


João Roberto Antonio1; Carlos Roberto Antonio2; Lívia Arroyo Trídico3
Introduction: Androgenetic alopecia is the most common type of hair loss in men and women. Nowadays, medication based treatments are the most frequently used nevertheless they yield poor results. More recently, the use of lasers has been proposed to treat this condition. At the same time, the infiltration of medications in the scalp has also been growing as a therapeutic option, although there are few scientific studies on this treatment modality.
Objective: To evaluate the results of using 1,550nm Erbium-Glass laser associated with the injection of active principles (minoxidil, finasteride, growth factors and a vitamin complex) for the treatment of male and female androgenetic alopecia.
Methods: A retrospective study was carried out with patients with androgenetic alopecia diagnosis, who underwent monthly sessions of the proposed combination therapy. The results were evaluated by means of comparative photographs taken before and after the treatment period and the assessment of the patients' opinion.
Results: Sixty-two patients were treated with 3 to 14 sessions; 48.39% of patients had mild improvement, and 46.77% had significant improvement. The vast majority (96.77%) was satisfied with the treatment. The patients who were very satisfied with the outcomes underwent a greater number of sessions (more than six, on average).
Conclusions: The association of 1,550nm Erbium-Glass laser therapy with the injection of active principles in the scalp is an effective and safe option for the treatment of androgenetic alopecia.
Keywords: ALOPECIA; LASERS; THERAPEUTICS
Androgenetic alopecia is the most common type of hair loss in men and women, affecting 50% of men at 50 years of age and 50% of women at 80 years of age.1, 2 It is a genetic condition caused by the action of circulating androgens. In addition, its multifactorial etiopathogenesis also involves hormonal factors. The clinical picture of hair loss is the result of the genetically determined distribution of hair follicles with specific sensitivity to the androgens and their own sensitized end-receptors.3
The involvement of the follicles leads to a reduction in follicular epithelial proliferation and progressive miniaturization of the scalp’s terminal hairs.2 The terminal follicles are reduced in size and diameter and, have their cycles progressively shortened over time, entailing a reduction in the growth period of the anagen hairs.4 The result is a reduction in hair density and miniaturization, predominantly in the frontolateral and vertex regions in men, and along the frontoparietal region, with diffuse pattern, in women.5
The only drugs currently approved by the FDA for treatment of androgenetic alopecia are finasteride and minoxidil. However, due to the fact it is a very common condition, several types of treatment have been sought, with only a few leading to satisfactory results. Laser therapy has become an alternative treatment both to prevent hair loss and to stimulate its growth in male and female androgenetic alopecia.6
Two types of devices already have FDA clearance for this purpose, due to the minimal level of associated risks – namely the Hair Max Laser Comb (Lexington Int. LLT, Boca Raton, FL, USA) and the TOPHAT 655 (Aspira Science Inc., Boca Raton, FL, USA), both with 655nm wavelength.7
The exact mechanism of this action on the hair is not well defined. Possibly, there is activation of the telogen hairs and reversion into the anagen phase, increasing the cycle’s duration and the growth rate during this phase, preventing its advancement into the regression stage (catagen phase).8
Kim et al. evaluated the effects of fractional 1,550nm laser on male androgenetic alopecia and observed increased hair density and growth. It is known that fractional photothermolysis caused by this wavelength stimulates collagen regeneration. In that study, the histological analysis has evidenced the conversion of follicles from the telogen into the anagen phase.9
Another treatment option for androgenetic alopecia is the application of intradermal injections into the scalp aimed at stimulating hair growth. Although there are few scientific studies on this method, this type of treatment has been growing as a therapeutic option.10-12
The most studied topical substances aimed at stimulating hair follicles, such as minoxidil, finasteride, dutasteride, biotin, vitamins and organic silicon, have also been employed for intradermal use.
The present study’s objective was to evaluate the association of laser therapy with injection of active principles in the scalp using mesotherapy, aimed at treating androgenetic alopecia. In light of the positive results obtained both with laser treatment and mesotherapy in androgenetic alopecia, it was hypothesized that the association of these techniques could lead to optimized results. The dermal stimulus and fractionation columns created by the laser’s action might strengthen the absorption and action of the injected active principles. In this manner, the authors of the present study sought a new and effective therapeutic option for androgenetic alopecia.
