


Ana Luísa Chaves de Olveira1; Fátima Maria de Oliveira Rabay2; Beatriz Lopes Ferraz Elias3; Márcia Lanzoni de Alvarenga Lira4; Samuel Henrique Mandelbaum5
The authors describe the case of a 54-year-old woman presenting papules and yellowish plaques on the right thigh for 15 years, which clinically resembled a plane xanthoma. An anatomical pathological examination evidenced a mature adipose tissue in the dermis, with a diagnosis of superficial cutaneous lipomatous nevus, a rare benign hamartomatous malformation characterized by the presence of ectopic mature adipocytes in the dermis.
Keywords: NEVUS; ADIPOCYTES; XANTHOMATOSIS
Superficial cutaneous lipomatous nevus (SCLN) was first described by Hoffman and Zurrhelle in 1921.1-4 The first Brazilian case was described in 1984 in a four-year-old child with lesions located on the left wrist.2 This condition is characterized by the ectopic presence of mature adipocytes in the dermis.
Case report
A 54-year-old white female patient, a cook by profession, born and raised in the city of Taubaté (São Paulo State), with complaints of "patches on the thigh for 15 years" was treated at the Dermatology Department of the Universidade de Taubaté (SP), Brazil. She stated that the lesions increased during this period and were accompanied by associated pruritus. There was a past medical history of dyslipidemia, treated with statins.
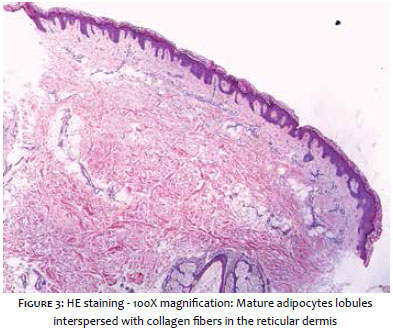
The dermatological examination revealed yellow papules, some of them grouped in a way that formed plaques on the lateral face of the right thigh (Figures 1 and 2). A biopsy of one of these lesions was carried out with pathology results showing lobules of mature adipocytes interspersed with collagen fibers in the reticular dermis, with an absence of xanthomatous histiocytes (Figure 3).
In light of the clinical and pathological findings, the diagnosis of SCLN was confirmed. The patient decided not to have her dermatosis treated.
There are two distinct clinical forms of SCLN: the multiple form (or classic Hoffman-Zurhelle form) and the papule or solitary nodule form. The classic SCLN consists of multiple soft, yellow or skin colored papules and nodules, which often coalesce or group and form plaques with segmented distribution, located commonly in the gluteus, lower dorsum, and upper thighs. There is no definitive explanation for this apparent predominance in the pelvic girdle region. 5, 6 In the present case, the patient had the characteristics of the classic clinical subtype. Some authors consider an extremely rare third clinical form, known as Michelin baby syndrome. 6-8
The classic form is usually present at birth or develops during the first two decades of life7 and even in the third,1,8 as in the present case. There appears to be no greater occurrence in either gender 1,5 nor is there evidence of a familial tendency.1 It affects all races.8
The differential diagnosis includes, among other possibilities, connective tissue nevus, epidermal nevus, lipoma, fibrolipoma, eccrine cells tumor, neurofibromas, elastic tissue nevi, lipoblastomosis, sebaceous nevus, and focal dermal hypoplasia. 1,8
The pathogenesis of this entity is unknown. One theory suggests that precursor cells around dermal blood vessels give rise to mature adipose cells in the dermis,1,5 arranged among collagen fibers, without connection to the hypodermis and that histologically characterize the SCLN lesions, 5 which are essential for confirming the diagnosis.
The treatment of choice is adequate surgical excision, in order to avoid recurrences.5 It is indicated due to esthetical reasons,1,7 for there have not been reports of malignancy to date.1 The multiple SCLN form, however, usually affects large areas, requiring skin grafts, which could cause unsatisfactory aesthetic results, unlike those treated with CO2 laser. 5 Nevertheless and despite the effectiveness of the latter, there have been reports of recurrence of classic SCLN after treatment with this method.5 There are reports of patients whose lesions were treated with cryotherapy, with a partial but satisfactory response.6 Our patient did not undergo treatment but remains in follow up care.
1. Ranjkesh MR, Herizchi QH, Yousefi N. Nevus lipomatosus cutaneous superficialis: a case report with histologic findings. J Turk Acad Dermatol 2009;3(1): 93103c
2. Festa Neto C, Iamaguchi T, Cucê LC. Nevo lipomatoso cutâneo superficial. Um caso de localização insólita. An bras Dermatol 1984;59(2):93-6.
3. Monteiro CM, Martins CJ, Machado MGV. Nevo lipomatoso cutâneo superficial. An bras Dermatol 1994;69(4):333-4.
4. Almeida Jr. HL, Gevehr D, Pinto IO. Nevo lipomatoso superficial de aparecimento tardio. An bras Dermatol 1999;74(6):601-3.
5. Kim YJ, Choi H, Kim H, Nam SH, Choi YW. Recurrence of nevus lipomatosus cutaneous superficialis after CO2 laser treatment. Arch Plast Surg 2012;39(6): 671-3.
6. Al-Mutairi N, Joshi A, Nour-Eldin O. Naevus lipomatosus cutaneous superficialis of Hoffmann-Zurhelle with angiokeratoma of Fordyce. Acta Derm Venereol 2006;86:92-3.
7. Pathirana PW, Ranasinghe A, Perera WMT. Nevus lipomatosus cutaneous superficialis: an unusual presentation. Journal of Diagnostic Pathology 2013;8(1):59-62.
8. Zaragozano JF, López JM, Jordán MPG, Pericas VD, López JLO. Nevo lipomatoso cutáneo superficial. Acta Pediatr Esp. 2007;65(8):413-15.
This study was carried out at the Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}