


Bárbara Nader Vasconcelos1; Jaqueline Barbeito de Vasconcellos2; João Carlos Macedo Fonseca3; Carla R Fonseca4
Introduction: Rhinophyma is the final stage of rosacea. It leads to the stigmatization of the patient.
Objective: To establish the safety and efficacy of dermachemabrasion in the treatment of rhinophyma.
Methods: The method, which consists of tangential excision and dermabrasion with sandpaper followed by 30% trichloroacetic acid on the previously sanded area, was prospectively applied in 7 patients. The excised material was histologically studied aiming at detecting hidden neoplasias. Safety and efficacy were evaluated clinically and through standardized photographic records.
Results: The patients' ages ranged from 57 to 68 years (6 men, 1 woman). The complete reepithelialization occurred within 7 to 14 days. The 7 patients progressed without infection, with satisfactory reepithelialization and results from the aesthetic point of view, with absence of dyschromias or scarring. The histological analysis revealed the presence of a hidden neoplasia (superficial basal cell carcinoma) in one case.
Conclusion: Dermachemabrasion is a low cost, simple to execute and effective treatment that leads to excellent cosmetic results in addition to having the advantage of the possibility of histological analysis, which is extremely important, since there are reports of hidden malignancy in rhinophyma.
Keywords: RHINOPHYMA; TREATMENT OUTCOME; DERMABRASION; TRICHLOROACETIC ACID
The rhinophyma term comes from the Greek "growth of the nose." It is considered the final stage of rosacea even though only a minority of patients develops into that stage. It arises as a chronic inflammation with long development, usually of years.1, 2
It is clinically characterized by a globose nose with irregular exophytic growths, due to the progressive increase of connective tissue, hyperplasia of the sebaceous glands and vascular ectasia. The most affected population is that of men over 40 years of age, with a frequency of 5:1 regarding women.1, 2
The picture often leads to stigmatization of the patient, interfering in their personal and professional lives.
Furthermore, there are reports in the literature of hidden neoplasias associated with rhinophyma. It is estimated that hidden basal cell carcinomas occur in a percentage ranging from 3% to 10% in cases of rhinophyma, while other types of skin cancers, including cutaneous metastases, have also been found simulating rhinophyma.3,4, The development time of rhinophyma seems to be closely associated with a higher risk of developing malignancy location.4
Among the various treatments described in the literature, the use of 90% trichloroacetic acid (TCA), dermabrasion, shaving associated with dermabrasion, cryosurgery and CO2 laser stand out.5 There are reports of the use of high frequency devices (radio frequency) for the treatment of rhinophyma with good results and short recovery time, however this method has the disadvantage of not allowing histologic evaluation.6 There is also a study describing 28 patients who underwent the association of decortication/dermabrasion with electrocoagulation.7
The term chemabrasion was described by Stagnone,8 in 1977 and consists in performing medium chemical peeling with Jessner's solution and 20% to 35% TCA applied across the face and upper third of the cervical region, followed by dermabrasion with diamond fraises. The purpose of this procedure is to reduce the skin's resistance and minimize demarcation lines in areas that will not be abraded.9
The objective of the present study was to establish the safety and efficacy of a new combination of methods for treating rhinophyma, called dermochemabrasion, which consists in tangential excision and dermabrasion with sandpaper followed by the use of 30% TCA on the area previously abraded.
In this prospective, single-center study 7 patients bearers of rhinophyma were treated with dermochemabrasion at the Corrective Dermatology Clinic of the Hospital Universitário Pedro Ernesto do Rio de Janeiro, from June 2010 to July 2014.
In compliance with the legal requirements, the procedures carried out in the present study were approved by the Clinical Studies and Research Committee of the institution where it was performed, with involved patients having signed the free and informed term of consent. Patients were instructed to avoid the use of medications such as aspirin, ginkgo biloba and vitamin E in the preoperative period, and that comorbidities such as systemic arterial hypertension and diabetes be controlled.
Dermochemabrasion: steps of the surgical technique
After asepsis and antisepsis, anesthetic blocks were performed of the infraorbital nerves (in the paranasal areas), infratrochlear nerves (in the base of the nose, below the glabella and close to the inner canthus) and nasociliary nerves (at the junction of cartilage and bone in the dorsum of the nose).1, 2 The anesthetic blocks were properly complemented by infiltrative anesthesia with 1% lidocaine and 1:100,000 epinephrine.
The first surgical step consisted in the tangential excision (shave) with number 15 scalpel blade. Thin layers were removed from the hyperplastic tissue up until the symmetry and nose contour were reconstructed. The material excised from all patients was sent for histology for detection of hidden neoplasias. Next, manual abrasion with number 100 wet sandpaper was carried out aiming at leveling the tissues. The final step was the chemical cauterization of the abraded area with 30% TCA to obtain coagulation and hemostasis of the surgical wound (Figure 1).
The dressing was prepared in the following order: topical antibiotic, PVC plastic film, gauze and medical tape. The plastic film acts blocking the nerve endings, controlling the postoperative pain. Patients were instructed to perform the daily re-application of the bandage for a week. After this period, sunscreen should be used daily up until the erythema disappeared, with the skin color returning to natural.
