


Estevão José Muller Uliano1; Gustavo Palmeira Valter1; Daniel Ongoratto Barazzetti1; Jorge Bins Ely2; Vilberto Vieira3; Camila Bussolo Schmitt4
Introduction: The use of a median-frontal flap for nasal reconstruction was first described in 600 B.C., and it is still widely used for the reconstruction of nasal tumoral lesions.
Objective: To report the experience of a medical school's plastic surgery service in the use of this flap type.
Methods: A retrospective descriptive study was carried out with a series of 35 cases surgically treated from January 2005 to June 2015.
Results: The patients' mean age was 68.6 (± 10.8) years, with a predominance of the male gender (68.6%). The median-frontal flap was used for reconstruction after resection of tumors, with basal cell carcinoma being the most frequent.
Conclusions: The median-frontal flap is the ideal reconstructive choice for many patients, with good aesthetic and functional outcomes.
Keywords: SURGICAL FLAPS; RECONSTRUCTION; NOSE; NOSE NEOPLASMS
The history of nasal reconstruction has its roots in ancient times. Adultery was punished with the amputation of the nose in ancient India, with reports of reconstructive surgeries performed in the nasal region.1
The nose’s skin is one of the most common sites for skin cancer and one of the most complex anatomical regions for reconstruction.2 The first advances in the search for techniques capable of improving the outcomes of nasal flaps were accomplished between the years of 1874 and 1879 by Carpue et al., who proposed to fold the edges of frontal flaps in order to reduce the bloody area, thus decreasing infection, fibrosis and retraction, as well as leading to better aesthetic results.3,4 Today the paramedian frontal flap is a standard procedure in nasal reconstructive surgery, allowing the reconstruction of extensive nasal defects.
Skin tumors are the main indication for nasal reconstruction surgery nowadays.5 Basal cell carcinoma is the most common tumor in this region, followed by squamous cell carcinoma.1 The Brazilian southern city of Florianópolis has a high index of incidence of cutaneous tumors due to the fact that most of the population is of Caucasian origin and has the habit of exposure to the sun.
The present article is aimed at demonstrating the median-frontal flap’s versatility for extensive nasal reconstruction. The Plastic Surgery Department, University Hospital, Universidade Federal de Santa Catarina (HU-UFSC, Santa Catarina State, Brazil) aims at using this technique as a standard, which promotes training in the method and leads to positive results with fewer interventions.
A retrospective descriptive study was carried out with a case series, based on a review of medical records and an images database of patients bearers of tumors in the nose, who underwent surgery at the Plastic Surgery and Burns Department at the HU-UFSC, in the period spanning from January 2005 to June 2015.
The following variables were analyzed: age, gender, histological type, affected nasal subunits, postoperative complications, type of anesthesia, tumor recurrence and number of surgical interventions. The following nasal anatomical subunits quoted in the literature were considered:6 1) nasal root, 2) nasal dorsum, 3) lateral wall, 4) tip, 5) ala, 6) columella.
Statistical analysis was performed with the help of the SPSS (Statistical Package for Social Sciences) version 19.0 software. The continuous variables were represented by mean values and standard deviations, while categories, by absolute values and percentages. The Student’s t-test was used to compare mean val-ues. The significance level (alpha) was set at 5%.
The study strictly complied with the ethical principles set by the 2013 revision of the Declaration of Helsinki. The patients signed a term of consent allowing the use of their medical records and the publication of images.
The median-frontal flap is the gold standard for any nasal reconstruction due to the large amount of tissue it provides, with good color and texture resemblance regarding the nose’s skin. Surgery can be performed under sedation or preferably with general anesthesia. The primary defect should be evaluated before the execution of the median-frontal flap. Following the evaluation and marking, the patient is placed in dorsal decubitus and local injection of anesthetic and hemostatic solution is carried out. Next, the lesion’s resection is performed with safety margins.
The following technique was used for the execution of the median-frontal flap:
1. Maintenance of the axial direction whenever possible.
2. Use of a pedicle ipsilateral to the defect with a variable width of 1.3 to 1.5cm, located 2cm from the lateral of the midline.
3. The initial flap elevation is carried out distally. The upper third is detached only with skin and subcutaneous tissue. The dissection is deepened in the middle third of the frontal region, incorporating the muscle in the flap.