A retrospective observational study was carried out including male and female patients older than 18, with clinical diagnosis of androgenetic alopecia, who had undergone at least three sessions of 1,550nm Erbium:Glass (Fraxel Laser Dual®, Solta Medical, Hayward, CA, USA) laser therapy associated to the injection of active principles (minoxidil, finasteride, growth factors and vitamin complex), from January 2015 to July 2016, at a private practice in the city of São José do Rio Preto, São Paulo State, Brazil. The sessions were performed at intervals of one month. Patients with other types of alopecia were excluded from the study. Women at childbearing age underwent oral hormonal contraceptive use prior to the beginning of the treatment due to the presence of finasteride among the injection’s active principles. The study was approved by the Research Ethics Committee of the Faculdade de Medicina de São José do Rio Preto (SP), Brazil.
The patients initially underwent injectable anesthesia on the scalp with 2% lidocaine with vasoconstrictor by means of anesthetic points in the region to be treated, in the frontoparietal direction. Subsequently, 1,550nm Erbium:Glass laser was applied with the following settings: energy = 6mj, treatment level = 3, and six passes (three in the vertical direction, followed by three in the horizontal direction). Next, intradermal injection with the following active principles was performed: 1ml 0.05% finasteride, 2ml 0.5% minoxidil, 2 ml of a vitamin combination (25mg L-methionine, 50mg L-taurine, 10mg L-proline, 10mg biotin, 5mg vitamin B, 10mg vitamin B3, 10mg vitamin B6, 10mg D-panthenol), and 2ml of growth factors (1% copper peptide, 1% IGF, 1% VEGF, 40mg D-panthenol and 10mg biotin). Patients were instructed to wash the scalp two hours after the intradermal injections.
The assessment of the results was based on photographs taken before and after the treatment, and analysis performed by a dermatologist unrelated to the study, who classified the comparison between the images in: absence of improvement, slight improvement and significant improvement of androgenetic alopecia. The patients’ satisfaction was assessed by an opinion survey that rated the answers regarding the treatment as: dissatisfied, satisfied and very satisfied.
Sixty-two patients participated in the study (27 men, 35 women / mean age = 45.27 / age range = 20 to 81).
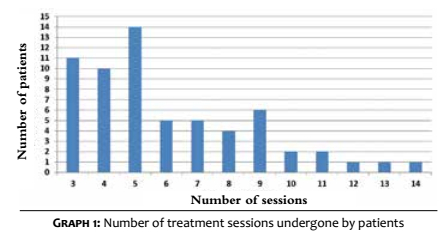
The patients underwent one session per month (min = 3, max = 14 / average = 6 sessions per month) (Graph 1).
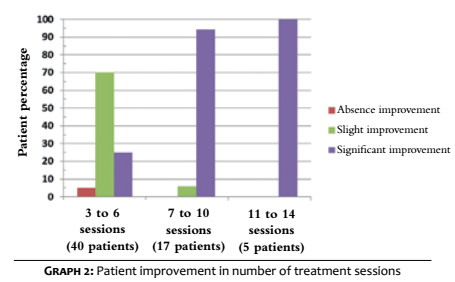
The assessment of the photographs carried out by a physician classified 3 patients (4.84%) with absence of improvement, 30 (48.39%) with slight improvement and 29 (46.77%) with significant improvement. Of the patients who showed slight improvement, the majority (96.55%) underwent 3 to 6 sessions. Among those who experienced significant improvement, the majority (67.7%) underwent more than 7 sessions (Graph 2).
