


Alessandra Haddad1; Bogdana Victoria Kadunc2; Christine Guarnieri3; Juliana Sarubi Noviello4; Marisa Gonzaga da Cunha5; Meire Brasil Parada6
The concept of facial rejuvenation currently includes a three-dimensional perspective, which recognizes as signs of aging not only the loss of the skin's texture and the emergence of expression wrinkles, but also the volumetric losses secondary to bone remodeling and redistribution of facial fat. This article was aimed at reviewing the literature on poly-L-lactic acid for facial rejuvenation – including its indications, injection techniques, expected results and possible adverse effects – and offer practical guidelines, based on the authors' 12-year experience with the product.
Keywords: SKIN AGING; INJECTIONS; COLLAGEN
Up until the 1990s, the concept of facial rejuvenation was limited to a two-dimensional perspective, focused on reducing wrinkles and furrows. With the improvement of the facial anatomical knowledge, this concept was expanded and nowadays encompasses a three-dimensional perspective, which recognizes as signs of aging not only the loss of cutaneous texture and expression wrinkles, but also the volumetric losses secondary to bone remodeling and redistribution of facial fat.1 Thus, approaches that recognize the balance between the various facial structures, observing the individual patient’s gender, ethnicity and personal goals, allow for more natural and harmonious treatment outcomes. Several products and therapeutic strategies for facial rejuvenation are available today. Since its introduction a little over 15 years ago, poly-L-lactic acid has been used increasingly, which calls for the need to deepen the knowledge about its indications, injection techniques, expected results and possible adverse effects. The present article is aimed at presenting a literature review on poly-1-lactic acid for facial rejuvenation, while demonstrating the 12-year experience with the product in order to offer to the reader some guidelines on its use in the dermatological practice.
The knowledge of the correlation between the various skin layers, especially the dermis and hypodermis, and the changes they undergo during aging, is crucial for the understanding of the skin’s flaccidity, and the poly-L-lactic acid’s mechanism of action and its indications for rejuvenation.2,3 In chronological aging, the thickness of the dermis decreases as a result of biochemical and structural changes in collagen and elastic fibers as well as in the fundamental substance.4,5 There is a reduction in collagen synthesis and an increase in its degradation due to an increase in the levels of collagenase. The cutaneous content of collagen is reduced by about 1% per year throughout adult life, starting at around 40 years of age in women and a little later, around 50 years of age in men. The remaining collagen fibers are disorganized, more compact and fragmented. Elastic fibers decrease in number and diameter. The amount of mucopolysaccharides of the fundamental substance is reduced, in special hyaluronic acid. These changes negatively affect the skin’s turgor and collagen.6 The hypodermis thins due to aging, weight loss, or the practice of high-performance sports, where there is reduction in the body mass index. On palpation, these patients report feeling their skin is thin and lacking consistency, lacking “filling matter”. The changes that occur in these tissues can have great influence in the surrounding areas, leading to a cascade of secondary events. Although the main complaints that lead the patient to seek treatment are wrinkles and furrows, it is important to consider that these changes are a result of the slow and progressive alteration that occurs in all facial structures.7,8
Alterations of other structuresCraniofacial bone remodeling is an important contributor to facial aging.9 Shaw and Kahn found changes in the orbit’s contour (superomedial and inferolateral remodeling), glabella resorption, and piriform fossa widening, among other alterations.10 Regarding the muscles, it is unclear whether histologic aging occurs with age or whether they undergo physiological changes in response to the aging process of the underlying structures. Le Louarn et al. proposed that the deep fat pads beneath the facial mimetic muscles would be responsible for their curvilinear shapes and would contribute to the anterior projection characteristic of a young face.11 They also suggested that the volumetric loss beneath these muscles that occurs during aging, would lead to the shortening and flattening of these structures, thus contributing to the changes that characterize facial aging.11 The young face has a larger amount of fat distributed uniformly, allowing a smooth transition from one area to another and lending a more rounded, three-dimensional topography, delineated by a series of arcs and convexities.1 Thus, there is no clear distinction between areas such as the temples, eyelids and malar region, but only an uninterrupted reflection of light originating from a convex surface.3 In a series of innovative studies, Rohrich and Pessa demonstrated that facial fat is distributed into independent compartments with specific anatomical relationships among them, and that many of the retention ligaments that support facial subcutaneous tissue originate within the septal walls located between these compartments.12 Since deep fat is compartmentalized, the loss of volume in deep compartments would lead to predictable changes in facial topography.
Below is a review of the literature, based on a survey performed on the PubMed database. The authors of the present article searched all publications involving poly-1-lactic acid, selecting for reading and discussion those considered more relevant for the purpose of preparing a synthesis of the current knowledge about the product and its use in facial rejuvenation.