4. Subsequently, the dissection is performed subperiosteally 1cm above the eyebrow, continuing up until the orbits rhyme, along the configuration of the supratrochlear artery, as shown in figure 1A.
5. The medial rotation of the pedicle is carried out.
6. The insertion of the flap in the recipient area is performed by means of an absorbable suture along its entire border, aimed at reducing the risk of postoperative bleeding.
7. In case of bone and / or cartilage loss, the first option of donor areas are the septal and conchal cartilages.8 Primary suture is performed in the lower third of the frontal region, while in the upper two-thirds healing takes place by second intention.
9. Between 4 and 6 weeks later the section of the pedicle is performed with local anesthesia.
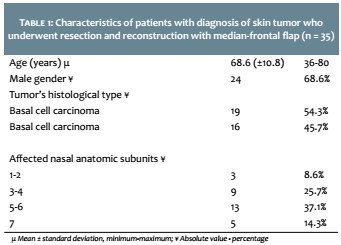
The HU-UFSC’s Plastic Surgery and Burns Department performed 35 surgeries of nasal reconstruction with median-frontal flap following resection of tumors during the evaluated period. Regarding the study sample, the mean age was 68.6 (± 10.8), ranging from 36 to 80 years. The male gender was the most prevalent, with 24 (68.6%) individuals. Regarding the histological type, basal cell carcinoma had predominance, with 19 (54.3%) cases, followed by squamous cell carcinoma, with 16 (45.7%) cases. The predominant nasal anatomic subunit was the “5-6”. Table 1 shows the characteristics of the patients included in the study.
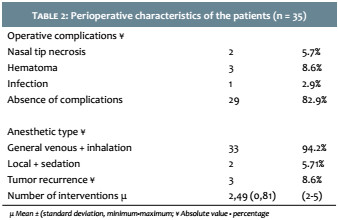
Regarding perioperative complications, the authors found a prevalence of 2 cases (5.7%) of nasal tip necrosis, 3 (8.6%) of hematomas and 1 (2.9%) of infection. Hematoma occurred in the first six hours, with all three cases undergoing re-intervention. One case had infection, treated with oral antibiotic therapy for 7 days. General anesthesia was the most used method, having been employed in 33 cases (94.2%). During the follow-up period, 3 (8.6%) patients had tumor recurrence. The mean number of interventions was 2.49 (SD = 0.81, min = 2, max = 5). Table 2 shows the patients’ perioperative characteristics.
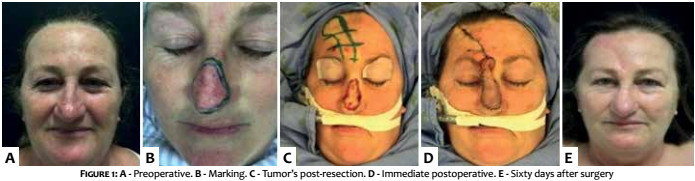
Figure 1A shows the patient in the preoperative period, Figure 1B shows the tumor resection marking on the nasal dorsum, and Figure 1C illustrates the transoperative period after the tumor’s resection with the marking of the median-frontal flap. Figure 1D shows the immediate postoperative and Figure 1E, the postoperative 60 days later.
The median-frontal flap is the gold standard for any nasal reconstruction given the amount of tissue it provides and the similarity of color and texture to those of the nose’s skin.7 Indications for nasal reconstruction arise from multifactorial cases. In the present study, this flap type was used after nasal tumor resection in 35 cases operated at the HU-UFSC’s Plastic Surgery and Burns Department.
Tumors – mainly basal cell carcinoma and epidermoid carcinoma – are the main surgical indication for nasal reconstruction.5 Basal cell carcinoma (BCC) was the most frequent histological subtype found (54.3%) after resection of the lesion, followed by the squamous cell carcinoma (45.7%), corroborating the literature’s data.8 The nasal pyramid is the most common site for malignant tumors of the head and neck, which have particular predilection for areas exposed to the sun.9
In the present study, there was a higher incidence (37.1%) of lesions in the nasal ala and columella (subunits 5-6). On the other hand, (41.50%) the literature reports a higher incidence in the nasal dorsum.
