


Sandra Tagliolatto; Nancy Vanessa Paranhos Mazon
Post-inflammatory hyperpigmentation is a common consequence of inflammatory dermatoses that tends to affect patients with higher phototypes more frequently and severely. It can be caused by any skin inflammation or lesion, including acne, eczema, contact dermatitis or burns. Topical therapies are generally effective, however in some cases the post-inflammatory hyperpigmentation is resistant to conventional treatments, such as chemical peels and laser therapy. The percutaneous collagen induction technique can be used in postinflammatory hyperpigmentation with good response. The authors describe a case of hyperchromia resulting from a burn caused by Alexandrite laser for hair removal that was resistant to conventional treatments. Based on the literature review and their clinical experience, the authors suggest that the percutaneous collagen induction technique — also known as microneedling — may be included in the therapeutic armamentarium for the treatment of postinflammatory skin hyperpigmentation, especially when there is resistance to conventional treatments.
Keywords: HYPERPIGMENTATION; THERAPEUTICS; NEEDLES
Post-inflammatory hyperpigmentation is a common consequence of inflammatory dermatoses; it tends to affect darker skinned patients with more frequency and severity.
Epidemiological studies show that dyschromias, including post-inflammatory hyperpigmentation, are among the most common complaints in darker racial groups/ethnicities seeking dermatological care. 1
Disorders that cause hyperpigmentation of the skin are frequent, the most common being melasma, lentigos and post-inflammatory hyperpigmentation (PIH).2
PIH probably occurs due to the increased production or deposition of melanin in the epidermis or dermis by the melanocytes. Typically, epidermal lesions will show a dark-brown, brown or beige color, whereas dermal hypermelanosis tends to be blue-gray in color.3
Multiple endogenous or exogenous inflammatory conditions can result in PIH.3
Generally, any inflammation or lesion on the skin can result in pigmentation (hyper/hypopigmentation), and PIH can be seen in many skin conditions, such as acne, eczema and contact dermatitis.4
At least two processes are involved in hyperpigmentation after cutaneous inflammation resulting in epidermal or dermal melanosis.5
The first one is pigmentary incontinence that follows destruction of the basal layer of the skin. The consequence of this process is the buildup of melanophages in the upper dermis. The macrophage can phagocytose the degenerated basal keratinocyte and the melanocytes, both containing great amounts of melanin, remaining in the upper dermis for some time.
The other process involves the epidermal inflammatory response, resulting in oxidation of the arachidonic acid into prostaglandins and leukotrienes.
These mediators stimulate epidermal melanocytes, that lead to increased melanin production and pigment transfer to the surrounding keratinocytes.
In other words, the epidermal hypermelanosis results from excessive stimulation and subsequent transfer to the melanin granules.5
Although its pathophysiology is still unknown, PIH can be explained by the regulation of skin pigmentation, parallel to the transfer between keratinocytes and melanocytes. There is evidence of the role of the interactions between epithelial and mesenchymal cells through the release of fibroblast growth factors. Among them, the keratinocyte growth factor (KGF), alone or in combination with interleukin-1a, induces melanin deposition in vitro and hyperpigmented lesions in vivo. Besides, moderate increase in KGF and upregulation of its receptors were observed in solar lentigo lesions, suggesting the participation of this growth factor in the appearance of hypepigmented patches.4
Some studies have quantified changes in the number of melanocytes associated with PIH secondary to exogenous causes, with findings of increased melanocyte count.
Changes in melanocyte density and their features are also seen secondary to inflammation; besides, an increase in dermal melanocytes after cutaneous exposure to certain agents was observed, as well as melanocyte increase, that vary according to the agent.
One can say that there is a correlation between the degree of hyperpigmentation and the intensity and duration of the exposure to PIH causal factors.6
Even though it does not cause any systemic problems, PIH can have a negative impact in the patient’s quality of life and lead to serious psychological consequences, explaining why patients seek treatment for the patches.1,3
PIH treatment must be commenced early to help speed its resolution, and should begin with the precipitating inflammatory condition. First line therapy usually consists of the use of topical bleaching agents, including use of sunscreens and topical tyrosinase inhibitors, such as hydroquinone, azelaic and kojic, acids, and arbutin. Other bleaching agents include retinoids, mequinol, ascorbic acid, niacinamide, N-acetylglucosamine and soy in emerging therapies. Topical therapy is usually effective for the treatment of epidermal post-inflammatory hyperpigmentation; however, some procedures, such as laser therapy and chemical peels, can help treat refractory hyperpigmentation. It is worth highlighting that it is important to be careful with more aggressive skin treatments, in order to avoid irritation and worsening of the PIH.1
We must point out that the treatment for PIH is many times difficult and lengthy.2
Some studies suggest that the lesions that are not amenable to medical or surgical therapy can somewhat improve with cosmetic camouflage,3 what we, the authors, believe that, in real life, can be very frustrating for the physician and the patient.
