


Letícia Abel Penedo de Moura1; Jane Marcy Neffá Pinto2; Marcelo de Souza Teixeira3
Introduction: Melasma is a chronic hyperpigmentation of the skin, characterized by irregular brownish spots distributed in areas exposed to the sun, common in Brazilian women. Due to facial involvement, it impacts on appearance, causing psychosocial and emotional discomfort, thus affecting patients' quality of life.
Objective: A double-blind, longitudinal, comparative and monocentric clinical study was conducted comparing the quality of life and the pigmentation intensity of melasma in women before and 60 days after oral use of Lingonberry (Vaccinium vitis idaea L.) extract in association with sunscreen as the only topical treatment.
Methods: The study investigated the influence of the presence of melasma on the quality of life of volunteers before and after 60 days of oral use of lingonberry extract (Vaccinium vitis idaea L.) in combination with topical sunscreen and in patients who just wore sunscreen through the Melasma Quality of Life Scale Scale. Comparative and standardized dermatoscopic photographs of the lesions had the intensity of the pigmentation evaluated by an optical density analysis program.
Results: Evaluation of the Melasma Quality of Life Scale indicated a reduction of the discomfort caused by the pathology after the use of the phytotherapic drug in association with the sunscreen, which did not occur in the group that used the sunscreen alone. The analysis of the pigmentation density in the photographs showed a significant reduction in the degree of pigmentation after the use of phytotherapic drug, as well as no alterations in the control group.
Conclusion: The use of lingonberry may contribute to the treatment of facial melasma.
Keywords: MELASMA; PHYTOTHERAPY; SKIN PIGMENTATION
The skin is the most visible phenotypic characteristic of the human being, and its color, one of its most variable factors. Knowledge about the genetic, evolutionary and cultural aspects related to the establishment of human skin color levels is restricted.1 Human skin and hair pigmentation is related to melanogenic activity in melanin producing cells, as well as on the size, number, composition, and distribution of melanocyte cytoplasmic particles called melanosomes, as well as the chemical nature of the melanin they contain.1
Melasma is common melanoderma, characterized by macules on areas exposed to UV radiation, with brownish pigmentation of different intensities, mainly affecting adult women (aged 30 to 55 years) of childbearing age.2
The name melasma is derived from the Greek melas, which means black. Also known as chloasma, equally derived from the Greek cloazein: to be greenish. The name melasma is, therefore, more appropriate for the disease.3
The etiopathogenesis of melasma has not yet been fully elucidated; It is known, however, that several factors are involved in the expansion or in its emergence. Periods of partial reduction during the winter and periods of exacerbation during the summer are observed, and the lesions may appear abruptly due to intense sun exposure, or gradually, by constant exposure.
One of the most well-accepted theories for the appearance of this dyschromia is that ultraviolet radiation causes the peroxidation of the lipids of the cell membrane, with consequent formation of free radicals, which stimulate the melanocytes to produce melanin excessively, thus generating cutaneous hyperpigmentation.4 The hormonal influence on the etiopathogenesis of melasma is structured by the high frequency of presence in pregnant women, users of oral contraceptives, and women in hormone replacement therapy.4
It is a dermatological disease diagnosed with a clinical examination, which presents characteristic chronicity, with frequent recurrences and great refractoriness to existing treatments.5
There is no consensus on the clinical classification of melasma. In the face, where it is more frequent, two main patterns are recognized: centrofacial, affecting the central regions of the forehead, supralabial and mental regions; And malar, which affects the zygomatic regions. Some authors also add a third, less frequent pattern called the mandibular.5
Melasma may be classified as transient or persistent. When the stimuli are interrupted for a year and the melasma disappears, it is classified as transient; if it does not disappear, is of the persistent type, having as a causal factor the solar radiation, among others.5