HistoryPoly-1-lactic acid was approved in Europe as a cutaneous filler in 1999 under the trade name New-Fill® (Biotech Industry SA).8 In 2004, it was approved by the USA Food and Drug Administration for the treatment of HIV-associated lipoatrophy, under the trade name Sculptra® (Dermik Laboratories, Sanofi Aventis, USA). In 2009, the indication was expanded to aesthetic treatments in immunocompetent patients.13 By 2006, more than 150,000 patients had been treated with poly-L-lactic acid in more than 30 countries.14 The product has been available in Brazil for roughly 12 years. In 2006, Danny Vleggaar reported his experience in treating more than 2,000 patients.15 Since then, many studies have been published attesting the safety, efficacy and durability of the outcomes obtained with poly-1-lactic acid.16
Physical and chemical propertiesPoly-1-lactic acid – the crystalline form of polylactic acid – is an injectable synthetic polymer of the alpha-hydroxy acids family, of amphiphilic, biocompatible and biodegradable nature, with the properties of self-organization and formation of colloidal micelles in aqueous medium. The polymer has been used for many years in absorbable suture yarns and nanoparticles for drug release control.17-19 The product is made available in the form of a lyophilized powder in a sterile vial containing non-pyrogenic mannitol (which improves the lyophilization of the particles), croscarmellose (an emulsifying agent that maintains particle distribution after reconstitution), and microparticles of poly-1-lactic acid measuring 40 to 63 micrometers in diameter.14 The particles’ size is large enough to prevent phagocytosis by macrophages or passage through the capillary walls, but also small enough to allow their injection using 26G needles.19
Mechanism of actionPoly-1-lactic acid is a biostimulator of collagen. Its clinical effects are due to the stimulation of a desired controlled inflammatory response, which leads to the slow degradation of the material and culminates with the deposition of collagen in the tissue.17 Once injected into the skin, local subclinical inflammatory response occurs, with the recruitment of monocytes, macrophages and fibroblasts. One capsule is formed around each microsphere individually. As poly-1-lactic acid is metabolized, the increased fibroblast collagen deposition remains, with resulting increase in dermal thickness.16,20 Fibroplasia therefore determines aesthetic results, however there is no evidence of residual fibrosis.16,17,21 Type I collagen production begins about 10 days after the application and continues for a period ranging from 8 to 24 months, while the product is degraded and the subclinical inflammatory response fades.22,23
Poly-1-lactic acid is degraded by hydrolysis, followed by the lactic acid’s oxidation process, which yields pyruvic acid. The release of CO2 occurs in the presence of acetyl-coenzyme A and, consequently, decomposition into citrate, which is incorporated into the Krebs cycle and results in the formation of CO2 and water, which can be eliminated through urine, feces and breathing. No significant amount of degradation residues is found in vital organs, and the product is completely eliminated in roughly 18 months.17,24
Animal studies have demonstrated that the implantation of solid particles of poly-1-lactic acid produces a cascade of events that results in the formation of new tissue.21,25 After the injection of reconstituted poly-1-lactic acid in the volar portion of the forearm, Lemperle et al. observed cellular response involving macrophages, lymphocytes and giant cells, similar to that observed in mice.26
Goldberg et al. investigated the human tissue response to injectable poly-L-lactic acid through the evaluation of collagen formation and inflammatory reaction in 14 volunteers. Three sessions of poly-1-lactic acid injection were performed in the retroauricular region, with an interval of four weeks. Skin biopsies were obtained at the baseline and at 3, 6 and 12 months after the first injection allowing the qualitative and quantitative analysis of collagen type I and III levels. In addition, measurements aimed at evaluating inflammatory responses were also taken at the experimental timepoints. The mean level of type I collagen increased significantly at 6 months as compared to the baseline. Histological assessment of the inflammation suggested that none of the volunteers had moderate or severe inflammation in the 3, 6 and 12-month analyzes.27
Clinical implications of the mechanism of actionThe mechanism of action of poly-1-lactic acid has important practical implications, including the application technique, optimization of outcomes and minimization of the product’s adverse effects.23 The technical differences between its use as a biostimulator and as facial cutaneous fillers are small, nevertheless crucial for the safety and success in results.14,16,20,21 After the application of poly-1-lactic acid, the injected volume promotes a readily observable change that remains for 2 to 3 days up until the diluent is completely absorbed, which allows the prior evaluation of future results.23 The poly-L-lactic acid’s biostimulatory mechanism allows the correction of facial furrows and wrinkles through the production of collagen, with a gradual increase in tissue volume.14,16,17 As outcomes may not be clearly visible for weeks after the application, it is important to await for the biological response that occurs between the applications. Also, additional treatments should be performed at intervals of at least 4 weeks, so that overcorrection is avoided.22 The response time and correction degree depend primarily on each patient’s characteristics, varying according to the age, gender, skin quality, phototype and eating habits. Each treatment with poly-1-lactic acid will lead to the formation of collagen, whose magnitude will also depend on the concentration and volume used, which should be individualized. Subsequent injections promote continuous stimulation of the tissue response, with deposition of new extracellular matrix and collagen, resulting in volume restoration and facial contour improvement. A study using cutaneous ultrasonography demonstrated a 4-6mm increase in the dermal thickness of the nasolabial and mandibular regions after bilateral injections of poly-1-lactic acid in HIV patients who had lipoatrophy caused by antiretroviral treatment.28 In addition, it was shown that the results remained for 2 years or longer.17,20 An ultrasound study measured the thickness of the dermis in 33 patients with HIV-associated lipoatrophy, and treatment with 4 sessions of poly-L-lactic acid led to an increase of 151% in thickness at 12 months, and of 196% at 24 months, confirming that the effect of neocollagenesis continues many months after the injection of the product.29
Clinical efficacy summaryAfter having its efficacy and safety proven in patients with HIV infection 28,30-32 even in the long-term,33,34 poly-L-lactic acid was subjected to randomized studies in immunocompetent patients. Poly-1-lactic acid was more effective than human collagen for the treatment of nasolabial sulcus in a randomized, multicenter, blinded evaluation,35 also leading to a higher overall satisfaction rate among patients.36 The overall improvement was of 100% three weeks after the third treatment session, remaining above 85% 25 months after the first injection of poly-1-lactic acid. These results led to product approval in the US and in several other countries. Likewise, the product was evaluated in a South Korean randomized study, having been considered not inferior to hyaluronic acid in the treatment of nasolabial folds of moderate to severe intensity.37 The most encompassing study was conducted in Europe involving 2,131 patients and 7,185 treatment sessions with poly-1-lactic acid, with 95% of patients satisfied with their aesthetic results.15 In addition to randomized studies, several single arm studies have been reported in the literature and commented on review articles and consensus panels about the facial and extrafacial use of poly-1-lactic acid.2,38-40
Poly-1-lactic acid is indicated for the improvement of sagging skin caused by aging, volumetric correction of depressed areas such as furrows, wrinkles, cutaneous depressions, atrophic scars and alterations resulting from lipoatrophy or bone remodeling of the treated area. In practice, this implies improving the quality and stiffening of the skin (for example, in acne scars), improving sagging and facial contour, leading to overall facial rejuvenation. Due to the fact that poly-L-lactic acid is used to treat changes caused by volumetric loss secondary to bone resorption, lipoatrophy and skin aging, it is currently recommended that the product be applied in different planes, such as the supraperiosteal, subcutaneous and subdermal planes. It is worth noting that the application is not performed directly on wrinkles, lines and furrows (two-dimensional application), but rather on flaccid and atrophic facial areas (three-dimensional application), aimed at treating the underlying loss of volume.
