the total number of lesions in the 6th week with a remaining 8.5% of the total of lesions of the beginning in the 12th week, resulting in an efficacy of 81.1% for curettage in this group.
Graph 3 shows the mean level of pain during curettage in degrees as described in the methods section between 0 and 3 for all patients of both groups. Group A had a mean level of pain of 1.8, while Group B had a mean level of pain of 3.0. the reduction in the level of pain was statistically significant, with p<0.001 in t test for the group that used imiquimod before curettage. The related adverse events were: in Group A, 20 patients had irritation, 20 erythema and 3 edema with the use of imiquimod and in Group B there was no adverse event during the treatment.
Molluscum contagiosum is a common viral infection of childhood, affecting mainly children in school age. It manifests clinically as sessile and umbilicated papules almost always on the trunk, limbs and genital area, what was also seen in this study.
The lesions are characterized by being self-limited, with spontaneous regression from 6 to 18 months.
Treatments are divided into destructive, immunomodu-lators and antivirals. For being the most common, destructive treatments are the most reported in the literature, from topicals such as the application of potassium hydroxide solution, can-tharidin, tretinoin, salicylic acid and lactic acid, to procedures such as curettage and liquid nitrogen. However, the treatment with immunomodulators has good responses for the treatments of other viral skin infections, such as topical imiquimod and systemic cimetidine. This research showed a 31% reduction in the number of MC lesions in Group A, that used imiquimod three times a week for 12 weeks whereas Group B, that used cream base in the same way as Group A, had a 4.9% increase in the number of MC lesions. The results here found indicate imiqui-mod is superior to the other classic topical therapies, such potassium hydroxide, that had a level of efficacy of 25% in double the application time (12 weeks) and did not show total clearing in any patient when used as 5% by Schmitt12 and as 10% by Machado13 . However, it also had inferior results when compared to invasive dermatological procedures such as curettage.12-14
The second objective of this study was to evaluate the level of pain by a numerical scale detailed in the methods section during curettage, to which all patients were submitted for the lesions that remained after the first period. Group A had a mean pain of 1.8 in the numerical scale, whereas Group B had a mean of 3.0, with a statistically significant difference. This observation could be due to the stimulation of the cellular immunity by imiquimod 5% cream, leading to an inflammatory epidermal reaction also found in other studies,15 what could make a destructive treatment easier and less painful, besides the elimination of the virus.
After curettage in week 6, a new MC lesion count was performed in week 12, with data pointing to a clearing efficacy of 97.6% for Group A and 81.1% for Group B. this difference was important because it is an auto-infectious disease, with transmission via fomites or direct contact to other children1 and is in accordance to the literature, that demonstrates levels of efficacy of isolated curettage between 61 and 100%.16 This higher rate of elimination in Group A was probably due to the immu-nomodulating properties of imiquimod on the viral lesions and by the fragility of the inflamed skin.15
Regarding side effects during the 6 weeks, in Group A, all patients had irritation and erythema and 10% of edema on the application site. Group B did not show any adverse event. Color changes, formation of blisters, secondary infections or scars were not identified in neither study group. The adverse events were mild and expected, in concordance with studies with imiquimod in the literature for the treatment of MC.16,17
Regarding molluscum contagiosum, the scientific background for the initiation of a therapeutic intervention still have not reached a consensus in the literature, leaving doubts to dermatologists about which is the best decision to make in terms of performing or not an interventionist treatment, as well as a topical therapeutic option before surgical procedures. Even though observation can be an option, many parent and patients prefer the fast resolution of lesions with the aim of relieving the discomfort, control dissemination of the lesions, prevent the development of scars or secondary bacterial infections, and also, be used by aesthetic and social reasons. This study showed positive and satisfactory results in comparison to the control group, with a clearance of 97.6% of the MC lesions and reduction in the level of pain during curettage, the most described surgical procedure in the literature, with the association of two distinct types of treatment, imiquimod as an immunomodulator and curettage as destructive. This way, we conclude that the association of imiquimod 5% cream with curettage can be an important therapeutic option for daily practice. We highlight that more studies in the literature are important to confirm this observation.