According to data from the Brazilian Society of Dermatology, in 2006 Brazil had 57,343 cases of face melasma diagnosed; melanodermas make up the third most common group of dermatological diseases in Brazil.6
Because it appears mainly on the face, melasma disturbs the patient, negatively affecting his or her psychological and emotional well-being, thus generating a negative impact on the quality of life, which often leads the person to seek the dermatologist.7 Thus, the need arose for the development of a standardized and validated questionnaire in order to evaluate the quality of life of these patients. The MELASQoL (Melasma Quality of Life Scale) is an instrument that covers three situations affected by dermatosis: social life, recreation / leisure and emotional well-being.8, 9 In Brazil, the questionnaire was translated into Portuguese in 2006 (MELASQoL- BP), following World Health Organization standards.10 The response to MELASQoL of 300 patients of both genders from different demographic regions was investigated; Among the answers, 65% of the patients reported discomfort with facial melasma, 55% felt frustration, and 57% were ashamed of the discolored appearance of the skin.11
The treatment of melasma is often unsatisfactory, due to the great recurrence of the lesions and the absence of alternatives for definitive whitening. From the topical treatments available, hydroquinone is considered the most efficient drug, despite its adverse effects – irritant or allergic contact dermatitis, hypopigmentation, and postinflammatory hyperpigmentation.12
Controlled clinical studies indicate photoprotection and use of topical and / or oral whitening agents as the main treatment measures.10, 13 Vegetable substances with antioxidant functions have been reported to be useful in the treatment of melasma. Vacciniumvitis-idaea, commonly called lingonberry or cowberry, is a small green shrub of the Ericaceae family that produces edible fruits as small as a pea. Its high antioxidant capacity is reflected by its high ORAC (Oxygen Radical Absorbance Capacity) of 16,000, thus indicating the great potential of the extract of this vegetable in acting against free radicals in the human organism.14
This study sought to investigate this substance in the control of melasma in Brazilian women.
This is a double-blind, longitudinal, comparative, monocentric clinical study approved by the University Ethics Committee in Human Research at the University Hospital of the Fluminense Federal University (Universidade Federal Fluminense), in which 42 volunteers with facial melasma and aged between 30 and 55 years were investigated.
During the period of March and April of 2015, patients who had clinical complaints of melasma were selected and monitored at the Dermatology Outpatient Clinic at the University Hospital of the Fluminense Federal University, Niterói, Rio de Janeiro, Brazil.
All participants met the following inclusion criteria: presence of facial melasma in women aged between 30 and 55 years, who had not undergone topical or oral depigmentation treatment for at least six months, and agreed to have their photographs published for scientific purposes. Were excluded from the project, women who were pregnant or lactating, and women with active dermatoses in the area to be treated; who, in the 30 days prior to the study, used products based on hydroquinone, vitamin C, azelaic acid, kojic acid, phytic acid, glycolic acid, antiinflammatories and retinoid derivatives.
After signing the Consent Form, the 42 volunteers were randomly divided into the control group (21), who used only the Photoprot® FPS 100 sunscreen (Biolab, São Paulo, Brazil) throughout the surface of the face, three times a day, according to the manufacturer's instructions; and the phytotherapic group (21), in which patients used sunscreen in combination with the lingonberry phytotherapic (vaccinium vitis ideae) for 60 days, the length of the study. At the initial visit, the volunteers were clinically evaluated and submitted to photographic recording of their macules by the non-polarized dermatoscope, Medicam 800 FotoFinder (FotoFinder Systems GmbH, Aichner, Birnbach, Germany). The dermoscopic images were captured with an increase in magnitude of 20x.
The impact of melasma on quality of life was assessed using the MELASQoL (Melasma Quality of Life scale), a Portuguese language version validated by Cestari et al.15 at the beginning and at the end of the study.