In the experience of the authors of the present article, this approach is capable of yielding the harmonic and natural outcomes desired by many patients. Poly-1-lactic acid should be avoided in dynamic and sphincteric areas of the face, such as the lips and the periorbital region, since repetitive movement may lead to accumulation of the product and subsequent emergence of nodules, sometimes with delayed resolution.41
In addition to indications for facial treatment, poly-1-lactic acid can be used in other body sites, such as the medial face of the arms, neck, chest region, abdomen and buttocks.39,42-46 Although the published experience with its extrafacial use is limited, preliminary data and clinical experience suggest that this product is a versatile option to treat sagging skin, loss of volume and contour in many body areas.39,47 In addition, there are descriptions in the literature of applications in cases of postoperative tissue loss 48 and nipple reconstruction after surgery for breast cancer.49 It is worth noting that in some body regions, such as the neck and pectoral region, the reduction of skin thickness due to loss of elastin and collagen is more relevant than the loss of volume seen on the face and hands. Thus, the aesthetic enhancement of these regions is more focused on the improvement of the skin’s quality than on the loss of volume.
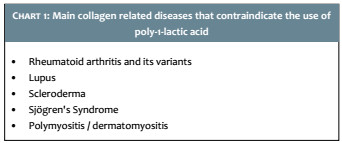
Poly-1-lactic acid is contraindicated in cases of infection or local inflammatory process, active autoimmune diseases, collagen diseases (Chart 1) and pregnancy, presence of definitive cutaneous fillers, or when there is history of keloids or hypertrophic scars. In addition, the product should not be used in people who are hypersensitive to any of its components.
Based on the fact that two different faces do not age identically, there is no single algorithm to follow.8 A younger patient often needs less product and fewer treatment sessions than an elderly patient.
Another relevant point is that treatments for rejuvenation in general should be performed cautiously, for some adverse effects can produce impacts both for the patient and physician. Cautiousness begins by obtaining a detailed anamnesis of medications in use – especially anticoagulants – as well as on the history of recurrent herpes simplex, inflammatory processes (for example, upper airways, sinus, dental or any structure located close to the area to be treated) and autoimmune diseases, including collagen related conditions (Chart 1). It is crucial to question whether the patient has already undergone some type of filling procedure and whether there has been any reaction to the filling substance previously used.
Evaluation of the faceFacial analysis is a process of observation and palpation that allows the determination of the nature and extent of facial structural changes. The treatment depends on the extent of the changes observed in each structural layer and the similarity of these changes between the layers. For example, a young patient with lipoatrophy due to the use of antiretrovirals only needs volumization of atrophic adipose fat pads. Most patients, however, tend to lose volume in all structural layers, implying that the face should be treated entirely, in a way that the treatment leads to more satisfactory results and outcomes are closer to the natural one. Therefore it is worthwhile to initially assess the integrity of each tissue: skin, fat, muscle and bone. Next, it is important to estimate the role of each tissue in the changes in shape, proportions and topography observed (the contribution of each structural layer to the facial appearance can easily be observed in patients with congenital facial asymmetry). The analysis of light and shadow regions evidences areas of prominence and depression (convexities and concavities) that contribute to the alterations – sometimes subtle – in the facial shape and topography. Palpation of shadow areas may reveal areas of atrophy. The evaluation of the orbits’ shapes, the bone support beneath the frontal region and the nose, and the proportions of the different areas of the face, yields information that goes beyond the “lines and folds”, assisting in obtaining a global picture of the structural changes in the face and of the interdependence between them.
The face should be observed in a three-dimensional way, so that it can be assessed whether the correction of one area can have an impact on another.
Pre-treatment guidelinesPhotographs of individuals in different decades of life arranged in chronological progression are often used to illustrate the depth of malar and mandibular atrophy, nasolabial folds, and marionette lines. However, it is possible to observe that changes in younger patients are not linked to the loss of facial volume, but to changes in the skin’s texture. In this manner, before planning a rejuvenation treatment, it is necessary to assess the patient’s face, make her or him aware of how the signs of aging can be modified by the available treatment options, and address additional concerns. The physician and patient must come to a common agreement on a realistic and comprehensive facial rejuvenation plan aiming at preserving facial balance. For example, patients with very marked aging or lipoatrophy should be made aware that their treatment might require a substantial amount of the product so that a desirable outcome is achieved.
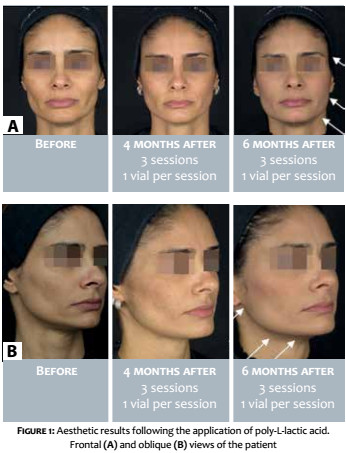
Advising the patient on the product’s mechanism of action facilitates the understanding of the need for a time interval for the results to become visible (some improvement can already be seen in most patients after the second treatment session) and on the need to undergo at least 3 applications with monthly intervals. Regarding the result’s duration, it is important to clarify that it may vary depending on the products used, the procedures performed, the patient’s general health and lifestyle.47 Figure 1 illustrates the clinical results obtained after the treatment of a patient with 3 sessions of Sculptra, 1 bottle per session.
