


Rebeca Alvares Rodrigues Maffra de Rezende1; Flávio Barbosa Luz2
Aspiration curettage of sweat glands is a minimally invasive surgical technique for the treatment of axillary hyperhidrosis. It is safe and easy to perform, offers a high success rate and comparatively few side effects. It is generally well tolerated by patients and requires a reduced recovery time when compared to other surgical modalities.
Keywords: HYPERHIDROSIS; SURGERY; CURETTAGE
The majority of patients with severe axillary hyperhidrosis need to consider surgery as a therapeutic option.1
Local surgical treatment of axillary hyperhidrosis is aimed at eliminating the greatest possible number of sweat glands from that region, retaining – to the extent possible – the axilla's normal aesthetic appearance and arm's mobility.2
Several surgical techniques have been developed and modified over the years. The most important of them can be classified into four types: I) block resection of the subcutaneous tissue and overlying skin (Hurley and Shelley, 19633; Tipton, 19684); II) block excision of a small part of the central axillary region with the removal of subcutaneous tissue in adjacent regions (Bisbal, 19875; Weaver, 19706; Hurley and Shelley, 19667); III) methods which remove only the subcutaneous tissue, without excision of the skin (Skoog, 19628; Jemec, 19759) and IV) methods which remove the subcutaneous tissue and deep dermis, without excision of the skin (Darabaneau, 200810, Kim, 200811; Rho, 200812; Boni, 200613; Bechara, 200614; Tronstad, 201415; Feldmeyer, 201516).
Nevertheless, it was only after the development of minimally invasive techniques (e.g. curettage9,17,18, liposuction19, laser20, ultrasonic surgical aspiration,21,22 and aspiration curettage10-16) that its use became more widespread.
Minimally invasive techniques offer many advantages, such as reduced risk of infection, diminished pain in the postoperative period, reduced recovery time and less scarring when compared to traditional surgical methods. However, the small size of the operating field during the implementation of these procedures requires great skillfulness from surgeons.23
Aspiration curettage of the sweat glands is a minimally invasive, safe and easy to perform surgical technique, which has high success rates and few side effects. It also offers the possibility of permanent reduction of hyperhidrosis, which corresponds to the most frequent request from patients. 24,25
For the preparation of the present article, MEDLINE and Cochrane databases were searched using the following terms: hyperhidrosis, axillary hyperhidrosis, surgery, aspiration curettage.
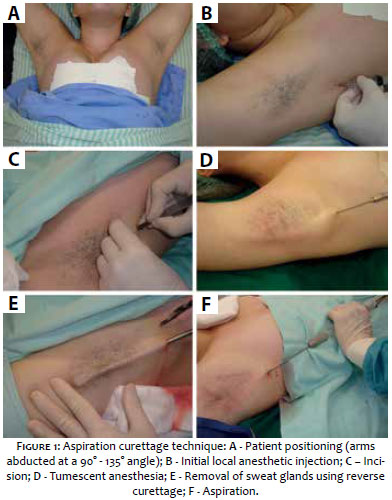
Aspiration curettage technique
The treatment of axillary hyperhidrosis based on surgical removal consists of the removal of the eccrine, apocrine and apo-eccrine glands of the region in question. This technique has many variations. The procedure, which is currently carried out ambulatorially with tumescent anesthesia, consists of two main phases: dissection of the dermis from the underlying subcutaneous tissue, and removal of the sweat glands from the dermis and the region comprising the dermo-hypodermic junction.5
The region to be treated generally extends for 1cm to 2cm beyond the axilla's hairy area. Nonetheless, the iodine-starch test can be performed before surgery in order to mark the affected area and prevent the occurrence of residual hyperhidrosis areas.
The axillary hair can be shaved from 15 to 30 days before surgery. Once having been shaved, the growing hair should not be shaved again so as to allow easy visualization and delimitation of the area to be treated, therefore serving as a parameter for interrupting the procedure.
Step-by-step of the surgery
STEP 1 – Patient's positioning:
Patients are positioned in the supine position with the arms abducted (90-135º angle) in order to expose the axilla. Excessive abduction should be avoided in order to prevent lesion in the brachial plexus (Figure 1).26-28
STEP 2 - Asepsis and antisepsis:
The asepsis and antisepsis are performed using a chlorhexidine or 70% alcohol solution.
STEP 3 - Initial local injection of anesthetic / Incision:
After the initial local anesthetic injection, three small incisions are usually performed outside the area to be curetted, for surgical access. These incisions are made in different points, according to the surgeon's preference: in the superomedial aspect of the axilla, in the anterior and distal borders, in the central portion of the axilla, in the upper inner region29-31 or infralateral region of the arm (Figures 1 B and C).