Sixty days after the first photographic record of the macules, the volunteers returned to the dermatology outpatient clinic for the control registry. In this visit, in addition to responding to the MELASQoL questionnaire, the volunteers evaluated the effect of the proposed protocol on the macules using the following parameters: 0 - worsened; 1 - stable; 2 - improved; 3 - improved significantly. The images generated by FotoFinder were evaluated by two dermatology physicians with the same options of responses contained in the evaluations of the volunteers (0 - worsened; 1 - stable; 2 - improved; 3 - improved significantly).16
The photographs were analyzed by the Scion Image Software, Version 4.03, (Scion Corporation, MD, USA). The dark areas (melasma) of the photographed skin, as well as the nonpigmented area of the adjacent one, were quantified; followed by the subtraction of the measured values, aiming to eliminate the variation of the intensity in skin color when comparing the macules among the volunteers.17
In order to investigate the influence of the study on the quality of life of the volunteers, the responses to the MELASQoL questionnaire, before and after treatment, were analyzed by the paired t-test. For the analyses of the optical densities of the macules, before and after the treatment, in each group and between the groups, the Anova test with Tukey's Post Hoc Analysis was used. The level of statistical significance was set to p < 0.05. The program used for data analysis was Prism 6.
All volunteers in the study reported the presence of melasma macules for more than two years. Among the 42 volunteers, 38 (control group: 18, phytotherapic group: 20) completed the study; four left it for personal reasons.
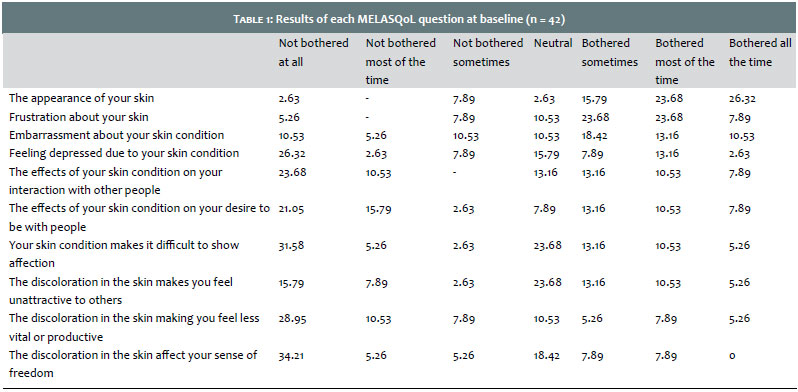
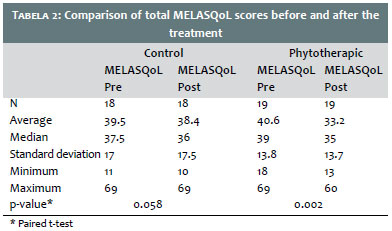
Initial analysis of MELASQoL revealed that 65.79% of patients were uncomfortable with their skin appearance, 55.26% experienced frustration or embarrassment due to their skin condition, 42.11% felt depressed, and 23.68% do not feel attractive. For 34.21% of the volunteers, however, melasma does not impact the relationships they have with other people; for 39.47% it does not affect the desire to be with other people; 26.32% of patients have no difficulty in showing affection; 47.37% do not feel less productive; and for 44.74% of the volunteers, melasma does not affect their sense of freedom (Table 1). The evaluation of the total MELASQoL score indicated no significant change after treatment in the control group (p = 0.058); however, a significant reduction was observed in the total MELASQoL score in the phytotherapic group (p = 0.002). The average MELASQoL score was 39.5 before treatment and 38.4 after the study in the control group; its value decreased from 40.6 before medical intervention to 33.2 after the use of the phytotherapic in combination with the sunscreen (Table 2).
Regarding the evaluation of the efficacy of the treatment, in the opinion of the patients, improvement of melasma was achieved in 33.3% of the volunteers in the control group and in 66.6% of the volunteers in the phytotherapic group. In the evaluation of dermatologist physicians, the treatment showed improvement in 30% of the patients in the control group and in 80% of the patients in the phytotherapic group.