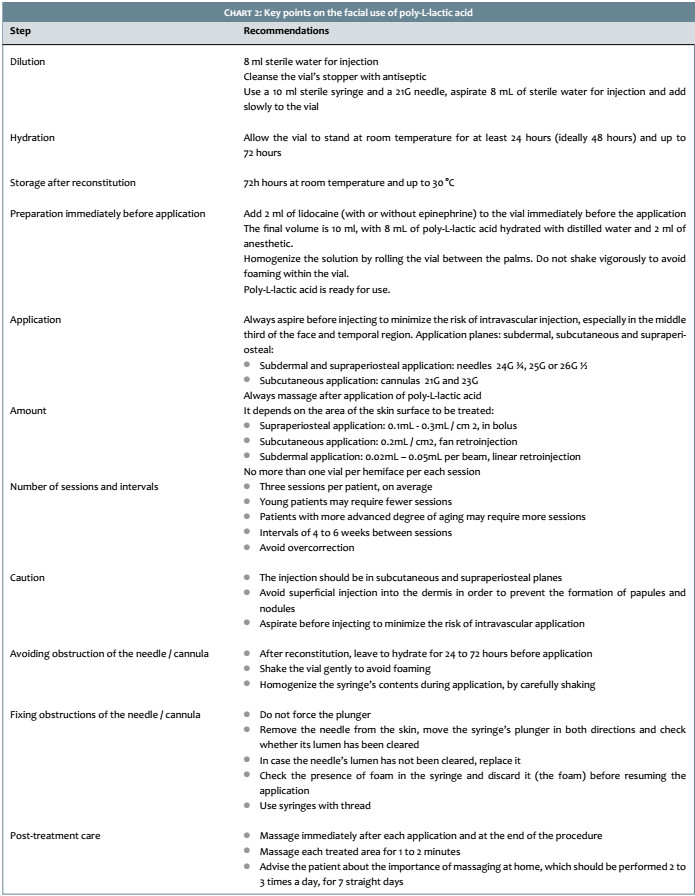
The appropriate technique for the preparation and application of poly-1-lactic acid is critical for the optimization of results. This includes the correct reconstitution and hydration of the product, application in the specific areas under local anesthesia, and massaging of the entire injected area after the procedure, ensuring the appropriate dispersion of the product.2,14,17,39,50-52 Chart 2 summarizes the key points in the process.
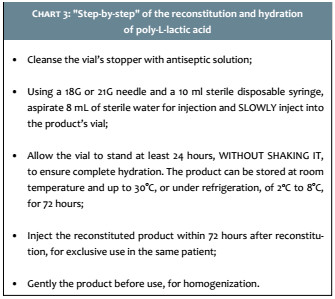
Reconstitution and hydrationThe vial’s contents should be reconstituted with 8 ml of sterile water for injections. The vial should not be shaken immediately after reconstitution so as to avoid the deposition of the still unhydrated particles in the vial’s wall. After reconstitution, the product should be allowed to stand for 24 to 72 hours prior to application. Storage of the product should preferably be done at room temperature up to 30 °C or under refrigeration, at 2 ºC to 8 °C, for up to 72 hours. The longer the resting time, the greater the hydration and, therefore, the easier it is to perform applications without obstruction of the needle. Immediately prior to use, the product should be gently shaken for better homogenization. Chart 3 shows a “step by step” description of this process.
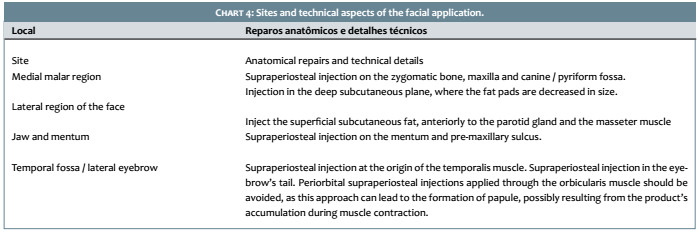
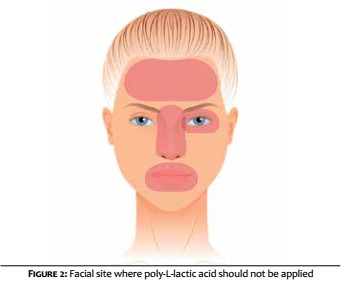
Application sitesThe selection of dynamically stable sites of application, with sufficient dermal thickness to allow appropriate depth of injection may assist in obtaining more favorable results. Chart 4 shows a summary of the anatomical location of the applications, while Figure 2 shows the locations where the product should not be applied. In the upper third of the face, poly-1-lactic acid should not be applied into the frontal and periorbital regions, for the musculature is hyperdynamic in these sites.39 In the temporal fossa, there should be attention with the superficial temporal artery, which is at the level of the temporal fascia. The application in this area should preferably be carried out supraperiosteally – since it is a more secure plane – in 0.3 ml boli.16 The middle third of the face is a common area of projection and volume loss. The projection of the face is mainly due to the bone support of the maxilla and the zygomatic arch. In aging, the resorption of these bone structures can be corrected with the application of poly-1-lactic acid in the supraperiosteal plane. It can be performed with 1 to 4 boli, as necessary, observing the distance of 1cm between them.16 The reabsorption of the pyriform fossa during aging results in the accentuation of the nasolabial sulcus, an increase in the distance between the columella and the upper lip, and the fall of the nasal tip. The restoration of this support is implemented with the application of poly-L-lactic acid in boli (0.3 to 0.5 ml / bolus) in the supraperiosteal plane, which is the safest for the pyriform fossa, given that the angular artery becomes more superficial in this region. The superficial fat compartments of the middle third of the face are the nasolabial fat pad and 3 distinct compartments of malar fat: medial malar fat pad, central malar fat pad, and temporolateral fat pad. Submalar fat atrophy is treated with applications in the subcutaneous plane using a cannula, with the fan retroinjection technique (0.2ml / cm2 or 0.2ml per retroinjection). The temporolateral fat pad connects the temporal fat to the cervical fat, laying superficially to the parotid gland.12 The loss of volume in this area creates concavities in the temporal and preauricular regions, increasing the demarcation of the zygomatic arch. The restoration of the lateral contour of the face is achieved by the application of the poly-1-lactic acid along the temporolateral fat pad. In the preauricular region, which extends from the angle of the mandible to the zygomatic arch, the application is preferably performed with a cannula in the superficial subcutaneous plane, anteriorly to the parotid gland and to the masseter muscle, using the fan retroinjection technique.16 Application in appropriate anatomical regions of the lower third of the face restores the contour of the chin and mandible, which undergo remodeling during aging. The irregularities of the lower face’s contour can be treated by supraperiosteal bolus applications (0.1 to 0.3 ml / cm2) along the chin’s border aimed at promoting the increase of its anterior projection; in the region lateral to the mentum (prejowl sulcus) and along the jaw’s body and angle, aimed at restoring the mandible support and redefine the facial contour. For the treatment of flaccidity in the lateral region of the face, resulting from dermal atrophy due to degeneration of collagen and elastic fibers, it is recommended to apply poly-L-lactic acid using the linear retroinjection technique with a needle in the subdermal plane, with a layout of several parallel beams (0.02 to 0.05 ml / beam). As a result, a traction vector is created by neocollagenesis, contributing to the lifting effect on the lateral region of the face. Applications should not be performed in the perioral region, as this area has hyperdynamic muscles.39
Preparation and anesthesiaPhotographic documentation is very important due to the fact that the injection of poly-L-lactic acid is a serial procedure, with gradual emergence of results over the months.53 The patient should be photographed in 5 positions (frontal, right and left diagonals, and right and left profiles). The areas to be treated should be marked with the patient seated. It is recommended that topical anesthetic be applied 30-60 minutes before the procedure, with some authors adding the anesthetic to the solution immediately before the application.53 The authors of the present study recommend 2ml of 2% lidocaine, totaling a volume of 10ml. Some authors recommend the infraorbital and mental nerves blocks. Still others apply ice before and after the injection of poly-L-lactic acid to decrease pain, stimulate vasoconstriction, and reduce the formation of echymoses.52 Skin antisepsis should be performed with 2% alcoholic chlorhexidine in order to avoid infectious complications in the post-procedure.