STEP 4 -Introduction of the injection cannula / Tumescent anesthesia:
A volume of 100-500 ml of tumescent solution is subsequently injected as superficially as possible in areas previously marked in each axilla, creating the effect of "peau d'orange" in the overlaying tissue.26,30,32,33 The use of small diameter infusion cannulas is important for the patient's comfort. Although the standard formula for tumescent anesthesia is 1,000 ml normal saline, 50-100 ml 1% lidocaine, 1 ml 1:1,000 epinephrine and 12.5 ml sodium bicarbonate, there are many variants of this formula (Figure 1 D).34
This solution minimizes bleeding, makes the dissection easier and reduces ecchymosis.35 The prolonged analgesic effect of lidocaine deposits in the tissue ensures some comfort in the immediate postoperative period.36 The expansion of the axilla's soft tissue minimizes the risk of lesion in the brachial plexus. 37
STEP 5 – Back-and-forth movements for the subdermal tunneling:
After the whitening of the region by hemostasis, subcutaneous tunnels are created via precise dissection (a Schroeder curette can be used at this stage), with back-and-forth movements so as to separate the dermis from the subcutaneous tissue. Subcutaneous sweat glands are thus mobilized.
STEP 6 - Removal of the glands through inverted curettage with or without aspiration (dermal and subcutaneous tissue):
Curettage:
Next, a tool with a cutting edge (Fatemi cannula, Cassio cannula or event a dermatological curette) is inserted in order that the dermal curettage is performed. (Figure 1E) Additional care must be taken when these curettes are used in isolation. If used too aggressively, can lead to skin necrosis.
Most of the sweat glands of all kinds (eccrine, apocrine and apo-eccrine) in the axillae of adult Caucasians are located in the subcutaneous tissue, in the interface with the dermis – and not in the dermis.38
It would be impossible to eradicate all subcutaneous glands using only superficial liposuction, since some of them are firmly adhered to the dermis, and a considerable force would be required to separate the glands from their ducts.38-40
Likewise, curettage cannot be performed in a wrong anatomical tissue layer. 41 Performing the procedure in a deep level makes it virtually impossible to completely remove the sweat glands.42
The tension of the overlying skin, as well as the force applied during the scraping movements is of great importance during the inverted curettage. In this way, the surgeon's non-dominant hand can help in the procedure, compressing the overlaying skin.26,43
The curettage must be carefully performed around the incision sites, since the subcutaneous tissue located near the incisions might not be properly removed only by liposuction.44
The size cannula's size and orifices, in addition to the vacuum's intensity and the movement's speed, directly affect the amount of tissue removed.40
The surgery's success depends on the removal of the sweat glands in the dermis / subcutaneous junction up until the point where the axillary tissue becomes similar to a total skin graft.24,38 Thus, a cannula with a cutting edge is more suitable for performing curettage of the deep dermis – a more aggressive procedure – and the more efficient removal of sweat glands, achieving higher cure rates. This area would become irrigated with the blood of the surrounding skin, which did not undergo the procedure.26
Aspiration:
The aspiration of the removed tissue can be performed manually or mechanically (Figure 1 F).
In the manual vacuum aspiration variant, a syringe is attached to the cannula, which is inserted into the tissue to be removed before the plunger is retracted. There must be a mechanical lock to keep the plunger retracted. As this system does not provide a deep and continuous vacuum, if the cannula is unintentionally partially removed during aspiration around the incision sites, the vacuum will be lost. If this occurs, the air must be removed from the syringe before reuse.
When a mechanical suction system is used, the cannula is connected to a collection container through a tube. The tissue mobilized by the cannula is conveyed to the container by means of a collection system that uses negative pressure generated by a vacuum pump.40
STEP 7 - Sutures:
Profuse irrigation with saline and meticulous hemostasis should be performed at the end of the procedure. Subsequently, the surgical incisions can be closed.
Anchorage sutures can to be used in the areas treated with aggressive liposuction and curettage in order to prevent hematoma formation. 26
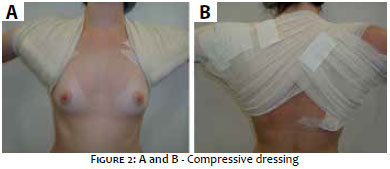
STEP 8 - Compressive dressing:
Large compressive dressings must be used for 2-3 days after the procedure to prevent hematoma and seroma formation (Figures 2A and B).