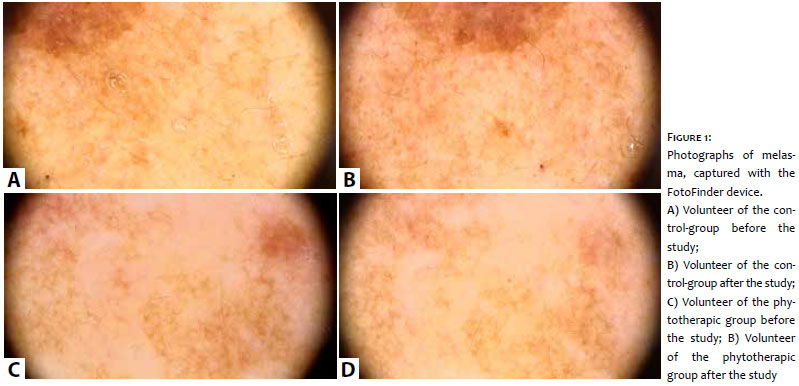
The quantitative analyses of optical density have indicated that the control group had no significant change in pigment density before and after the use of the topical photoprotection; the phytotherapic group, however, presented a significant reduction (p = 0.01) in the intensity of pigmentation during the study (Figure 1) (Graph 1).
Melasma, due to being a very frequent dermatosis, is extensively investigated and has a large number of publications.18,19
The MELASQoL questionnaire, in the Brazilian version, was validated to evaluate the impact of this pathology, allowing for cultural identity to be preserved by using it in national clinical and research practices.10, 20 In the present study, the average total MELASQoL score was 38.40 ± 10.50, close to the averages found in other Brazilian studies.20, 21
Emotional well-being was the most affected are by melasma; just like in the study conducted by Balkrishnan et al.,22 social relations were also affected by melasma in our study, being that 66% of the volunteers reported that the macules influenced their sense of freedom, and 70% noticed that their relationships with other people had been affected, which also indicates the high degree of embarrassment generated by the presence of these macules on the face.
The absence of efficient treatment for the control or cure of melasma, as well as its frequent recurrence, still creates numerous lines of research with constant discussions on therapeutic modalities, of great clinical and scientific interest.23-25
In the present study, the oral use of the LingonMAX® concentrated nutrition composed of procyanidins, resveratrol and anthocyanidins, with both anti-inflammatory and antioxidant properties, presented great whitening potential of facial melasma according to the quantitative evaluation of the optical density of pigmentation in the photographs. This result is supported by previous studies, which indicated beneficial effects of the active principle in this pathology, although isolatedly.26,27
In 2002, Ni et al28 concluded that oral use of procyanidins (75 mg / day) for 30 days reduced the extent of the area affected by melasma (P < 0.001) and average intensity of pigmentation (P < 0.001) in Chinese women. The study did not show an adverse reaction to the treatment. In 2004, Shahrir et al29 conducted a double-blind controlled study with 30 women, in which the consumption of procyanidins (80mg / day) during 30 days resulted in significant improvement of the macules, highlighting the whitening potential of this vegetable compound.
Resveratrol, a polyphenol that can be found mainly in grape seeds, has an important antioxidant activity30,31 and numerous pharmacological functions – including tyrosinase inhibitory activity, which converts tyrosine into L-3,4-dihydroxyphenylalanine (L-DOPA), and L-DOPA in dopaquinone, through hydroxylation and oxidation reactions, has also been shown to have a positive effect on melasma treatments.7, 32 Some studies, however, have demonstrated that resveratrol alone does not inhibit melanin synthesis effectively, which increases when it is used in combination with other depigmenting agents.33
Despite the lack of scientific publications, anthocyanidins, also called anthocyanins, are natural pigments responsible for a wide variety of colors in fruits, flowers and leaves, ranging from red-orange to purple and blue,34 also have a depigmenting action. Its natural function is to protect plants and fruits against ultraviolet light (UV), and to avoid the production of free radicals.35 Thus, because they have antioxidative functions, inhibitory action of the enzyme tyrosinase, anthocyanidins appear to be promising substances in the control of melasma. No adverse effects were observed during the present study, which suggests safety in the oral use of lingonberry extract (vaccinium vitis) (100mg / day) as an adjuvant in the control of facial melasma.