The mean age of the operated patients was 68.6 (± 10.8), ranging from 36 to 80 years. According to the literature,the elderly experience more cutaneous neoplasias as compared to the younger population.1
In the reported cases, the male gender was the most prevalent, with 24 (68.6%) occurrences. According to data from the Brazilian National Cancer Institute (Inca), there is an estimated risk of 100.75 new cases per 100,000 men and 82.24 per 100,000 women, regarding the onset of nonmelanoma cutaneous neoplasms.10
The choice of reconstructive method is based on the size, location and depth of the defect to be corrected. In the present study the median-frontal flap was used as the best therapeutic option for the cases demanding reconstruction. The outcomes were deemed satisfactory for both the patient and the medical team. Refinements are required in most cases, with the mean value of interventions calculated at 2.49 (SD = 0.81, min = 2, max = 5) in the present study. A cohort study published by Santos Stahl et al.11 in 2013 shows that performing a two-stage reconstruction – rather than a three-stage procedure – for the refinement of the flap does not increase the rate of complications like partial ischemia or flap necrosis.
Surgery can be performed under sedation or, preferably, with general anesthesia, which was used in 94.2% of the studied cases. The gold standard in the treatment of cutaneous neoplasms is the removal of the lesion followed by a freezing biopsy aimed at defining the surgical margins. Unfortunately in the authors’ medical service this treatment is not usually offered due to possible difficulties for performing the examination. The Head and Neck Surgery team performed most of the resections. Late reconstruction was performed in 5 cases.
Potential complications of the median-frontal flap include bleeding, pain, inadequate healing, infection, dehiscence, distortion of free margins, and flap necrosis.12 Of the cases evaluated, 17.2% had postoperative complications, with hematoma being the most common. Cases that progressed with hematoma required surgical re-intervention.
The frontal flap is the ideal reconstructive choice in many patients and can be performed safely and reliably in a hospital setting.
This technique allows the restoration of the nose’s function, preserving good ventilatory permeability and good aesthetic outcome. Therefore, the technique was instituted as the standard method for nasal reconstruction after resection of neoplasias in the authors’ medical service.
1. Mélega JM. Cirurgia plástica fundamentos e arte - cirurgia reparadora de cabeça e pescoço. Vol. 2. Rio de Janeiro: MEDSI; 2002.
2. Converse JM. Corrective and reconstructive surgery of the nose. In: Converse JM, editor. Reconstructive plastic surgery. 2nd ed. Philadelphia: Saunders; 1977. p. 87-189.
3. Rohrich RJ, Barton FE, Hollier L. Nasal reconstruction. 5th ed. In: Aston SJ, Beasley RW, Thorne CHM, editors. Grabb and Smith's plastic surgery. Philadelphia: Lippincott-Raven; 1997. p. 513-29.
4. Talmant JC. Reconstruction du Nez. In: EMC. Techniques chirurgicales: chirurgie plastique reconstructive et esthétique. Vol. 1. Paris: Elsevier; 2000. p. 325-41.
5. Soares VR. Reconstrução de nariz em neoplasias. Rev Bras Med. 1975;32(1):3-9.
6. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-47.
7. Pitanguy I, Franco T, Escobar R. Reconstrução de nariz. Trib Med.1968;345:22-4.
8. Filho MVPS, Kobig RN, Barros PB, Dibe MJA, Leal PRA. Reconstrução nasal: Análise de 253 casos realizados no Instituto Nacional de Câncer. Rev Bras Cancerologia. 2002;48(2):239-45.
9. Chiummariello S, Dessy LA, Buccheri EM, Gagliardi DN, Menichini G, Alfano C, et al. An approach to managing non-melanoma skin cancer of the nose with mucosal invasion: our experience. Acta Otolaryngol. 2008;128(8):915-9.
10. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2014: incidência de câncer no Brasil [Internet]. Rio de Janeiro: INCA; 2014. Available from: http://www.inca.gov.br/estimativa/2014/estimativa-24042014.pdf
11. Santos Stahl A, Gubisch W, Fischer H, Haack S, Meisner C, Stahl S. A cohort study of paramedian forehead flap in 2 stages (87 flaps) and 3 stages (100 flaps). Ann Plast Surg. 2015;75(6):615-9.
12. Little SC, Hughley BB, Park SS. Complications with forehead flaps in nasal reconstruction. Laryngoscope. 2009;119(6):1093-9.
This study was carried out at the Surgery Department of the Hospital Universitário Polydoro Ernani São Thiago da Universidade Federal de Santa Catarina (UFSC) - Florianópolis (SC), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}