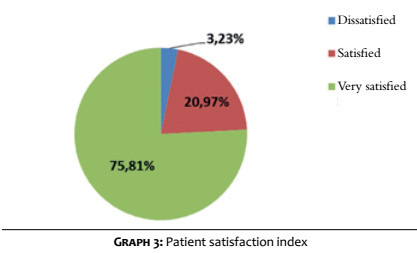
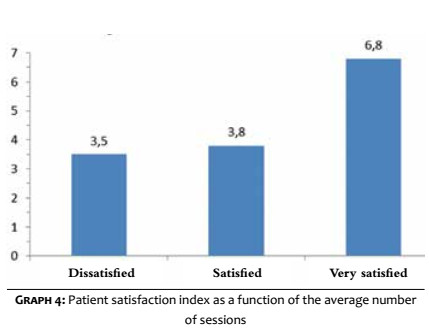
Regarding the evaluation of the patients’ satisfaction, 2 (3.23%) said they were dissatisfied with treatment (one of whom underwent 3 sessions, the other 4 sessions), 13 (20.97%) reported being satisfied, and 47 (75.80%) said they were very satisfied (Graph 3). Those who were satisfied underwent on average 3.8 sessions, while those who were very satisfied underwent an average of 6.8 sessions (Graph 4).
Adverse effects were deemed as mild, with erythema being more common within the first hours after the session, and mild pain on the scalp occurring on the day after the treatment.
Several studies have demonstrated the use of laser therapy for hair growth, describing an increase in hair density and of anagen hairs in most of them.1,6-9,13,14 Kim et al. have suggested that the mechanisms of action involved in inducing hair growth using fractional laser includes increased blood flow, induction of cytokines and growth factors associated with hair biology, as well as platelet-derived growth factor, keratinocyte growth factor, insulin-like growth factor and fibroblast growth factor. In addition, there is direct stimulation of stem cells, bulge cells or dermal papilla cells.9 Moreover, laser radiation acts to reduce the inflammation present in the follicles in cases of alopecia areata.6,14
The treatment using the injection of active principles in the scalp aimed at controlling hair loss has increased in recent years.11 The effects of hair mesotherapy are: increase in the local microcirculation and nutrient supply, delayed hair involution process and stimulation of hair growth due to the trauma in the dermis caused by the needling procedure.10,15,16 Minoxidil acts as a vasodilator, vitamins are crucial in promoting hair growth, finasteride acts by inhibiting the hormonal action involved in androgenetic alopecia, and growth factors act directly on the development of the hair follicle.10,17
In light of the findings of the present study, it was possible to observe that the improvement in the clinical picture of androgenetic alopecia was proportional to the number of therapeutic sessions undergone by the patients, since the majority of the patients who underwent more than 7 sessions experienced a significant improvement of the picture, and all patients who underwent more than 11 sessions showed an important improvement of androgenetic alopecia.
Patient satisfaction was also progressive according to the number of sessions. Overall, the majority of patients (96.77%) were satisfied with the treatment. The majority of patients was significantly satisfied (75.8%) and underwent the greatest number of sessions on average (> 6 sessions).
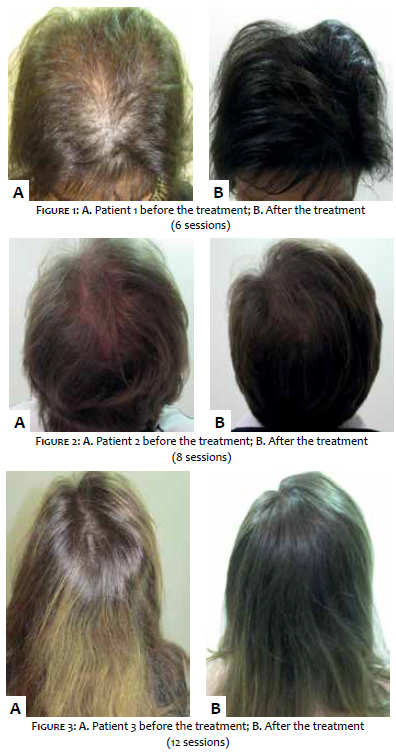
In face of these data, it is possible to conclude that the combination of two treatments in a single session aimed at treating androgenetic alopecia allowed patients to achieve an important degree of personal satisfaction, since it is a condition of difficult treatment at the present time. In addition, the improvement observed on the photographs analysis, demonstrates the perceptible increase in the hair density obtained with the treatment (Figures 1-3).