Controlling melasma often requires alternating depigmenting agents. The results obtained in the present study allow us to conclude that lingonberry extract may be an effective strategy in the control of melasma, also allowing future comparative clinical studies to ratify its efficiency and tolerability.
1. Costin GE, Hearing VJ. Human skin pigmentation: melanocytes modulate skin color in response to stress. FASEB J. 2007;21(4):976-94.
2. Kasraee B, Safaee Ardekani GH, Parhizgar A, Handjani F, Omrani GR, et al. Safety of topical methimazole for the treatment of melasma. Transdermal absorption, the effect on thyroid function and cutaneous adverse effects. Skin Pharmacol Physiol. 2008;21(6):300-5.
3. Sanchez NP, Pathak MA, Sato S, Fitzpatrick TB, Sanchez JL, Mihm MC Jr. Melasma: a clinical, light microscopic, ultrastructural, and immunofluorescence study. J Am Acad Dermatol. 1981;4(6):698-710.
4. Katsambas AD, Lotti TM. European handbook of dermatological treatments: Springer; 2003.
5. Kang WH, Yoon KH, Lee ES, Kim J, Lee KB, Yim H, et al. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002;146(2):228-37.
6. Handel AC, Miot LD, Miot HA. Melasma: a clinical and epidemiological review. An Bras Dermatol. 2014;89(5):771-82.
7. Miot LDB, Miot HA, Silva MG, Marques MEA. Fisiopatologia do melasma. Anais brasileiros de dermatologia. 2009;84(6):623-35.
8. Sharquie KE, Al-Tikreety MM, Al-Mashhadani SA. Lactic acid chemical peels as a new therapeutic modality in melasma in comparison to Jessner's solution chemical peels. Dermatologic surgery. 2006;32(12):1429-36.
9. Grimes P, Nordlund JJ, Pandya AG, Taylor S, Rendon M, Ortonne J-P. Increasing our understanding of pigmentary disorders. Journal of the American Academy of Dermatology. 2006;54(5):S255-S61.
10. Cestari TF, Balkrishann R, Weber MB, Prati C, Menegon DB, Mazzotti NG, et al. Translation and cultural adaptation to Portuguese of a quality of life questionnaire for patients with melasma. Med Cutan Iber Lat Am. 2006;34(6):270-4.
11. Cestari TF, Hexsel D, Viegas ML, Azulay L, Hassun K, Almeida AR, et al. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: the MelasQoL-BP study and improvement of QoL of melasma patients after triple combination therapy. Br J Dermatol. 2006;156 (Suppl 1):13-20.
12. Victor FC, Gelber J, Rao B. Melasma: a review. J Cutan Med Surg. 2004;8(2):97-102.
13. Pandya A, Berneburg M, Ortonne JÄ, Picardo M. Guidelines for clinical trials in melasma. British Journal of Dermatology. 2006;156(s1):21-8.
14. Li Y, Dou X, Cheng Q. Lingonberry extract, the preparing method and use thereof. Google Patents; 2009.
15. Cestari TF, Hexsel D, Viegas M, Azulay L, Hassun K, Almeida A, et al. Validation of a melasma quality of life questionnaire for Brazilian Portuguese language: the MelasQoL‚ÄêBP study and improvement of QoL of melasma patients after triple combination therapy. British Journal of Dermatology. 2006;156(s1):13-20.
16. Costa A, Moisés TSA, Cordero T, Alves CRT, Marmirori J. Association of emblica, licorice and belides as an alternative to hydroquinone in the clinical treatment of melasma. An Bras Dermatol. 2010;85(5):613-20.
17. Wang HÄ, Chen CÄ, Wen ZÄ. Identifying melanogenesis inhibitors from Cinnamomum subavenium with in vitro and in vivo screening systems by targeting the human tyrosinase. Experimental dermatology. 2011;20(3):242-8.
