


Tatiana Cristina Pedro Cordeiro de Andrade1; Tábata Yamasaki Martins1; Agnes Mayumi Nakano Oliveira1; Tatiane Meira Santiago1; Cleverson Teixeira Soares2; Sadamitsu Nakandakari3
Lichen planopilaris is a rare disorder that belongs to the primary scarring alopecia type. The present study describes the case of a female patient bearing desquamative erythematous plaques and follicular plugs bilaterally in the frontoparietal region, associated with positive pull test. The biopsy's result was consistent with lichen planopilaris and the patient was treated with prednisone associated with clobetasol, with regrowth of the hair in the affected area. The treatment of this pathology is a challenge due to the lack of data on efficacy of therapies and constant recurrence. The picture is irreversible if not treated early. This paper describes a classic case of a case of lichen planopilaris with good therapeutic response, highlighting the importance of early diagnosis, due to the fact that most cicatricial alopecias do not produce scarring in their initial stage and should for this reason be managed as an emergency in trichology.
Keywords: ALOPECIA; EARLY DIAGNOSIS; LICHEN PLANUS
Described by Pringle in 1985, lichen planopilaris (LPP) is a rare inflammatory disorder mediated by lymphocytes.1-3 It is classified as a primary lymphocytic cicatricial alopecia 1,3,4 – the same classification received by discoid erythematosus lupus (DEL), central centrifugal cicatricial alopecia, pseudopelade of Brocq (PBB) among others.1 The destruction of the hair follicle and replacement by fibrosis is a natural development in cicatricial alopecias.1,2
Lichen planopilaris has chronic course, unpredictable development and, probably, autoimmune pathogenesis, 2,3 with an unknown inflammatory process against an autoantigen.1 Drugs, infections, genetic factors and immunological abnormalities are described as possible triggering factors.1
The authors of the present paper describe a case with classic manifestations of LPP, highlighting the importance of early diagnosis.
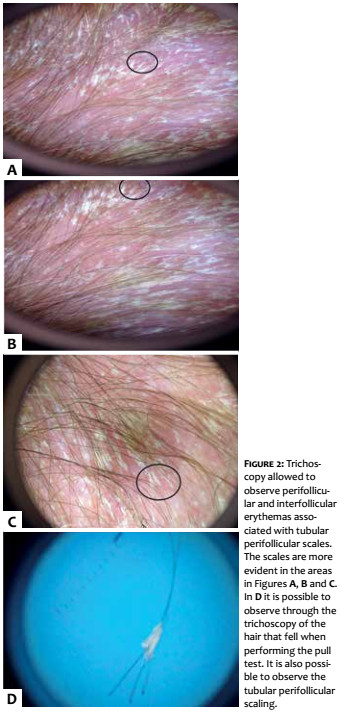
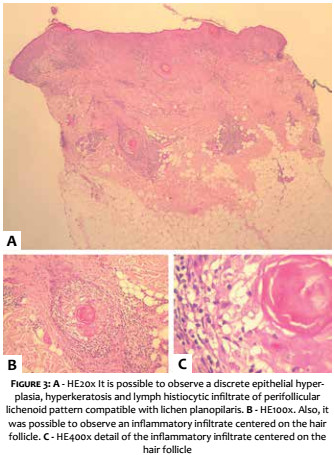
A 43-year-old female patient reported erythema and desquamation on the scalp with onset three months before, and intense pruritus associated with hair loss. She described previous use of clobetasol without improvement, denying comorbidities or use of any other medications. Dermatological examination showed erythematous-desquamative plaques with follicular plugs in the frontoparietal region bilaterally, (Figure 1) and positive pull test. Perifollicular and interfollicular erythema associated with tubular perifollicular scales were observed using trichoscopy (Figure 2). There were no nail or mucosal alterations at examination. The hypotheses of LPP and seborrheic dermatitis were raised. The lesion’s biopsy yielded an anatomopathological study compatible with LPP (Figure 3). General laboratory tests were requested, resulting in serologies with absence of alterations. The patient started to use 40 mg/day oral prednisone, associated with 0.05% topical clobetasol twice daily, in addition to hydration. The patient progressed with great clinical improvement 30 days after the beginning of the treatment (Figure 4). The weaning off of the corticoid was then started up until it could be suspended. The patient is being follow-up and experienced hair regrowth of the affected area, at present with four months of remission, after the total suspension of systemic and topical corticosteroids (Figure 5).
