


Luciana Imaculada de Faria Melo1; Myrian de Faria Melo2; Maria Christina Marques Nogueira Castañon3
Basal cell carcinoma is the most common type of cancer and its non-surgical treatment has been the subject of many studies. Large lesions of this tumor are therapeutic challenges and the effective topical treatment has good applicability. The authors present a female patient diagnosed with multicentric superficial basal cell carcinoma in the lumbar region for more than 20 years, who refused to be treated surgically. The tumor reached dimensions of 12 cm x 10 cm. A decision was made for a non-surgical therapy, with the application of Imiquimod in a treatment of 5 weekly applications for 2 months. The treatment led to a clinical and histological cure, without recurrence to date (36 months), with excellent aesthetic results and few side effects.
Keywords: CARCINOMA, BASAL CELL; THERAPEUTICS; NEOPLASMS
Basal cell carcinoma (BCC) is the most frequent malignant neoplasia throughout the world 1 and corresponds to ¾ of all skin cancers. 2 It is a slow growing tumor with rare probability of metastasis, allowing non-surgical therapies in cases of low-aggressiveness, which is determined by clinical and histological characteristics. The treatment is aimed at completely eradicating the tumor, with good aesthetical results, preventing recurrences and improving the quality of life of millions of patients who are positively diagnosed every year. Treatments recognized as alternative to surgery are: radiotherapy, photodynamic therapy, cryotherapy and the topical 5% 5-fluorouracil, 3% diclofenac, 0.015% -0.05% ingenol mebutate and 5% imiquimod.
Imiquimod acts modifying the biological response via induction of cytokines, making the immune system to recognize tumor cells as antigens, eradicating them. It is an approved medicament by the US regulatory agency Food and Drug Administration (FDA) for the treatment of superficial BCC. The most commonly used regimen is 5 weekly applications for 6 weeks. Double-blind randomized multicenter studies carried out aimed at comparing schemes of 5 versus 7 weekly applications have shown conflicting results. As a result, the dosage can be chosen based on tolerance to adverse effects, with the scheme with fewer weekly applications being advantageous.2, 3
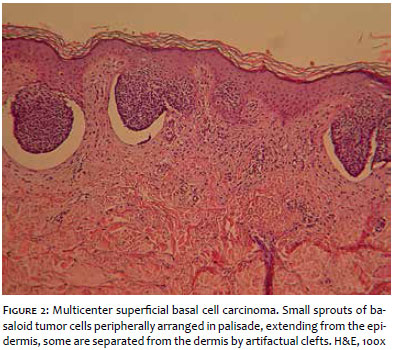
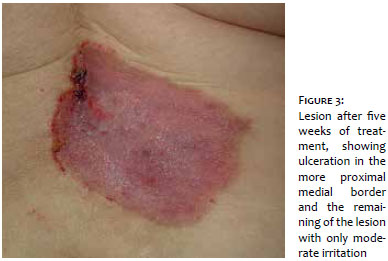
A sixty-nine year-old Caucasian female patient sought care at the Dermatology Department of the Universidade Federal de Juiz de Fora (UFJF), Minas Gerais, Brazil, in 2011, presenting an asymptomatic, erythematous, scaly and crusted lesion in the shape of a plaque, with well defined borders, located in the right lower back, measuring 12cm x10cm, with roughly 20 years of development (Figure 1). The patient was diagnosed with skin cancer (not specified by the patient) in 1989, nevertheless the authors did not have access to that histology. On that occasion, the patient refused the proposed surgery for a still nummular lesion. In December 2011, she sought the mentioned service with complaints related to the lesion and occasional small bleedings. In this manner, with the diagnostic hypothesis of Bowen's disease and BCC, an incisional biopsy was indicated, which defined the diagnosis of multicentric superficial BCC (Figure 2). In face of the diagnosis and taking into consideration the lesion's size and the patient's resistance to surgery, a decision was made for the treatment with imiquimod (Intendis do Brasil Farmacêutica Ltda., Itapevi, SP, Brasil), following the five weekly applications scheme. After five weeks of use, the first clinical review was carried out, when an ulceration on the more proximal medial border was observed, however a larger portion of the lesion was only moderately irritated (Figure 3). The authors indicated the continuation of the treatment, prolonging the use to 8 weeks - and not the 6 recommended by the literature - based on the good tolerance and aiming at increasing the effectiveness, given that the lesion's size exceeded those of the reports researched at that time. The treatment was suspended after two months, with biopsies of various skin fragments having been later performed, with negative results for neoplasm (Figure 4). A quarterly follow-up examination has already been in place for 36 months, without suspicious clinical lesions, and the increasing improvement of the initial appearance of the scar (Figure 5).
The treatment of BCC is aimed at the complete eradication of the tumor in a way to prevent recurrences and obtain good aesthetic result, improving the patients' quality of life. It is known that recurrent tumors can be more aggressive than the primary lesion. Factors associated with greater recurrence are: histological type (sclerodermiform, infiltrative, micronodular, baso-squamous), large dimensions, involvement of deep levels, location (centrofacial, nose, ears and scalp), poorly defined borders and perineural and/or perivascular involvement.3 Surgery is the gold standard treatment, with less chance of recurrence. Nonsurgical treatments are indicated when clinical conditions are unfavorable to the surgery or when this method may result in large unsightly scars and/or functional damage, or even when there is patient refusal. Since 2004, the treatment with imiquimod, alternative to surgery, is well indicated for immunocompetent patients with superficial lesions in the trunk, neck or extremities (excluding hands and feet), and when the periodic follow-up is assured.4,5 Complete regression is reported in 83% of patients treated with imiquimod in lesions with over 2cm in diameter.3
The patient described in the present paper refused undergoing any surgery of the large BCC with clinical and histological characteristics of weak aggressiveness that she was bearing, therefore with good indication for treatment alternative to surgery. The use of imiquimod was started in January 2012, with 5 weekly applications, and due to good tolerability its use was extended to 8 weeks, as it was a lesion with dimensions larger than those described in the literature up until then. Clinical and histological results were excellent, with total regression of the lesion and excellent aesthetic results. The patient has been followed up on a quarterly basis without recurrences, completing three years without the lesion (Figures 4 and 5).
1. Gaitanis G, Bassukas ID. Immunocryosurgery for Non-superficial Basal Cell Carcinoma: A Prospective, Open-label Phase III Study for Tumors < 2 cm in Diameter. Acta Derm Venereol. 2014; 94(1): 38-44.
2. Enokihara MY, Simões MM, Enokihara S. Carcinoma Basocelular e Carcinoma Espinocelular. Rotinas de Diagnóstico e Tratamento da Sociedade Brasileira de Dermatologia. 2010. p. 29-34.
3. Goldenberg G, Hamid O. Nonsurgical Treatment Options for Basal Cell Carcinoma - Focus on Advanced Disease. J Drugs Dermatol. 2013;12(12):1371-8.
4. Botto N, Rogers G. Nontradicional management of basal cell carcinoma. J Drugs Dermatol. 2013;12(5):525-32.
5. Aldara Cream [package insert]; Bristol, TN: Graceway Pharmaceuticals, LLC; 2010. Acessado em: 15 abril 2015. Disponível em: www.accessdata.fda.gov/drugsatfda_docs/label/2010/020723s022lbl.pdf.
The present study was conducted at the Universidade Federal de Juiz de Fora (ICB UFJF) - Juiz de Fora (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}