In the most recent years, percutaneous collagen induction technique started to be described as a therapeutic option in the treatment of hyperpigmented skin, but its use is usually associated with the loss of integrity of the stratum corneum, aiming at facilitating the transport of transdermal drugs. The microneedles, measuring from a few dozens to a few hundreds of microns, usually in an array, help the so-called drug delivery.7,8
In the percutaneous collagen induction technique, multiple perforations are made in the epidermis without destroying it, stimulating the collagen and thickening the skin.9
The use of needles for collagen stimulation was described in 1995 when Orentreich and Orentreich reported the method known as subcision for the treatment of scars.10
In 1997, Camirand and Doucet wrote about the use of a tattoo pistol without pigment to stimulate regeneration of the skin, whereby there would be replacement of the subdermal collagen by new collagen fibers and elastin after rupture of the damaged subdermal collagen.10
Based on these principles, the therapy of percutaneous collagen induction was developed in 2006.10
The device used for the procedure is a roller covered with fine needles in which, according to the manufacturer, there is variable amount and length of needles, from 0.25 to 3mm with approximately 0.1mm diameter.10
Because it is a procedure that opens channels between epidermal keratinocytes, topical agents can be used to enhance treatment results.9,11,12
A healing inflammatory process is triggered by the lesion caused by the needles, which has three phases: injury, healing and maturation.
In the injury phase, there is platelet and neutrophil release, that will be responsible for the release of growth factors that will act on keratinocytes and fibroblasts.
In the healing phase, neutrophils are replaced by monocytes and angiogenesis, epithelization and fibroblast proliferation occur, followed by collagen type III, elastin, glycosaminoglycan and proteoglycan production. In parallel, fibroblast growth factor is secreted by monocytes. The fibronectin matrix is formed approximately five days after injury, allowing the deposit of collagen below the basal layer of the epidermis.
In the maturation phase, collagen type III, that is predominant in the initial phase of the healing process, is slowly replaced by collagen type I, more long-lasting.11,12
This technique was recently described not to promote collagen improvement, but to treat facial melasma unresponsive to conventional treatment.13 In this study, the procedure was done without using the drug delivery technique, that is, without using topical agents during the procedure, yielding satisfactory bleaching results in 100% of patients.
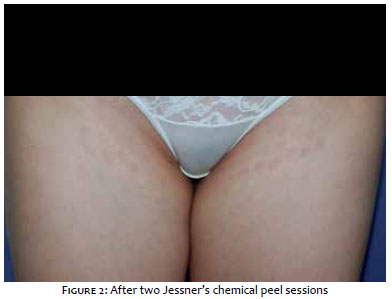
Female patient, 30 years old, complained of hyperchromic round patches bilaterally on the groins, after burn with Alexandrite laser hair removal done 20 months back (Figure 1). Topical products were applied, such as hydroquinone and triple combination for prolonged time, with no response. A chemical peel session using Jessner’s solution was initially performed, with mild bleaching of the inguinal patches, followed by two more similar treatments, with no clinical response (Figure 2). One year after failing the previous treatments for PIH, the percutaneous collagen induction technique was performed, using the Genosys device (Genosys Brazil. PLK Log. Health/Medical/Pharmaceuticals) with 0.5mm length needles.
The procedure was performed under topical anesthesia, with 4% lidocaine (Dermomax, Ferndale Industries Inc., USA — Biosintética Farmacêutica, Aché Laboratórios Farmacêuticos).
After disinfection with 2% chlorhexidine in aqueous solution, back and forth movements were performed with moderate pressure on the affected area, with approximately 10 passes in the same direction and at least 4 overlaps until pin-point bleeding was obtained. The area was cleaned with saline after the treatment and no substance was applied aiming at drug delivery. Dressings were applied without removing the blood from the area.
The patient was advised to use fusidic acid and mometasone in the area once daily for three days, and skin regenerator twice daily until complete healing of the skin injury caused.
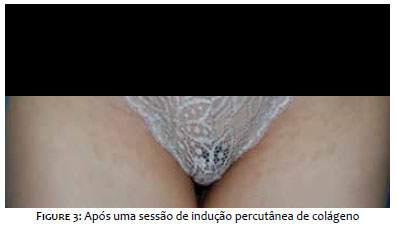
The patient was advised to restart using topical bleaching agents on the area approximately one week after the procedure; 20% azelaic acid in the morning and 4% hydroquinone cream at night. The patient was reassessed two months after the procedure, when a significant bleaching of the lesions was observed (Figure 3).