Lichen planopilaris (LPP) is considered a variant of lichen planus (LP) with follicular involvement1,2 and can be classified into 3 forms: classical, frontal fibrosing alopecia (FFA) and Graham-Little-Piccardi-Lasseur syndrome (GLPLS).1-3 These forms are differentiated by their distribution on the scalp and the patient’s age group, however they have overlapping characteristics, such as perifollicular inflammation, follicular hyperkeratosis, and cicatricial alopecia.2
In FFA, there is a characteristic involvement of the frontotemporal area of postmenopausal women with an association of eyebrow lesion in a percentage that ranges from 50 to 83% of the cases.1,3 In GLPLS, it is possible to observe the triad of cicatricial alopecia in the scalp preceding non-cicatricial alopecia in the axillae and groins, accompanied by generalized lichenoid follicular papules.1,3
The case reported is compatible with classical LPP, the most common variant affecting women,1-3 which frequently has its onset between the fifth and the seventh decades of life.2,3 The involvement of the scalp is irregular and occurs in the form of plaques, mainly in the apex1-3,5,6 and in the parietal region, as observed in the studied patient. Nevertheless, any region of the scalp can be affected.2,3
The first observed clinical signs are hyperkeratosis, follicular plugs and perifollicular erythema, 3,5,6 associated with a positive pull test.3 Trichoscopy of early stages evidence perifollicular and interfollicular erythema associated with tubular perifollicular scales. Many patients are misdiagnosed with seborrheic dermatitis at this stage,5 entailing a delay in the treatment and worsening of the prognosis. Atrophic scars replace the lesions later on, with definitive loss of follicular orifices, which makes the first irreversible.1-3,5,6
Complaints of pruritus and burning sensation are common,1,3,5,6 as well as the association with the skin, nail and mucosal LP lesions.1
It is estimated that at the time of diagnosis 17 to 28% of patients have evidence of LP 3 in other places of the body, meaning a complete physical examination is of paramount importance.1,3,5
Differential diagnosis is performed with seborrheic dermatitis, DEL and PBB.1 Biopsy of the lesions is necessary to differentiate them at the initial stage.3,6 Lichen planopilaris’ histopathology shows inflammation with epithelial hyperplasia, hyperkeratosis and degeneration of the basal layer.1-3 The peripheral lymphocytic infiltrate mainly affects the region that lays between the infundibulum and the isthmus, coursing with the destruction of the bulge.2,3,5,6 If LPP is not expanding with perifollicular inflammation and hyperkeratosis, it is impossible to differentiate it from PBB,1-3 which some authors do not consider a different entity, but the final stage of LPP.1,3
The treatment of LPP is a challenge because of the scarcity of data on the efficacy of therapies and inconsistent response to treatment, with constant recurrences.1,3,5,7,8 However, it becomes irreversible if not treated early, entailing that early diagnosis and treatment are mandatory.1,3,8 Hair re-growth in areas of existing alopecia is unlikely, meaning that the treatment’s objectives are to improve the patient’s symptoms and halt the progression of the disease.1-3,8
High potency topical corticosteroid 7,8 (level of evidence B) and / or intralesional triamcinolone acetonide (level of evidence D) are reported to be first-line therapies, with 66 to 70% and 40 to 50% remission rates, respectively.8 In the absence of response within four months, the methods should be alternated.3,8 The second-line treatment is systemic therapy, which is ideal for fast developing cases or those that are unresponsive to topical medicaments.3,8 First and second-line treatments are usually associated, as was the option in the reported case, which was characterized by the rapid progression and history of previous use of topical corticosteroids without improvement.
Among second-line options are oral corticosteroids, with 82% remission within one year.8 The recommended dose corresponds to 1mg / kg / day or 30-40mg / day prednisone for up to four months.1,3,8 As for antimalarials, Chiang et al. described improvement of 69% within six months, and of 83% within 12 months, based on the LPP’s activity score, with the use of hydroxychloroquine.5 Nonetheless, Donati et al. challenged the basically clinical nature of this improvement score and performed a photographic follow-up study with the use of hydroxychloroquine, however without obtaining good results.4 In refractory cases, oral cyclosporine is described as an option.1,3,8
Other therapeutic options are oral retinoids, tetracycline, thalidomide and mycophenolate mofetil, which have been reported in limited studies.3,8 The PPAR (peroxisome proliferator activated receptor-g) antagonist – pioglitazone – did not show lasting results.9
In cases with progression to cicatricial alopecia, hair transplantation is an option, however there is risk of recurrence of the disease in the transplanted areas. In this manner, it is suggested that a 2-year interval (without disease activity) be observed before it is indicated. In addition, the patient should be advised that the integration of the grafts might be reduced.2
The authors of the present paper have described a rare case of LPP with good therapeutic response, highlighting the importance of early diagnosis, since most cicatricial alopecias are of the non-cicatricial type in their initial phase and should therefore be managed as a trichology emergency.
1. Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53(1):1-37; quiz 38-40.
2. Crisóstomo MR, Crisóstomo MCC, Crisóstomo MGR, Gondim VJT, Crisóstomo MR, Benevides NA. Perda pilosa por líquen plano pilar após transplante capilar: relato de dois casos e revisão da literatura. An Bras Dermatol. 2011;86(2):359-62.
3. Assouly P, Reygagne P. Lichen planopilaris: update on diagnosis and treatment. Semin Cutan Med Surg. 2009;28(1):3-10.
4. Donati A, Assouly P, Matard B, Jouanique C, Reygagne P. Clinical and photographic assessment of lichen planopilaris treatment efficacy. J Am Acad Dermatol. 2011;64(3):597-8.
5. Chiang C, Sah D, Cho BK, Ochoa BE, Price VH. Hydroxychloroquine and lichen planopilaris: efficacy and introduction of Lichen Planopilaris Activity Index scoring system. J Am Acad Dermatol. 2010;62(3):387-92.
6. Meinhard J, Stroux A, Lünnemann L, Vogt A, Blume-Peytavi U. Lichen planopilaris: Epidemiology and prevalence of subtypes - a retrospective analysis in 104 patients. J Dtsch Dermatol Ges. 2014;12(3):229-35, 229-36.
7. Rácz E, Gho C, Moorman PW, Noordhoek Hegt V, Neumann HA. Treatment of frontal fibrosing alopecia and lichen planopilaris: a systematic review. J Eur Acad Dermatol Venereol. 2013;27(12):1461-70.
8. Harries MJ, Sinclair RD, Macdonald-Hull S, Whiting DA, Griffiths CE, Paus R. Management of primary cicatricial alopecias: options for treatment. Br J Dermatol. 2008;159(1):1-22.
9. Spring P, Spanou Z, de Viragh PA. Lichen planopilaris treated by the peroxisome proliferator activated receptor-γ agonist pioglitazone: lack of lasting improvement or cure in the majority of patients. J Am Acad Dermatol. 2013;69(5):830-2.
This study was carried out at the Istituto Lauro de Souza Lima (ILSL) Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}