


Rafael Abdala Beicher1; Denise Steiner2; Elizabeth Leocádia Fernandes3
Amyloidosis is characterized by the deposition of a modified protein. It can affect the skin by accumulating in the papillary dermis. In general, it develops with brownish maculae predominant in the interscapular region, and rarely coursing with generalized forms. This report describes a 59 year-old female patient who had had a spot in the lower back for 43 years, which in the last 8 years had progressively spread for the entire body. Dermoscopy has proven extremely effective in locating the various foci of pigmentary incontinence, which together with apoptotic keratinocytes constitute the pathophysiological basis for the formation of the amyloid protein.
Keywords: AMYLOIDOSIS; CONGO RED; DERMOSCOPY
Amyloidosis is a buildup, in any affected organ, of an abnormal protein which is the result of the combination of polysaccharides and globulin. Macular amyloidosis is the most common subtype of cutaneous amyloidosis. It typically presents with pigmentation in a reticular or wavy pattern on the interscapular region, affecting the extensor aspect of arms, forearms and legs1 to a lesser extent, rarely becoming generalized. Histopathology shows deposits of amyloid substance in the papillary dermis and, when stained with congo red under polarized light microscopy, shows greenish birefringence.2 Areas of pigmentary incontinence are also seen on the same location.3 We followed a 59-year-old female patient, born and living in São José dos Campos (SP), who presented with a complaint of a brownish patch in the sacrum for 43 years and progressive enlargement over the past 8 years.
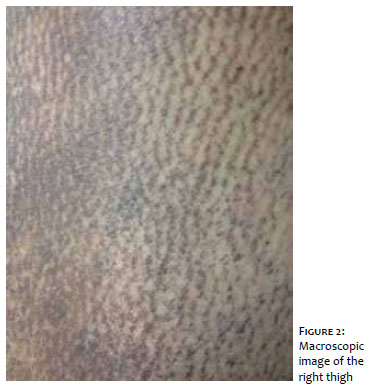
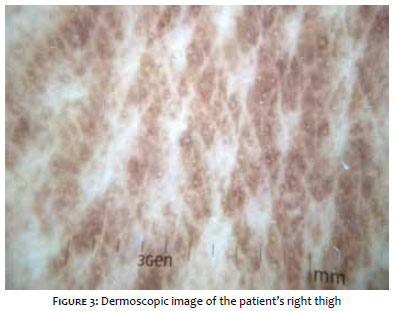
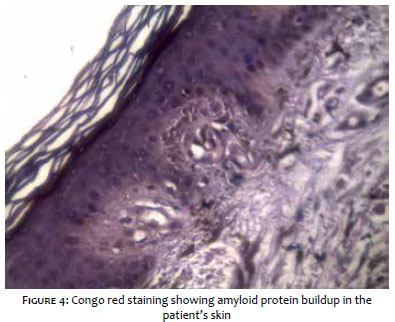
On physical examination, the patient had brownish patches, some of them reticulated, interspersed with normal skin all over the body, sparing only fingers, feet and scalp (Figure 1). On dermoscopy, multiple brown waves on the inferior aspect of the right leg, formed by brownish squared structures with fine streaks in the center of the lesion were of interest (Figures 2 and 3). She denied previous health issues or use of regular medications. Histopathology showed with apoptotic keratinocytes in the epidermis and enlargement of the papillary dermis, with deposition of hyaline eosinophilic globules, besides melanophages and mild superficial perivascular lymphomononuclear infiltrate (Figure 4).
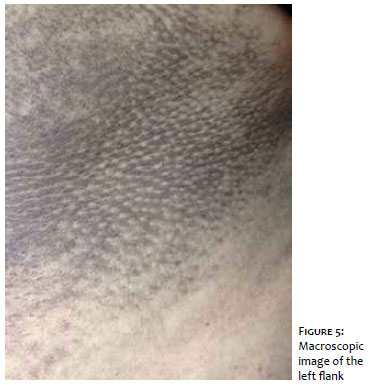
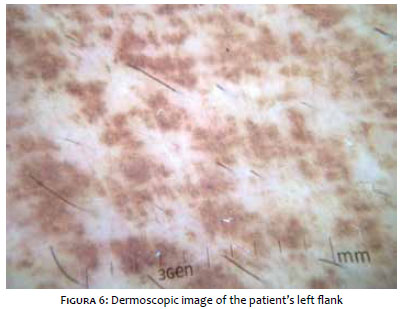
Cutaneous amyloidosis can be classified in primary and secondary. Of the primary forms, macular amyloidosis, like the case described, is the most common type. Still, the generalized presentation, such as our patient’s, is rarely seen in clinical practice.1 Diffuse forms can simulate nevoid pigmentation, such as the poikilodermatous form.2 Clinically, brown-gray patches, with varying diameters between 2-3mm are seen. The reticular or serpiginous pattern is typical. The diagnosis, initially clinical and easily mistaken for many other conditions including lichen simplex chronicus, atrophic lichen planus, lichen sclerosus, atopic dermatitis, hemocromatosis, xanthoma, pitiriasis versicolor, toxic melanoderma, among others, can be differentiated on dermoscopy by the findings of multiple small brown central cubes with fine streaks radiating from the center (Figures 5 and 6). The distinctive histopathological feature is amyloid substance deposition in previously healthy skin without deposition in other organs. It is more commonly
seen in Central and South Americas, Middle East and Asia, perhaps because of cultural habits. There are associated genetic factors as well, as we can see familial cases described in the literature. Other associated factors include ultraviolet B radiation (UVB), Epstein-Barr virus and race.3 During puberty, this type of amyloidosis affects both sexes equally, but there is female predominance between 20 to 50 years of age.3,4
The treatment for this condition is generally disappointing. Topical superpotent steroids are usually used for a short time. Calcipotriol and phototherapy are similarly of limited use.5 Dimethyl sulfoxide can improve pigmentation, but it completely recurs upon discontinuation.3
We demonstrate a florid case of disseminated macular amyloidosis, with characteristic dermoscopic pattern that helps differentiating from other conditions that are clinically similar. There is no question about the importance of the histopathological examination, but we highlight the importance of dermoscopy for the diagnosis of yet another dermatological condition.
Rafael Abdala Beicher
Data analysis and interpretation
Study design and planning
Critical review of the literature
Elizabeth Leocádia Fernandes
Approval of the manuscript's final version
Study design and planning
Denise Steiner
Intellectual participation in the therapeutic approach
Critical review of the literature
Intellectual participation in the therapeutic approach
Critical review of the manuscript
Critical review of the manuscript
1. Breathnach SM. Amyloidosis of the skin. In: Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, et al., editors. Fitzpatrick's dermatology in general medicine. 5th ed. New York: Mcgraw-Hill; 1999. p. 1756-65.
2. Kudur MH, Sathish PB, Sripathi H, Prabhu S. Unusual presentation of generalized macular amyloidosis in a young adult. Indian J Dermatol. 2008;53(4):201-3.
3. Melo BLA, Goes CAM, André NF, Costa IS, Tigre CAF. Amiloidose macular de localização atípica. An Bras Dermatol. 2011;86(4supl1):S24-7.
4. Rasi A, Khatami A, Javaheri SM. Macular amyloidosis: an assessment of prevalence, sex, and age. Int J Dermatol. 2004;43(12):898-9.
5. Khoo BP, Tay YK, Goh CL. Calcipotriol ointment vs. betamethasone 17-valerate ointment in the treatment of lichen amyloidosis. Int J Dermatol. 1999;38(7):539-41.
Study conducted at Universidade Mogi das Cruzes (UMC) – Mogi das Cruzes (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}