


Violeta Duarte Tortelly Costa1; Monica Jidid Mateus Tarazona2; Tassiana Esposito Simão3; Bruno Eduardo Nunes Moraes4; Fabiano Gualtiero Portugal5; Roberto Souto da Silva6; João Carlos Fonseca7
Description of a case where a female patient who received facial filling with polymethylmethacrylate developed late formation of a nodule and ipsilateral trigeminal neuralgia. The authors question whether there is a possible link between the two morbidities, which could have a common triggering factor or a causal relationship with each other.
Keywords: GRANULOMA; POLYMETHYLMETHACRYLATE; TRIGEMINAL NEURALGIA
Currently, there is a steady worldwide growth in the demand for aesthetic procedures. Recent indices prepared by the American Society for Aesthetic Plastic Surgery show that in the United States, more than 9.5 million non-surgical cosmetic procedures have been performed, including cutaneous filling procedures. 1 The diversity of options currently available, the products' strong safety profiles, and the fear of invasive surgeries, all linked to the present cult of beauty, are the main drivers for the growth of these ambulatorial procedures. As a result, the side effects inherent to the material used or poor technique have become more frequent - especially those regarding permanent products.2 The present paper describes the case of a patient who received facial filling with polymethylmethacrylate (PMMA) and evolved with nodule formation and ipsilateral trigeminal neuralgia.
Clinical case
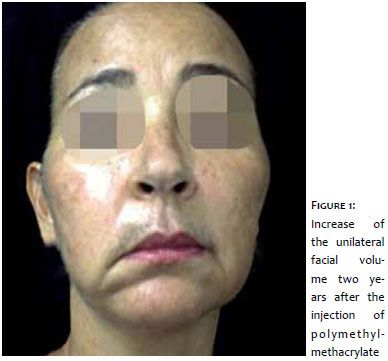
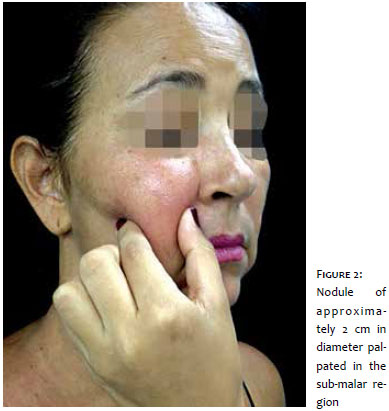
A 47-year-old female patient described having a paroxysmal and excruciating pain in the right hemiface for three years. While being followed up with by the Neurology Clinic, the patient has undergone MRI and electroneuromyography, which did not evidence abnormalities. The serologies were negative, except for herpes virus type 1. She was also evaluated by the Odontology Department, which showed no dental alterations. As a result, the patient was diagnosed as bearing trigeminal neuralgia. During the last two years the patient has noticed swelling of the malar and perioral region - only the side of the neuralgia - that had progressively worsened over the past four months (Figure 1), when it became possible to palpate a regional nodule of approximately 2 cm in diameter (Figure 2). The patient informed that she had undergone a cutaneous filling procedure in the nasogenian groove and malar region with PMMA four years before. She underwent an ultrasound of soft tissues of the face, which revealed the presence of amorphous material in the region. Due to the patient's psychological stress, it was not possible to collect material for biopsy. Through clinical elements, current and prior history, and findings of the ultrasound, the diagnosis of foreign body granuloma to PMMA was inferred. The treatment started with 1 mg/kg/day prednisone, and 100 mg/day doxycycline with partial improvement in three weeks (Figure 3).
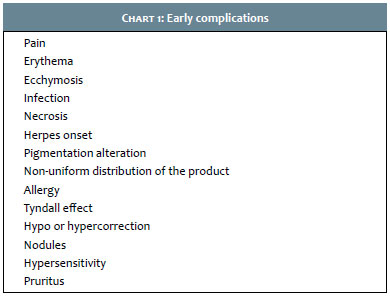
Permanent dermal fillers, more specifically the PMMA, have a low complication rate, varying from 0.01 - 3.00%. 3 However, due to the fact that the clinical picture is often deforming, complications are not easily accepted by the patient and can bring legal consequences for the physician. Adverse effects to filling substances can be classified into early and late onset. 4 Those linked to technical aspects, such as the injection plane, and improper amount, type and quality of material, can be avoided. Though usually mild and transient, acute effects are numerous and frequent (Chart 1). Among them it is necessary to emphasize the importance of bacterial infection - which can be severe. Relating mainly to contamination during the procedure, the most common are those caused by staphylococcus and streptococcus.5
The most feared complications are the late complications, including inflammatory (or not) nodules, mostly represented histologically by foreign body granulomas, which can be disfiguring and difficult to treat, while the patient many times is unaware of which product has been applied on the body site in question. They are often attributed to hypersensitivity phenomena, local infection, trauma, or drugs. The infections can be viral, with influenza having been reported in some cases. Those of mycobacterial origin are often caused by Mycobacterium furtuitum or Mycobacterium marinum; or still be the result of biofilm formation. The latter are constituted of bacteria in a dormant state that can be activated by external factors and whose structure protects them from antibiotics and host immune responses. These microorganisms are difficult to identify, which often can only be done by polymerase chain reaction. 5, 6 Interferon is among the described drugs.6 This type of reaction usually occurs after six months and may resolve spontaneously, nonetheless the approach rarely is expectant, given the patient's discomfort.