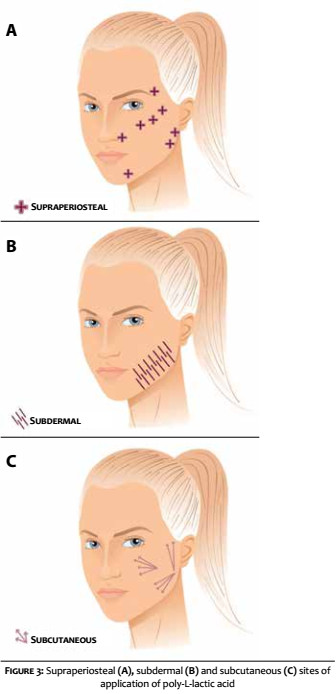
Application techniqueFigure 3 shows the sites for supraperiosteal, subdermal and subcutaneous application of poly-1-lactic acid. The product should be injected using 1ml or 3ml syringes and needles and/ or cannulas according to the application plan. 24G, 25G or 26G needles and/or 21G, 22G or 23G cannulas can be used. Aiming at minimizing the risk of needle obstruction, the solution should desirably be at room temperature at the time of application.
Poly-1-lactic acid should be injected into the supraperiosteal plane in areas with bone support (0.1 to 0.3 ml / cm2), or in the subcutaneous tissue where there is no bone structure (0.2 ml / cm2). Intradermal injections should be avoided due to the increased risk of papules and nodules. In the supraperiosteal plane, the deposit application technique is the most appropriate. The product is injected in the form of small boli using 24G 3/4 needles. The needle should be continuously inserted into the skin at a 90° angle up until the moment it touches the periosteum. Next, the reflux (aspirate) maneuver should be performed to avoid intravascular application, subsequently injecting a volume ranging from 0.1 to 0.3 ml / bolus. In the subcutaneous plane, it is recommended the use of 22G cannulas, with the previous preparation of a puncture with a larger gauge needle, using the fan retroinjection technique, which consists of a retrograde injection performed from a single entry point, covering more extensive areas – such as the preauricular and malar regions – slowly depositing 0.2ml/cm2 or 0.2ml/retroinjection. The injection should be halted when three-quarters of the cannula become visible, aiming at avoiding the superficialization of the product, which could lead to the emergence of papules and nodules. The application should be carried out in a continuous pace during the backwards movement of the needle in order to avoid the deposit of boli, which, according to the depth, can lead to the formation of papules or nodules. The syringe should be kept parallel to the surface of the skin during the application, which keeps the needle pervious during the procedure. The substance should be shaken intermittently in the syringe during the procedure.
Post-procedureMassaging the treated area is crucial in the application of poly-L-lactic acid, for it ensures uniform distribution of the substance and leads to better outcomes. It is recommended to use 2% degerming chlorhexidine, for its antiseptic effect and facilitation of the massage. The patient should be instructed to wash her or his hands and face, and massage the application area 2 to 3 times per day for five minutes, for 7 straight days, use emollient creams to minimize friction.
Frequency and number of applicationsFor a given patient, the surface area to be treated is the only factor determining the amount of poly-L-lactic acid to be applied during a session, with the volumetric correction obtained at the end of treatment being determined by the number of sessions.39 The amount of product used depends on the each patient’s need, according to the degree of aging. Younger patients or more volumetric faces usually need fewer sessions and a lower total amount of the product. In practice, for planning the number of vials needed for the full treatment (3 sessions), the ratio 1 vial / decade of life is used for 30 years old or older patients. Thus, a 30-year-old patient needs three bottles, a 40-year-old, four bottles, and so on. In general, most patients should receive the contents of 1 to 2 vials (half a bottle on each side) per session. It is important to ensure uniform distribution of the product in each treated region; the injection should not concentrate in any particular focus or vary according to specific aesthetic defects. Treatment may continue up until the patient is satisfied with the results, which usually occurs after 3 to 5 sessions. The rule “treat, wait and evaluate” should be used to guide the subsequent injections.38 The usual recommendation is to schedule a re-evaluation for a possible new treatment for between 4 and 6 weeks after the first application.52 Maintenance treatment is usually performed 1 year after the initial treatment. At these sessions, lesser amounts of poly-L-lactic acid, and fewer applications (often 1 or 2) are generally necessary.54
Cutaneous injection procedures often cause some discomfort, erythema, edema or hematoma, which are usually transient and resolve spontaneously. On the other hand, potentially more serious effects are uncommon. These are complications caused by the use of different products injected into the face, causing papules, non-inflammatory nodules and granulomas, infections and vascular phenomena, such as skin necrosis and even blindness. Although it has been used for decades in a generally safe manner, poly-L-lactic acid can cause the adverse effects described below.