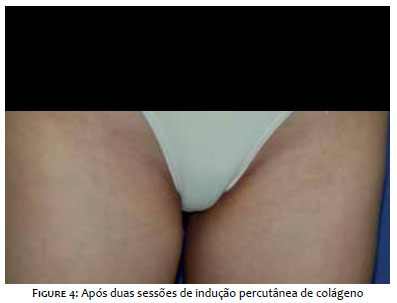
Although she declared to be very satisfied with the treatment, she still had some patches; thus, a new treatment of percutaneous collagen induction, identical to the first one, was performed after three months, with almost complete resolution of the patches in 45 days (Figure 4).
Post-inflammatory hyperpigmentation is a common consequence of inflammatory dermatoses and it can be caused by any skin inflammation. Even though its pathogenesis has not yet been elucidated, PIH probably occurs due to an increase of melanin production or deposition in the epidermis and/or dermis by melanocytes, that are the result of excessive stimulation and subsequent transfer to melanin granules.3
Early treatment is recommended for PIH, in order to speed its resolution, and it should start with management of the causative inflammatory condition. Usually, first line therapy consists on the use of topical bleaching agents, including sunscreens and topical tyrosinase inhibitors, such as hydroquinone, azelaic and kojic acids, and arbutin. Topical therapy is usually effective for the treatment of epidermal post-inflammatory hyperpigmentation; however, some procedures such as laser therapy and chemical peels are also helpful in treating refractory hyperpigmentation. However, in performing these procedures, one must realize that more aggressive skin treatments can worsen PIH.1 It is not uncommon for conventional treatments to be ineffective and slow. In these cases, percutaneous collagen induction comes as a new therapeutic approach. Despite not knowing exactly how the microneedling acts in the reduction of hyperchromia, the effect can take place due to the opening of the skin channels, promoting elimination of the pigment and also due to the activation of growth factors that, as already mentioned, are involved in the process of PIH and can be modified by using this technique.11,12
The effect of microneedling used alone in the treatment of skin hyperpigmentation can be a promising therapy, although there is need for further studies to help clarify the mechanism of action and maybe even establish better treatment protocols to enhance the technique’s therapeutic effects.
Sandra Tagliolatto
Metaanalysis on the subject and data interpretation.
Nancy Vanessa Paranhos Mazon
Data collection, analysis and interpretation.
1. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20-31.
2. Cayce KA, McMichael AJ, Feldman SR. Hyperpigmentation: an overview o f the common afflictions. Dermatol Nurs. 2004;16(5):401-6
3. Callender VD1, St Surin-Lord S, Davis EC, Maclin M. Postinflammatory hyperpigmentation: etiologic and therapeutic considerations. Am J Clin Dermatol. 2011;12(2):87-99.
4. Cardinali G, Kovacs D, Picardo M. Mechanisms underlying post-inflammatory hyperpigmentation: lessons from solar lentigo. Ann Dermatol Venereol. 2012;139 Suppl 4:S148-52.
5. Lacz NL, Vafaie J, Kihiczak NI, Schwartz RA. Postinflammatory hyperpigmentation: a common but troubling condition. Int J Dermatol. 2004;43(5):362-5.
6. Postinflammatory hyperpigmentation secondary to external insult: an overview of the quantitative analysis of pigmentation. Cutan Ocul Toxicol. 2013;32(1):67-71.
7. Vandervoort J, Ludwig A. Microneedles for transdermal drug delivery: a minireview. Front Biosci. 2008;13:1711-5.
8. Bariya SH, Gohel MC, Mehta TA, Sharma OP. Microneedles: an emerging transdermal drug delivery system. J Pharm Pharmacol. 2012;64(1):11-29.
9. Aust MC, Fernandes D, Kolokythas P, Kaplan HM, Vogt PM. Percutaneous collagen induction therapy: an alternative treatment for scars, wrinkles, and skin laxity. Plast Reconstr Surg. 2008;121(4):1421-9.
10. Matos MCO. O uso do microagulhamento no tratamento estético de cicatriz de acne [internet]. Rio de Janeiro: IBMR Laureat International Universities. 2014 [cited 2016 Nov 11]. Available from: https://www.henriquecursos.com/site/docs/Marina-TCC-completo2.pdf.
11. Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009;34(8):874-9.
12. Lima EVA, Lima MA, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol 2013;5(2):1104.
13. Lima EA. Microagulhamento em melasma facial recalcitrante: uma série de 22 casos. An Bras Dermatol. 2015;90(6):917-9.
Study conducted at Dermoclinica – Dermatologia e Laser – Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}