Androgenetic alopecia is a frequent complaint in dermatological practices, being characterized by poor therapeutic results to date. The present study allows to conclude that the association of 1,550nm Erbium:Glass laser with injections of active principles (minoxidil, finasteride, growth factors and vitamin complex) in the scalp was effective and safe for the treatment of this condition, reinforcing the relevance of this novel treatment option.
1. Munck A, Gavazzoni MF, Trüeb RM. Use of low-level laser therapy as monotherapy or concomitant therapy for male and female androgenetic alopecia. Int J Trichology. 2014;6(2):45-9.
2. Olsen EA, Messenger AG, Shapiro J, Bergfeld WF, Hordinsky MK, Roberts JL, Stough D,Washenik K, Whiting DA. Evaluation and treatment of male and female pattern hair loss. J Am Acad Dermatol. 2005;52(2):301-11.
3. Rutowitsch MS, Antonio JR, Steiner D, Talarico S. Alopecia androgenética. An Bras Dermatol. 1999;74(6):561-572.
4. Whiting DA. Possible mechanisms of miniaturization during androgenetic alopecia or pattern hair loss. J Am Acad Dermatol. 2001;45(3 Suppl):S81-6.
5. Belda Junior W, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 2nd ed. Rio de Janeiro; 2014.
6. Rangwala S, Rashid RM. Alopecia: a review of laser and light therapies. Dermatol Online J. 2012;18(2):3.
7. Afifi L, Maranda EL, Zarei M, Delcanto GM, Falto-Aizpurua L, Kluijfhout WP,Jimenez JJ. Low-level laser therapy as a treatment for androgenetic alopecia. Lasers Surg Med. 2016;49(1):27-39.
8. Wikramanayake TC, Rodriguez R, Choudhary S, Mauro LM, Nouri K, Schachner LA, Jimenez JJ. Effects of the Lexington LaserComb on hair regrowth in the C3H/HeJ mouse model of alopecia areata. Lasers Med Sci. 2012;27(2):431-6.
9. Kim WS, Lee HI, Lee JW, Lim YY, Lee SJ, Kim BJ, Kim MN, Song KY, Park WS. Fractional photothermolysis laser treatment of male pattern hair loss. Dermatol Surg. 2011;37(1):41-51.
10. Kutlubay Z, Karaku Ö. Hair Mesotherapy. Hair: Ther Transplant; 2012;2(1):1000e102.
11. Sarkar R, Garg VK, Mysore V. Position paper on mesotherapy. Indian J Dermatol Venereol Leprol. 2011;77(2):232-7.
12. Jäger C, Brenner C, Habicht J, Wallich R. Bioactive reagents used in mesotherapy for skin rejuvenation in vivo induce diverse physiological processes in human skin fibroblasts in vitro- a pilot study. Exp Dermatol. 2012;21(1):72-5.
13. Lanzafame RJ, Blanche RR, Bodian AB, Chiacchierini RP, Fernandez-Obregon A, Kazmirek ER. The growth of human scalp hair mediated by visible red light laser and LED sources in males. Lasers Surg Med. 2013;45(8):487-95.
14. Jimenez JJ, Wikramanayake TC, Bergfeld W, Hordinsky M, Hickman JG, Hamblin MR,Schachner LA. Efficacy and safety of a low-level laser device in the treatment of male and female pattern hair loss: a multicenter, randomized, shamdevice-controlled, double-blind study. Am J Clin Dermatol. 2014;15(2):115-27.
15. Atiyeh BS, Ibrahim AE, Dibo AS. Cosmetic mesotherapy: between scientific evidence, science fiction, and lucrative business. Aesthetic Plast Surg. 2008;32(6):842-849.
16. Madhere S, editor. Aesthetic Mesotherapy and Injection Lipolysis in Clinical Practice. New York: Informa Healthcare; 2007. p. 109-143.
17. Peus D, Pittelkow MR. Growth factors in hair organ development and the hairgrowth cycle. Dermatol Clin. 1996;14(4):559-72.
This study was carried out at Clínica Pelle – Campos dos Goytacazes (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}