Guilherme Bueno de Oliveira:
Statistical analysis and approval of the final version of the manuscript
Conception and planning of the study
Active participation in supervising the research Intellectual participation in propaedeutic management and/or treatment of the cases studied
Critical review of the manuscript
Natália Cristina Rossi Bueno de Oliveira:
Active participation in supervising the research
Intellectual participation in propaedeutic management and/or treatment of the cases studied
Critical review of the manuscript
Bárbara Maria Tarraf Moreira:
Collection, analysis and interpretation of data
Critical review of the literature
Jonas Eduardo Nunes Franco Neto:
Collection, analysis and interpretation of data
Critical review of the literature
1. Hanna D, Hatami A, Powell J, Marcoux D, Maari C, Savard P, et al. A prospective randomized trial comparing the efficacy and adverse effects of four recognized treatments of molluscum contagiosum in children. Pediatr Dermatol. 2006; 23(6):574-9.
2. Hanson D, Diven DG. Molluscum Contagiosum. Dermatol Online J. 2003; 9(2):2.
3. Romiti R, Ribeiro AP, Romiti N. Evaluation of the effectiveness of 5% potassium hydroxide for the treatment of molluscum contagiosum. Pe-diatr Dermatology. 2000;17(6):495.
4. Short KA, Fuller LC, Higgins EM. Double-blind, randomized, placebo-controlled trial of the use of topical 10% potassium hydroxide solution in the treatment of molluscum contagiosum. Pediatr Dermatol. 2006;23(3):279-81.
5. Bolognia JL, Jorizzo JL, Rapini RP. Dermatology. EUA:Mosby; 2003.
6. Bauer JH, Miller OF, Peckham SJ. Medical Pearl: confirming the diagnosis of molluscum contagiosum using 10% potassium hydroxide. J Am Acad Dermatol. 2002; 56(5 Suppl):S104-5.
7. van der Wouden JC, van der Sande R, van Suijlekom-Smit LW, Berger M, Butler CC, Koning S. Interventions for Cutaneous Molluscum Contagiosum. Cochrane Database Syst Rev. 2009; (4): CD004767.
8. Jones S, Kress D.Treatment of Molluscum Contagiosum and Herpes Simplex Virus. Cutis. 2007; 79(4 Suppl):11-17.
9. Baverl C, Feller G, Goerdt S. Experience in Treating Molluscum Con- tagious in Children with Imiquimod 5% Cream. Br J Dermatol. 2003;149(Suppl 66):25-8.
10. Romiti R, Ribeiro AP, Grinblat BM, Rivitti EA, Romiti N. Treatment of Molluscum Contagiosum with Potassium Hydroxide: a Clinical Approach in 35 Children. Peditr Dermatol.1999;16(3):228-31.
11. Leslie KS, Dootson G, Sterling JC. Topical salicylic acid gel as a treatment for molluscum contagiosum in children. J Dermatol Treat. 2005; 16(5-6):336-40.
12. Schmitt, JV; Marchioro, HZ. Low efficacy in the use of 5% potassium hydroxide solution to treat contagious molluscum. Surg Cosmet Dermatol 2011;3(4):368-9.
13. Machado RB; Leal TF; Bonfá R; Werlang ME, Weber MB. Molluscum con-tagiosum in children: comparative treatments. Surg Cosmet Dermatol. 2010;2(4):272-5.
14. Brown J, Janniger CK, Schwartz RA, Silverberg NB. Childhood molluscum contagiosum. Int J Dermatol. 2006;45(2):93-9.
15. Val ICC, Faria R, Arcoverde F, Gomes M,Val R, Sampaio L, et al. Case Series of Anogenital Warts in Children Treated with Imiquimod. DST - J Bras Doenças Sex Transm 2011; 23(2): 101-105.
16. Gaspar MA, Pinheiro AF, Sanches A. Treatment of molluscum contagiosum in children: an evidence-based review. Rev Port Med Geral Fam. 2012;28(6):418-26.
17. Theos AU, Cummins R, Silverberg NB, Paller AS. Effectiveness of imi-quimod cream 5% for treating childhood molluscum contagiosum in a double-blind, randomized pilot trial. Cutis. 2004; 74 (2): 134-8, 141-2.
Study conducted at Vitta Dermatologia - São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}