Prophylactic antibiotic treatment can be performed preoperatively14, and the dressing can be carried out with antibiotic ointment.36
Local measures for the prevention and improvement of the subcutaneous fibrosis (local heat, massage, gels or ointments containing heparin or flavonoids) can be introduced 3 weeks after surgery and should be maintained for three months.16
Patients should be instructed to avoid sudden movements with the arms (especially abduction and elevation movements) for 2 weeks. Intense physical exercise should be avoided for 1 month.24
Surgeons should perform the procedure with a view to achieve the best results, with the fewest possible side effects.
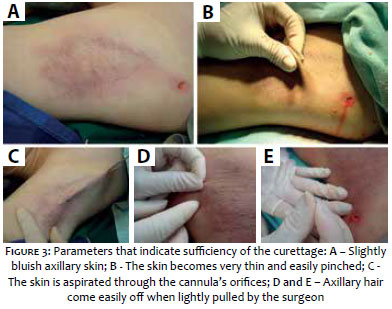
Clinical evidence indicating curettage sufficiency:
1. Complete elevation of the axillary skin regarding the subcutaneous tissue.21
2. Color of the overlaying skin: slight paleness of axillary skin (it becomes slightly bluish or pale, with some petechiae, indicating significant damage to the dermal vascular plexus) (Figure 3).6,21,24
3. Skin thickness: the skin becomes very thin and easy to pinch, as it if were a piece of clothing (Figure 3B).6,24
4. "Skin with skin" contact: indicates that there is no more fat adhered to the dermis (Figure 3B).21
5. Hair follicles are palpable during the "skin with skin" contact.21
6. The skin can be seen through the cannula's orifices while being aspirated (Figure 3C).24
7. "Suction sounds" caused by the cannula due to the axillary "cavity", indicating complete dissection of the dermis and subcutaneous tissue. 21
8. Axillary hair easily coming off when pulled by the surgeon. For this reason, the axillary hair should have a length of 2 to 4mm before surgery (Figures 3D and E).27
Despite the fact that minimally invasive techniques have demonstrated a relatively low rate of complications, several light to moderate side effects (most of them transient) have been described. 45 Possible complications include: hematoma, ecchymosis, seroma, superficial cutaneous erosions, loss of local sensitivity, skin necrosis, infection, epidermal inclusion cysts, reduction in the number of hairs, fibrosis, adhesion formation in the subcutaneous, scarring and recurrence of hyperhidrosis.46,47
Axillary hyperhidrosis is a disabling and distressing condition. Curettage is effective and can significantly improve the patients' quality of life.48
During the first two weeks after surgery, sweating usually stops completely, later rearising at a new individual level.49
Given that the removal of all sweat glands is unfeasible, a positive outcome occurs when patients are able to control their transpiration using conventional antiperspirants and deodorants.32
Although the technique in question is usually very effective and curative, patients not fully satisfied can be re-operated using the same method. This is almost invariably done with success.
Likewise, in case of recurrence (insufficient curettage, anatomical variations with great concentrations of sweat glands in the upper reticular dermis, compensatory hyperfunction of the remaining sweat glands, curettage performed in the wrong anatomical layer), curettage can be repeated with effective results, without causing an increase in the occurrence of serious complications.41
Aspiration curettage or simple curettage of the sweat glands is a minimally invasive surgical technique that is safe and easy to perform, offering high success rates and few side effects.47
1. Collin J, Whatling P. Treating hyperhidrosis. Surgery and botulinum toxin are treatments of choice in severe cases. BMJ. 2000;320(7244):1221-2.
2. Naumann M, Hamm H. Treatment of axillary hyperhidrosis. Br J Surg.2002;89(3):259-61.
3. Hurley HJ, Shelley WB. A simple surgical approach to the management of axillary hyperhidrosis. JAMA. 1963;186(2):109-12.
4. Tipton JB. Axillary hyperhidrosis and its surgical treatment. Plast Reconstr Surg. 1968;42(2):137-40.
5. Bisbal J, del Cacho C, Casalots J. Surgical treatment of axillary hyperhidrosis. Ann Plast Surg. 1987;18(5):429-36.
6. Weaver PC. Axillary hyperhidrosis. Br Med J. 1970;1(5687):48.
7. Hurley HJ, Shelley WB. Axillary hyperhidrosis. Clinical features and local surgical management. Br J Dermatol. 1966;78(2): 127-40.
8. Skoog T, Thyresson N. Hyperhidrosis of of the axillae. A method of surgical treatment. Acta Chir Scand. 1962;124:531-8.