Papules, nodules and granulomasPapules, nodules and granulomas are terms that have been used interchangeably in practice, however in fact they describe different clinical situations. Papules and nodules are non-inflammatory, and have good prognosis and easy resolution, while inflammatory nodules and granulomas can be chronic and difficult to resolve. Due to the acid-poly-L-lactic acid’s crystalloid microparticles, the most common adverse effect are papules and nodules caused by the accumulation of material, usually caused by inadequate reconstitution.55 Subcutaneous papules are invisible but palpable (<5mm), while non-inflammatory nodules are protruding. Both may develop several weeks after the injection of poly-L-lactic acid, being asymptomatic. Their frequency may be minimized if the recommended application technique is attentively observed (Chart 2). Just after the product was approved in Europe in 1999, application of poly-L-lactic acid was recommended following reconstitution to a volume ≤ 3ml, 2 hours before the injection.56 Sessions were performed with very short time intervals (7 to 10 days). In addition, the applications were very superficial and also carried out in hyperdynamic areas. As a result, the incidence of papules and nodules was very high, ranging from 10% to 44% in the literature reports.15,31,33,35,57 More recently, the frequency of these adverse effects decreased to around 1%, due to changes in the product’s reconstitution in greater volume of sterile water for injection, among other technical recommendations (Chart 2).2,41,57 Many papules or nodules are not visible, do not cause functional or aesthetic impact and can resolve spontaneously. In cases of visible or persistent lesions, vigorous massage, intralesional injection of corticosteroids or surgical excision may be options.38,58
Late granulomas are clinically characterized by inflammatory nodules that appear months or years after the injection, persisting and increasing over time.55,58 Although they have been initially attributed to hypersensitivity phenomena to the material, it is currently known that they may harbor chronic infections. This complication is rare (<0.1%) and seems to be systemic in nature, comprising an exaggerated response of the host to the material injected, infections caused by slow growth bacteria, and the formation of biofilms. Biofilms are sessile bacterial colonies where microorganisms are strongly adhered to a substrate comprised of exopolysaccharides extracellular matrix. This adherence hampers the penetration of antibiotics, explaining the long development of these lesions and the difficult treatment. The biofilm may exist in latent form for long periods and be triggered by trauma, handling and injections. Laboratory confirmation is considerably difficult and biopsies are generally necessary for correct histological identification and collection of material for the culture of bacteria, mycobacteria and fungi.59 In the absence of results, research with molecular techniques can be carried out. Treatment of late inflammatory nodules is designed to attempt to stop the increased secretion of interstitial substances and invasion of inflammatory cells in the lesion. This includes the use of corticosteroids, antibiotics (systemic and / or intralesional) and antimetabolites, such as 5-fluorouracil, which has activity against gram-negative bateria.39 Hyaluronidase can assist in disintegrating the biofilm’s matrix.
InfectionsThe risk of acute or late infections can be minimized using strict asepsis and antisepsis at the time of application (Chart 2). Acute infections are clinically characterized by inflammatory nodules in the first days after the procedure and are diagnosed via ultrasound, bacteriological examination and culture. Treatment should be conducted with systemic antibiotics and drainage of the material, in case there is fluctuation.
Vascular phenomenaCutaneous necrosis may be caused by intravascular injection, vasospasm or extrinsic compression caused by the injection of any product. Symptoms of the ischemia are pain, bleaching and reticulated erythema, accompanied by skin necrosis and ulceration on subsequent days.
Blindness has been described in cases of autologous fat, hyaluronic acid and collagen injections, being caused by the impairment of the central retinal and ophthalmic arteries. The material may be accidentally injected into a distal branch of the ophthalmic artery – such as the supratrochlear artery – retrogradely flowing via extraorbital peripheral branches, being propelled towards the main trunk of the ophthalmic artery, thus possibly causing blindness. The low viscosity of the poly-L-lactic acid solution allows aspiration to make sure that the needle is not within a vessel. Also, it prevents vascular compression in the region, which is an advantage regarding other more viscous materials.
The use of poly-L-lactic acid in combination with other facial rejuvenation procedures has found some supportive evidence in the literature, largely in studies conducted by the same authors.60 Fabi and Goldman reported their experience with 90 patients treated with intense pulsed light immediately before undergoing the application of the product diluted in 7ml bacteriostatic solution and 1ml lidocaine, between the years of 2003 and 2011. They observed that the combination is safe and effective, with absence of significant increase in complications as compared to the injection of poly-L-lactic acid alone. This combination can be used to treat photodamage and sagging skin at the same time. In another study performed by the same authors, they discussed aspects that should be questioned in the combination of techniques that affect the dermis: 1) Is there an increase in the complication rate?, 2) Is there denaturation or distortion of the implanted material if the second technique is superimposed?, 3) Does the new stimulus interrupt or modify the active dermal response? These issues are not yet fully understood. In these authors’ experience, the application of pulsed light followed by the application of micro focused ultrasound and poly-L-lactic acid seems safe when performed in this sequence. Finally, the group of authors proposed the use of micro focused ultrasound immediately before the application of poly-L-lactic acid, on the same day, aiming at treating multiple planes. These authors concluded that this combination provides a synergistic and effective approach for the treatment of multiple planes of the face, neck and chest. The combination of hyaluronic acid and poly-L-lactic acid is also possible in the same session if applied in different areas.
Despite the enormous range of injectable products for facial volumization, including hyaluronic acid in its different presentations, calcium hydroxyapatite and polymethylmethacrylate, poly-L-lactic acid is unique in its mechanism of action, which promotes local and gradual tissular reaction, resulting in neocollagenesis. The use of this collagen biostimulator employing current techniques, which consider changes in different facial structures due to the aging process, allows a more holistic approach to facial rejuvenation, leading to long lasting effects in the improvement of contours and facial sagging. It is worth noting that the final outcome of the treatment with poly-L-lactic acid depends on a careful facial assessment and appropriate treatment indication. It also depends on the use of the correct technique of preparation and application of the product and, last but not least, on the patients’ individual characteristics.