In order to evaluate the safety and efficacy of this therapeutic proposal, clinical evaluations and standardized photographic records were performed before and at 7, 14, 30 and 120 days after the procedure. The three first records were aimed at evaluating the duration of the re-epithelialization period and the presence of infections. One hundred and twenty days after, the patients returned to control the final outcome. The skin's thickness in the treated areas, the presence of large pores, the evenness of the cutaneous relief and the presence of dyschromias and scars were assessed on this visit.
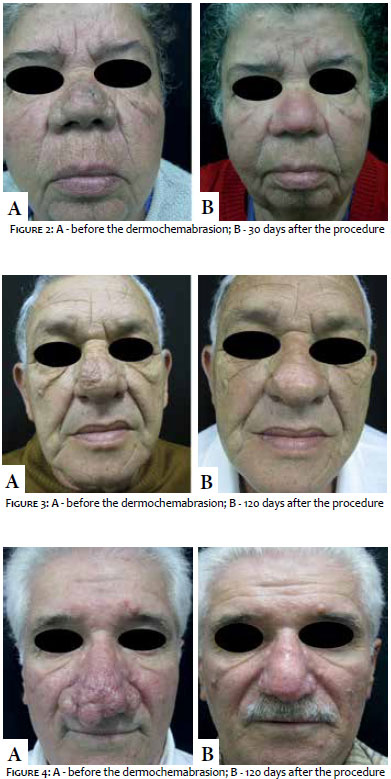
The patients' ages ranged from 57 to 68 years (6 men, 1 woman / Fitzpatrick phototypes III and IV). Complete reepithelialization occurred between 7 and 14 days. All patients progressed with absence of infections, satisfactory reepithelialization and resolution of exophytic tissues (Figures 2 to 4). Therefore, all patients obtained satisfactory final outcomes from the aesthetic point of view, with absence of dyschromias or scarring. In 6 of the cases described - except for one, where a superficial basal cell carcinoma was detected - the histology excluded hidden cutaneous neoplasias.
Rhinophyma is a stigmatizing condition. Different surgical treatments have been described in the literature, however there is no consensus on the best technique. Today there are multiple therapies published for the treatment of rhinophyma aimed at restoring the normal appearance of the nose.
Radioelectrosurgery has been widely used, and specific electrodes have been developed to treat this condition. Its advantage is the possibility to simultaneously remove tissue and control the bleeding, offering enough comfort to the surgeon.6
In 2014, an innovative and simple to implement technique was described to treat this condition exclusively using high concentrations of TCA.10 However, the greatest advantage of the technique is the possibility of histological examination of the removed material, which also allows the diagnosis of benign or malignant tumors hidden in the exophytic tissue that is characteristic of rhinophyma. The procedure also allows visual control of the planes to be reached, whose limit lies between the medium reticular and deep dermis. This protects the base of the cutaneous appendages, thus preventing scarring, lending safety and effectiveness to the technique.
Dermochemabrasion is a treatment characterized by its effectiveness, low cost, straightforward implementation and excellent cosmetic outcome, in addition to the advantage of allowing histologic analysis - the latter being of great importance, since there are cases of hidden neoplasia in rhinophyma described in the literature.3, 4
1. Silva SCMC. Rinofima. In: Kede MPV, Sabatovich O. Dermatologia Estética. 2ª ed. São Paulo: Atheneu; 2009. p. 198-201.
2. Popa D, Osman G, Parvanescu H, Ciurea R, Ciurea M. The treatment of giant rhinophyma-case report. Curr Health Sci J. 2012;38(1):41-4.
3. Rohrich RJ, Griffin JR, Adams WP. Rhinophyma: review and update. Plast Reconstr Surg.2002;110(3):860-9
4. Lutz ME, Otley CC. Rhinophyma and Coexisting Occult Skin Cancers. Dermatol. Surg. 2001;27(2):201-2.
5. Silva SCMC. Cirurgia Dermatológica Teoria e Prática. Rio de Janeiro: Dilivros; 2008. p. 285-90.
6. Sperli ED, Freitas JOG, Fischler R. Rinofima:tratamento com equipamento de alta frequência Rev Bras Cir Plast. 2009; 24(4): 504-8.
7. Costa TC, Firme WAA, Brito LMR, Vieira MBG, Leite LAS. Rinofima: opções cirúrgicas utilizadas no Serviço de Cirurgia Plástica do Hospital Agamenon Magalhães - PE. Rev. Bras. Cir. Plást.2010; 25(4): 633-6.
8. Stagnone JJ. Chemabrasion, a combined technique of chemical peeling and dremabrasion. J. Dermatol. Surg Oncol 1977;3(2):217-9.
9. Meski AP, Cucé LC. Quimioabrasão para tratamento de rugas periorais: avaliação clínica e quantificação das células de langerhans epidérmicas. Surg Cosmet Dermatol. 2009;1(2):74-9.
10. Gaspar NK, Gaspar APA, Aidê MK. Rinofima: tratamento prático e seguro com ácido triclcoroacético. Surg Cosmet Dermatol. 2014;6(4):368-72.
This study was performed at the Corrective Dermatology Clinic, Hospital Universitário Pedro Ernesto of the Universidade do Estado do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}