9. Jemec B. Abrasio axillae in hyperhidrosis. Scand J Plast Reconstr Surg. 1975; 9(1): 44-6.
10. Darabaneau S, Darabaneau HA, Niederberger U, Russo PAJ, Lischner S, Hauschild A. Long-term efficacy of subcutaneous sweat gland suction curettage for axillary hyperhidrosis: a prospective gravimetrically controlled study. Dermatol Surg. 2008; 34(9):1170-7
11. Kim WO, Song Y, Kil HK, Yoon KB, Yoon DM. Suction-curettage with combination of two different cannulae in the treatment of axillary osmidrosis and hyperhidrosis. J Eur Acad Dermatol Venereol. 2008;22(9):1083-8.
12. Rho NK, Shin JH, Jung CW, Park BS, Lee YT, Nam JH, Kim WS. Effects of quilting sutures on hematoma formation after liposuction with dermal curettage for treatment of axillary hyperhidrosis: a randomized clinical trial. Dermatol Surg. 2008;34(8):1010-5.
13. Boni R. Tumescent suction curettage in the treatment of axillary hyperidrosis: experience in 63 patientes. Dermatology. 2006;213(3):215-7.
14. Bechara FG, Sand M, Sand D, Altmeyer P, Hoffmann K. Surgical treatment of axillary hyperidrosis: a study comparing liposuction cannulas with a suction-curettage cannula. Ann Plast Surg. 2006;56(6):654-7.
15. Tronstad C, Helsing P, Tønseth KA, Grimnes S, Krogstad AL. Tumescent suction curettage vs. curettage only for treatment of axillary hyperhidrosis evaluated by subjective and new objective methods. Acta Derm Venereol. 2014;94(2):215-20.
16. Feldmeyer L, Bogdan I, Moser A, Specker R, Kamarashev J, French LE, Läuchli S. Short- and long-term efficacy and mechanism of action of tumescent suction curettage for axillary hyprehidrosisJ Eur Acad Dermatol Venereol. 2015;29(10):1933-7.
17. Rompel R, Scholz S. Subcutaneous curettage vs. injection of botulinum toxin A for treatment of axillary hyperhidrosis. J Eur Acad Dermatol Venereol. 2001;15(3):207-11.
18. Jemec B, Holm Hansen B. Follow-up of patients operated on for axillary hyperhidrosis by subcutaneous curettage. Scand J Plast Reconstr Surg. 1978;12(1):65-7.
19. Lee MR, Ryman WJ. Liposuction for axillary hyperhidrosis. Australas J Dermatol. 2005;46(2):76-9.
20. Goldman A, Wollina U. Subdermal Nd-YAG laser for axillary hyperhidrosis. Dermatol Surg. 2008;34(6):756-62.
21. Lee HC, Chen CC, Lee WY, Chuang HU, Kao MC. Axillary hyperhidrosis and osmidrosis treated by ultrasonic surgical aspiration compared with transthoracic endoscopic sympathectomy. Surg Neurol. 2008;70(Suppl 1):64-8.
22. Commons GW, Lim AF. Treatment of axillary hyperhidrosis/bromidrosis using VASER ultrassound. Aesth Plast Surg. 2009;33(3):312-23.
23. Kim IH, Seo SL, Oh CH. Minimally invasive surgery for axillary osmidrosis: combined operation with CO2 laser and subcutaneous tissue remover. Dermatol Surg.1999;25:875-9.
24. Bechara FG, Tomi NS, Boorboor P, Sand M, Altmeyer P, Hoffmann K. Liposuction curettage for axillary hyperhidrosis: enhancing success rates and quantifying its efficacy. Dermatology. 2007;215(3):268-9.
25. Bechara FG, Sand M, Stucker M, Georgas D, Hoffmann K, Altmeyer P. Laser Doppler scanning study of axillary skin before and after liposuction curettage in patients with focal hyperhidrosis. Dermatology. 2008;216(2):173-9.
26. Rho NK, Shin JH, Jung CW, Park BS, Lee YT, Nam JH, Kim WS. Effects of quilting sutures on hematoma formation after liposuction with dermal curettage for treatment of axillary hyperhidrosis: a randomized clinical trial. Dermatol Surg. 2008;34(8):1010-5.
27. Chern E, Yau D, Chuang FC, Wu WM. Arthroscopic shaver with refinement for xillary osmidrosis. Int J Dermatol. 2010;49(7):813-7.
28. Arneja JS, Hayakawa TE, Singh GB, Murray KA, Turner RB, Ross LL, et al. Axillary hyperhidrosis: a 5-year review of treatment efficacy and recurrence rates using a new arthroscopic shaver technique. Plast Reconstr Surg. 2007;119(2):562-7.
29. Ong WC, Lim TC, Lim J, Leow M, Lee SJ. Suction-curettage: treatment for axillary hyperhidrosis and hidradenitis. Plast Reconstr Surg. 2003;111(2):958-9.