1. Donofrio LM. Fat distribution: a morphologic study of the aging face. Dermatol Surg. 2000;26(12):1107-12.
2. Bartus C, William Hanke C, Daro-Kaftan E. A decade of experience with injectable poly-L-lactic acid: a focus on safety. Dermatol Surg. 2013;39(5):698-705.
3. Coleman SR, Grover R. The anatomy of the aging face: volume loss and changes in 3-dimensional topography. Aesthet Surg J. 2006;26(1S):S4-9.
4. Quan T, Fisher GJ. Role of age-associated alterations of the dermal extracellular matrix microenvironment in human skin aging: A Mini-Review. Gerontology. 2015;61(5):427-34.
5. Fisher GJ, Varani J, Voorhees JJ. Looking older: fibroblast collapse and therapeutic implications. Arch Dermatol. 2008;144(5):666-72.
6. Yaar M, Gilchrest B. Aging of skin. In: Fitzpatrick's dermatology in general medicine. 7th ed. New York : McGraw-Hill Medical; 2008. p. 963-73.
7. Beer K. Dermal fillers and combinations of fillers for facial rejuvenation. Dermatol Clin. 2009;27(4):427-32.
8. Goldman MP. Cosmetic use of poly-L-lactic acid: my technique for success and minimizing complications. Dermatol Surg. 2011;37(5):688-93.
9. Sharabi SE, Hatef DA, Koshy JC, Hollier LH, Jr., Yaremchuk MJ. Mechanotransduction: the missing link in the facial aging puzzle? Aesthetic Plast Surg. 2010;34(5):603-11.
10. Shaw RB, Jr., Kahn DM. Aging of the midface bony elements: a three-dimensional computed tomographic study. Plast Reconstr Surg. 2007;119(2):675-81; discussion 82-3.
11. Le Louarn C, Buthiau D, Buis J. Structural aging: the facial recurve concept. Aesthetic Plast Surg. 2007;31(3):213-8.
12. Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119(7):2219-27; discussion 2228-31.
13. Bassichis B, Blick G, Conant M, Condoluci D, Echavez M, Eviatar J, et al. Injectable poly-L-lactic acid for human immunodeficiency virus-associated facial lipoatrophy: cumulative year 2 interim analysis of an open-label study (FACES). Dermatol Surg. 2012;38(7 Pt 2):1193-205.
14. Lam SM, Azizzadeh B, Graivier M. Injectable poly-L-lactic acid (Sculptra): technical considerations in soft-tissue contouring. Plast Reconstr Surg. 2006;118(3 Suppl):55S-63S.
15. Vleggaar D. Soft-tissue augmentation and the role of poly-L-lactic acid. Plast Reconstr Surg. 2006;118(3 Suppl):46S-54S.
16. Fitzgerald R, Vleggaar D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatol Ther. 2011;24(1):2-27.
17. Lacombe V. Sculptra: a stimulatory filler. Facial Plast Surg. 2009;25(2):95-9.
18. Hoffman AS. Hydrogels for biomedical applications. Adv Drug Deliv Rev. 2002;54(1):3-12.
19. Griffith LG. Polymeric biomaterials. Acta Materialia. 2000;48(1):263-77.
20. Schierle CF, Casas LA. Nonsurgical rejuvenation of the aging face with injectable poly-L-lactic acid for restoration of soft tissue volume. Aesthet Surg J. 2011;31(1):95-109.
21. Lowe NJ. Optimizing poly-L-lactic acid use. J Cosmet Laser Ther. 2008;10(1):43-6.
22. Bauer U, Graivier MH. Optimizing injectable poly-L-lactic acid administration for soft tissue augmentation: The rationale for three treatment sessions. Can J Plast Surg. 2011;19(3):e22-7.
23. Rhoda S, Narins MD. Minimizing adverse events associated with poly-l-lactic acid injection. Dermatol Surg. 2008;34 Suppl 1:S100-4.
24. Gupta AP, Kumar V. New emerging trends in synthetic biodegradable polymers - Polylactide: A critique. European Polymer Journal 2007;43(10):4053-74.
25. Hooper KA, Nickolas TL, Yurkow EJ, Kohn J, Laskin DL. Characterization of the inflammatory response to biomaterials using a rodent air pouch model. J Biomed Mater Res. 2000;50(3):365-74.
26. Lemperle G, Morhenn VB, Pestonjamasp V, Gallo RL. Migration studies and histology of injectable microspheres of different sizes in mice. Plast Reconstr Surg. 2004;113(5):1380-90.
27. Goldberg D, Guana A, Volk A, Daro-Kaftan E. Single-arm study for the characterization of human tissue response to injectable poly-L-lactic acid. Dermatol Surg. 2013;39(6):915-22.
28. Moyle GJ, Lysakova L, Brown S, Sibtain N, Healy J, Priest C, et al. A randomized open-label study of immediate versus delayed polylactic acid injections for the cosmetic management of facial lipoatrophy in persons with HIV infection. HIV Med. 2004;5(2):82-7.
29. Rendon MI. Long-term aesthetic outcomes with injectable poly-l-lactic acid: observations and practical recommendations based on clinical experience over 5 years. J Cosmet Dermatol. 2012;11(2):93-100.
30. Guaraldi G, Orlando G, De Fazio D, De Lorenzi I, Rottino A, De Santis G, et al. Comparison of three different interventions for the correction of HIV-associated facial lipoatrophy: a prospective study. Antivir Ther. 2005;10(6):753-9.
31. Carey DL, Baker D, Rogers GD, Petoumenos K, Chuah J, Easey N, et al. A randomized, multicenter, open-label study of poly-L-lactic acid for HIV-1 facial lipoatrophy. J Acquir Immune Defic Syndr. 2007;46(5):581-9.
32. Narciso P, Bucciardini R, Tozzi V, Bellagamba R, Ivanovic J, Giulianelli M, et al. Immediate versus delayed surgical intervention for reconstructive therapy of HIV-associated facial lipoatrophy: a randomized open-label study. AIDS Res Hum Retroviruses. 2009;25(10):979-87.