18. Jadotte YT, Schwartz RA. Melasma: insights and perspectives. Acta Dermatovenerologica Croatica. 2010;18(2):124-9.
19. Chen Z, Chen Y, Zeng J, Wang Y, Ye T, Zhou Q, et al. Quality of randomized controlled trials reporting in the treatment of melasma conducted in China. Trials. 2015;16:156.
20. Freitag FM, Cestari TF, Leopoldo LR, Paludo P, Boza JC. Effect of melasma on quality of life in a sample of women living in southern Brazil. J Eur Acad Dermatol Venereol. 2008;22(6):655-62.
21. Purim KS, Avelar MF. Photoprotection, melasma and quality of life in pregnant women. Rev Bras Ginecol Obstet. 2012;34(5):228-34.
22. Balkrishnan R, McMichael AJ, Camacho FT, Saltzberg F, Housman TS, Grummer S, et al. Development and validation of a health-related quality of life instrument for women with melasma. Br J Dermatol. 2003;149(3):572-7.
23. Ibrahim ZA, Gheida SF, El Maghraby GM, Farag ZE. Evaluation of the efficacy and safety of combinations of hydroquinone, glycolic acid, and hyaluronic acid in the treatment of melasma. J Cosmet Dermatol. 2015;14(2):113-23.
24. Rodrigues M, Pandya AG. Melasma: clinical diagnosis and management options. Australas J Dermatol. 2015;56(3):151-63.
25. Zhong SM, Sun N, Liu HX, Niu YQ, Wu Y. Reduction of facial pigmentation of melasma by topical lignin peroxidase: A novel fast-acting skin-lightening agent. Exp Ther Med. 2015;9(2):341-4.
26. Puupponen-Pimia R, Nohynek L, Hartmann-Schmidlin S, Kahkonen M, Heinonen M, Maatta-Riihinen K, et al. Berry phenolics selectively inhibit the growth of intestinal pathogens. J Appl Microbiol. 2005;98(4):991-1000.
27. Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma. J Am Acad Dermatol. 2006;54(5):S272-S81.
28. Ni Z, Mu Y, Gulati O. Treatment of melasma with Pycnogenol. Phytother Res. 2002;16(6):567-71.
29. Shahrir M, Saadiah S, Sharifah I. The efficacy and safety of French Maritime pine bark extract in the form of MSS Complex Actinosome on melasma. Int Med J. 2004;3(2):130-2.
30. Holthoff JH, Woodling KA, Doerge DR, Burns ST, Hinson JA, Mayeux PR. Resveratrol, a dietary polyphenolic phytoalexin, is a functional scavenger of peroxynitrite. Biochem Pharmacol. 2010;80(8):1260-5.
31. Iuga C, Alvarez-Idaboy JR, Russo N. Antioxidant activity of trans-resveratrol toward hydroxyl and hydroperoxyl radicals: a quantum chemical and computational kinetics study. J Org Chem. 2012;77(8):3868-77.
32. Kim YM, Yun J, Lee CK, Lee H, Min KR, Kim Y. Oxyresveratrol and hydroxystilbene compounds. Inhibitory effect on tyrosinase and mechanism of action. J Biol Chem. 2002;277(18):16340-4.
33. Satooka H, Kubo I. Resveratrol as a k cat type inhibitor for tyrosinase: Potentiated melanogenesis inhibitor. Bioorg Med Chem. 2012;20(2):1090-9.
34. Tosun I, Ustun NS, Tekguler B. Physical and chemical changes during ripening of blackberry fruits. Scientia agricola. 2008;65(1):87-90.
35. Inhibition of lipid peroxidation and the active oxygen radical scavengingeffect of anthocyanin pigments isolated from Phaseolus vulgaris L. Biochem Pharmacol. 1996;52(7):1033-9.
This study was performed at the Universidade Federal Fluminense (UFF), Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}