In the present case, the patient developed trigeminal neuralgia after a cutaneous filling procedure with PMMA, developing an ipsilateral nodule. This neuropathic pain is characterized for being excruciating and paroxysmal, and is observed in the distribution area of one or more branches of the trigeminal nerve. The pain is triggered by stimuli originating in the skin, mucosa, or teeth innervated by this cranial nerve. The right hand side is five times more likely to be affected, especially in the V2 and V3 branches (mandibular and maxillary). Its etiology is believed to be multifactorial and is not well established yet,7 and is academically divided into idiopathic and secondary. The latter is usually associated with tumors, multiple sclerosis, amyloidosis, herpes zoster, or skull base abnormalities.
The main hypothesis of the idiopathic form would be the contact of an artery with the nerve, causing a local lesion and subsequent hyperexcitability of nociceptive fibers, resulting in pain. Another hypothesis is the chronic presence of herpes virus 1, which would have as an underlying cause an ion channel disorder resulting from the activation of the latent HSV-1 genome in the nucleus of infected neurons in nociceptive trigeminal fibers. 8 In light of this etiology, the authors ask whether the herpes virus could also be acting as a re-activator of this granuloma, since there are reports of viral infections triggering the process. In this case, both disorders would have the same origins, without a cause and consequence correlation. However, the very normal initial inflammatory reaction arising from the PMMA would lead to the stimulation of the trigeminal fibers, causing neuropathic pain, which would later lead to chronic inflammation and formation of granulomas. The application of the filling substance in deeper planes - generally subcutaneously or supraperiosteally - can promote inflammation by contiguity, since the nerve has a mostly intrabony path, and can trigger an inflammatory cascade, culminating in neuropathic pain. It is impossible to prove these hypotheses, however there is a temporal association of the two conditions, corroborating the correlation.
As for treatments, there are some therapeutic options, including corticosteroids, delivered orally and via intralesional route.5, 9 5-fluorouracil (5FU) should be applied in association with corticosteroids, however with an aim of reducing the dose of the latter, consequently reducing the risk of atrophy. Nevertheless, there is the practical limitation of increased pain with injection. 5FU is a pyrimidine antagonist that would work with two active metabolites (5FdUMP, which interferes with the DNA synthesis, and 5FdUTP, which inhibits the synthesis of RNA and hence the collagen formation and proliferation). Allopurinol is also part of the therapeutic armamentarium, though while not yet fully explained, it seems to act as a catalyzer of superoxides or as a captor of free radicals. Tetracycline and its derivatives are good options due top their anti-inflammatory and immunomodulatory effects, and their antigranulomatous properties. There are also reports of the use of hydroxychloroquine, imiquimod, and cyclosporine. Surgery is an extreme option due to the fact that if the material is too dispersed, and there is the risk of scarring and fistulas. If possible, access via the mucosa should be chosen.
It is extremely important to bear in mind the possible side effects of cutaneous filling.10 A broad knowledge of the technique and anatomy, including anatomical variations, the quality and quantity of the used product, can help to avoid undesirable complications in the follow-up of these patients. Thus, a careful anamnesis covering other aesthetic procedures already performed, comorbidities, and drug use are necessary in the cosmiatry practice.
1. American Society for Aesthetic Plastic Surgery- Statistics, Surveys & Trends, www.surgery.org
2. Lemperle G. Complications from Artecoll are treatable. Aesthetic Surg J. 2003;23(6):469-70.
3. Conejo-Mir JS, Sanz Guirado S, Angel Muñoz M. Adverse granulomatous reaction to Artecoll treated by intralesional 5-fluorouracil and triamcinolone injections. Dermatol Surg. 2006;32(8):1079-81.
4. Lowe, N J, Maxwell, C A, Patnaik R. Adverse Reactions to Dermal Fillers: Review. Dermatol Surg. 2005;31(11 Pt 2):1616-25.
5. Alijotas-Reig j, Figueras-Fernandez MT, Puig L. Late-Onset inflammatory Adverse reactions Related of Soft tissue Filler Injections. Clin Rev Allergy Immunol. 2013;45(1):97-108.
6. Bringel DM, Bomm L, Azevedo AC, Souto R, Fonseca JC. Dermal filling complication after hepatitis C treatment with interferon and ribavirin. Surg Cosmet Dermatol. 2012;4(3):271-3.
7. Frizzo HM, Hasse PN, Veronese RM. Trigeminal Neuralgia: na analytic review of the literature. Rev Cir Traumatol Buco-Maxilo-Facial. 2004;4(4):204-57.
8. Ecker AD, Smith JE. Are Latent, Immediate-Early Genes of Herpes Simplex Virus 1 Essencial in Causing Trigeminal Neurlagia? Medical Hypotheses. 2002;59(5):603-6.
9. Boulle KD. Management of complications after implantation of fillers. J Cosmet Dermatol. 2004;3(1):2-15.
10. Crocco EI, Alves RO, Alessi C Eventos adversos do ácido hialurônico injetável. Surg Cosmet Dermatol. 2012;4(3):259-63
This study was carried out at Hospital Universitário Pedro Ernesto da Universidade do Estado do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}