33. Moyle GJ, Brown S, Lysakova L, Barton SE. Long-term safety and efficacy of poly-L-lactic acid in the treatment of HIV-related facial lipoatrophy. HIV Med. 2006;7(3):181-5.
34. Carey D, Baker D, Petoumenos K, Chuah J, Rogers GD, Watson J, et al. Poly-l-lactic acid for HIV-1 facial lipoatrophy: 48-week follow-up. HIV Med. 2009;10(3):163-72.
35. Narins RS, Baumann L, Brandt FS, Fagien S, Glazer S, Lowe NJ, et al. A randomized study of the efficacy and safety of injectable poly-L-lactic acid versus human-based collagen implant in the treatment of nasolabial fold wrinkles. J Am Acad Dermatol. 2010;62(3):448-62.
36. Brown SA, Rohrich RJ, Baumann L, Brandt FS, Fagien S, Glazer S, et al. Subject global evaluation and subject satisfaction using injectable poly-L-lactic acid versus human collagen for the correction of nasolabial fold wrinkles. Plast Reconstr Surg. 2011;127(4):1684-92.
37. Hyun MY, Lee Y, No YA, Yoo KH, Kim MN, Hong CK, et al. Efficacy and safety of injection with poly-L-lactic acid compared with hyaluronic acid for correction of nasolabial fold: a randomized, evaluator-blinded, comparative study. Clin Exp Dermatol. 2015;40(2):129-35.
38. Alessio R, Rzany B, Eve L, Grangier Y, Herranz P, Olivier-Masveyraud F, et al. European expert recommendations on the use of injectable poly-L-lactic acid for facial rejuvenation. J Drugs Dermatol. 2014;13(9):1057-66.
39. Vleggaar D, Fitzgerald R, Lorenc ZP, Andrews JT, Butterwick K, Comstock J, et al. Consensus recommendations on the use of injectable poly-L-lactic acid for facial and nonfacial volumization. J Drugs Dermatol. 2014;13(4 Suppl):s44-51.
40. Kontis TC. Contemporary review of injectable facial fillers. JAMA Facial Plast Surg. 2013;15(1):58-64.
41. Palm MD, Woodhall KE, Butterwick KJ, Goldman MP. Cosmetic use of poly-l-lactic acid: a retrospective study of 130 patients. Dermatol Surg. 2010;36(2):161-70.
42. Butterwick KJ. Rejuvenation of the aging hand. Dermatol Clin. 2005;23(3):515-27, vii
43. Mazzuco R, Hexsel D. Poly-L-lactic acid for neck and chest rejuvenation. Dermatol Surg. 2009;35(8):1228-37.
44. Coimbra DD, Amorim AGF. Ácido Poli-L-láctico na região medial dos braços. Surg Cosmet Dermatol 2012;4(2):182-5.
45. Sadick NS, Arruda S. The Use of Poly-L-Lactic Acid in the Abdominal Area. Dermatol Surg. 2016;43(2):313-15.
46. Mazzuco R, Sadick NS. The Use of Poly-L-Lactic Acid in the Gluteal Area. Dermatol Surg. 2016;42(3):441-3
47. Werschler WP, Weinkle S. Longevity of effects of injectable products for soft-tissue augmentation. J Drugs Dermatol. 2005;4(1):20-7.
48. Ralston JP, Blume JE, Zeitouni NC. Treatment of postoperative soft tissue loss with injectable poly-L-lactic acid. J Drugs Dermatol. 2006;5(10):1000-1.
49. Dessy LA, Troccola A, Ranno RL, Maruccia M, Alfano C, Onesti MG. The use of poly-lactic acid to improve projection of reconstructed nipple. Breast. 2011;20(3):220-4.
50. Narins RS. Minimizing adverse events associated with poly-L-lactic acid injection. Dermatol Surg. 2008;34 Suppl 1:S100-4
51. Butterwick K, Lowe NJ. Injectable poly-L-lactic acid for cosmetic enhancement: learning from the European experience. J Am Acad Dermatol. 2009;61(2):281-93.
52. Sherman RN. Sculptra: the new three-dimensional filler. Clin Plast Surg. 2006;33(4):539-50.
53. Salles AG, Lotierzo PH, Gimenez R, Camargo CP, Ferreira MC. Evaluation of the poly-L-lactic acid implant for treatment of the nasolabial fold: 3-year follow-up evaluation. Aesthetic Plast Surg. 2008;32(5):753-6.
54. Fitzgerald R. Advanced techniques for Sculptra. J Drugs Dermatol. 2009;8(suppl 4):17-20.
55. Haneke E. Adverse effects of fillers and their histopathology. Facial Plast Surg. 2014;30(6):599-614.
56. Apikian M, Roberts S, Goodman GJ. Adverse reactions to polylactic acid injections in the periorbital area. J Cosmet Dermatol. 2007;6(2):95-101.
57. Rossner F, Rossner M, Hartmann V, Erdmann R, Wiest LG, Rzany B. Decrease of reported adverse events to injectable polylactic acid after recommending an increased dilution: 8-year results from the Injectable Filler Safety study. J Cosmet Dermatol. 2009;8(1):14-8.
58. Beer K, Avelar R. Relationship between delayed reactions to dermal fillers and biofilms: facts and considerations. Dermatol Surg. 2014;40(11):1175-9.
59. Parada MB, Michalany NS, Hassun KM, Bagatin E, Talarico S. A histologic study of adverse effects of different cosmetic skin fillers. Skinmed. 2005;4(6):345-9.
60. Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and decolletage. Plast Reconstr Surg. 2015;136(5 Suppl):180S-187S.
This study was carried out at the Universidade Federal de São Paulo – Escola Paulista de Medicina (Unifesp-EPM), São Paulo (SP) Brazil; Pontifícia Universidade Católica de Campinas (PUC-CAMP), Campinas (SP) Brazil; Fundação Hospitalar do Estado de Minas Gerais (Fhemig), Belo Horizonte (MG) Brazil; Faculdade de Medicina do ABC (FMABC), Santo André (SP) Brazil; Private practices in São Paulo (SP) and Belo Horizonte (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}