30. 30. Lee D, Cho SH, Kim YC, Park JH, Lee SS, Park SW. Tumescent liposuction with dermal curettage for treatment of axillary osmidrosis and hyperhidrosis. Dermatol Surg. 2006;32(4):505-11.
31. Bechara FG, Sand M, Hoffmann K, Boorboor P, Altmeyer P, Stuecker M. Histological and clinical findings in different surgical strategies for focal axillary hyperidrosis. Dermatol Surg. 2008;34(8):1001-9.
32. Swinehart JM. Treatment of axillary hyperhidrosis: combination of the starch-iodine test with the tumescent liposuction technique. Dermatol Surg. 2000;26(4):392-6.
33. Wollina U, Kostler E, Schonlebe J, Haroske G. Tumescent suction curettage versus minimal skin resection with subcutaneous curettage of sweat glands in axillary hyperhidrosis. Dermatol Surg. 2008;34(5):709-16.
34. Brewer JD, Roenigk RK. Anestesia tumescente: tecnica auxiliar para excisões extensas em cirurgia dermatologica. Surg Cosmet Dermatol. 2010;2(2):140-3.
35. Wu WH. Ablation of apocrine glands with the use of a suction-assisted cartilage shaver for treatment of axillary osmidrosis: annalysis of 156 cases. Ann Plast Surg. 2009;62(3):278-83.
36. Bieniek A, Białynicki-Birula R, Baran W, Kuniewska B, Okulewicz-Gojlik D, Szepietowski JC. Surgical treatment of axillary hyperhidrosis with liposuction equipment: risks and benefits. Acta Dermatovenerol Croat. 2005;13(4):212-8.
37. Qian JG, Wang XJ. Radical treatment of axillary osmidrosis by subdermal excision of apocrine glands: a prospective study in 31 cases. J Plast Reconstr Aesthet Surg. 2006;59(8):860-4.
38. Ou LF, Yan RS, Chen IC, Tang YW. Treatment of axillary bromhidrosis with superficial liposuction. Plast Reconstr Surg. 1998;102(5):1479-85.
39. Grazer FM. A noninvasive surgical treatment of axillary hyperhidrosis. Clin Dermatol. 1992;10(3):357-64.
40. Beer GM, Baumuller S, Zech N, Wyss P, Strasser D, Varga Z, et al. Immunohistochemical differentiation and localization analysis of sweat glands in the adult human axilla. Plast Reconstr Surg. 2006;117(6):2043-9.
41. Bechara FG, Sand M, Tomi NS, Altmeyer P, Hoffmann K. Repeat liposuction- curettage treatment of axillary hyperhidrosis is safe and effective. Br J Dermatol. 2007;157(4):739-43.
42. Bechara FG, Sand M, Sand D, Altmeyer P, Hoffmann K. Bilateral seroma after suction-curettage for axillary hyperhidrosis in a transaxillary breast- augmented patient. Dermatol Surg. 2007;33(6):731-3.
43. Field LM. Letter: Re: Insufficient Aggressiveness with Tumescent Suction Curettage. Dermatol Surg. 2009;35(3):555-6.
44. Seo SH, Jang BS, Oh CK, Kwon KS, Kim MBJ. Tumescent superficial liposuction with curettage for treatment of axillary bromhidrosis. J Eur Acad Dermatol Venereol. 2008;22(1):30-5.
45. Liu Q, Zhou Q, Song Y, Yang S, Zheng J, Ding Z. Surgical subcision as a cost-effective and minimally invasive treatment for axillary osmidrosis. J Cosmet Dermatol. 2010;9(1):44-9.
46. Bechara FG, Sand M, Rotterdam S, Altmeyer P, Hoffmann K. Multiple epidermal inclusion cysts after axillary liposuction-curettage: a rare complication of a frequent procedure. Int J Dermatol. 2008;47(11):1197-8.
47. Maffra de Rezende R, Luz FB. Surgical treatment of axillary hyperhidrosis by suction-curettage of sweat glands. An Bras Dermatol. 2014;89(6):940-54.
48. Bechara FG, Gambichler T, Bader A, Sand M, Altmeyer P, Hoffmann K. Assessment of quality of life in patients with primary axillary hyperhidrosis before and after suction- curettage. J Am Acad Dermatol. 2007;57(2):207-12.
49. Proebstle TM, Schneiders V, Knop J. Gravimetrically controlled efficacy of subcorial curettage: a prospective study for treatment of axillary hyperhidrosis. Dermatol Surg. 2002;28(11):1022-6.
The present study was carried out at Universidade Federal Fluminense (UFF) - Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}