


Beatriz de Medeiros Ribeiro1; Luiz Maurício Costa Almeida2; Adilson Costa3; Fábio Francesconi4; Ivonise Follador5; Juliane Rocio Neves6
Acne vulgaris is a very common dermatosis affecting the general population. Due to its prevalence, it is a much studied pathology. A number of studies on the subject are published on a yearly basis, including those on its pathogenesis. The present review aims at compiling the classically known etiopathogenic factors of acne vulgaris and introducing new concepts, such as the inflammatory nature of this condition. This new knowledge is crucial in the search for the best treatment option.
Keywords: ACNE VULGARIS; PROPIONIBACTERIUM ACNES; LINOLEIC ACID
Acne vulgaris is a chronic inflammatory, immune-mediated, and multifactorial skin disorder that affects the pilosebaceous unit and is characterized by a varied clinical picture.1
According to studies conducted in England, France, and the U. S.,2-4 it figures among the three most prevalent skin conditions affecting the general population.
Some degree of acne is present in virtually all teenagers between 15 and 17 years old.5-7 Rates of prevalence by age and data from the census conducted in 1996 in the U.S. estimated that 40 to 50 million individuals had acne in that country, with a prevalence rate of 85% in individuals between 12 and 24 years of age.8
Although it is considered a dermatosis that affects mostly adolescents, an increase was observed in the incidence in adults, especially in women.9
The concept currently in vogue is that acne results from the interaction of different pathogenic factors,10 namely follicular hyperkeratinization (leading to the formation of open and closed comedones), sebum hypersecretion (leading to excessive production of sebum, a hormonally determined condition), and changes in microbial flora in addition to immunological factors and inflammatory processes.11 These are primary pathogenic factors, however the precise influence of these elements and their interactions are still in question.12
They should not be viewed in isolation since they influence each other. The combination of seborrhea and follicular hyperkeratinization produces a favorable environment for the development of Propionibacterium acnes (P. acnes), which are found in the resident skin flora and are not pathogenic in normal circumstances.10, 13
Follicular hyperkeratinization
In normal follicles keratinocytes are detached in layers that peel off and are carried by the flow of sebum to the skin's surface. This process promotes a balance between the amount of cells that are shed and the production of new keratinocytes.10
Follicular hyperkeratinization results in the formation of a micro-comedo.11 It occurs via an abnormal keratinization process in the follicle infundibulum, with an increased production of follicular keratinocytes and alterations in the peeling process.14 An increase in the cohesion among corneocytes is also observed due to alterations in intra-structural cellular components responsible for the adhesion between cells and their accelerated production.12, 13
For this reason, the corneocytes, which would normally be disposed via the follicular ostium, are retained and initiate the hyperkeratosis process.14 This takes place in the proximal portion of the follicle infundibulum, which when obstructed, leads to the formation of a keratin stopper and a comedo.14 With the increase of the comedo, it is possible to verify an accumulation of detached corneocytes and sebum.14
Another important factor in the comedogenesis is the reduction of linoleic acid levels in the sebum, due to the sebaceous hypersecretion that takes place.11 Linoleic acid plays an important role in the maintenance function of the skin barrier.15 The alteration of this barrier facilitates the penetration of microorganisms and pro-inflammatory fatty acids in the dermis, leading to infection and inflammation.15 The more severe the acne, the lower the concentration of linoleic acid in the sebum.11, 15
P. acnes is also one of the factors responsible for comedo formation. It is capable of forming a biofilm, a protective barrier with antimicrobial function, which "glues" the corneocytes in the follicle infundibulum and intensifies the keratinization process, in addition it produces filaggrin protein, which increases the adhesion among the corneocytes.16, 17
Sebaceous hypersecretion
With rare exceptions (such as the "free" sebaceous glands in the genital region and some areas of mucous membranes), sebaceous glands are associated with hair follicles.10
Sebum is formed from the dissolution of sebocytes in the sebaceous lobules (holocrine secretion), being transported to the follicle by the sebaceous drain duct and reaching the skin surface via the infundibulum.10 The largest sebaceous glands are found in the face and upper trunk, regions where acne occurs preferentially.10
The sebaceous gland produces sebum rich in cholesterol, fatty acids, esters, triglycerides, and squalene.11 Its activity is regulated by androgens. An increase of sebum production can be detected after stimulation of the sebaceous gland by the action of these hormones.11 Patients with acne often show an increased production of sebum (seborrhea). On the other hand, eunuchs produce less sebum due to androgen deficiency and do not develop acne.10
Androgens have gonadal and adrenal origin, and can also be produced in the pilosebaceous unit.18, 19 Androstenedione and testosterone are produced in the ovaries. Dehydroepiandrosterone sulphate (DHEAS) and androstenedione are produced in the adrenal or suprarenal glands.18 In the pilosebaceous unit, there can be a peripheral conversion of androstenedione and DHEAS into testosterone.18 This production within the sebaceous gland occurs due to the action of enzymes such as 3-beta-hydroxysteroid dehydrogenase, 17-hydroxysteroid dehydrogenase and 5-alpha-reductase, which metabolize the circulating precursor androgens (DHEAS and androstenedione), transforming them into more potent androgens (testosterone and dihydrotestosterone). 18
There are receptors for androgen hormones located in sebaceous glands and the outer root sheath of the hair follicle. 11 These cellular structures respond to the action of testosterone and dihydrotestosterone, which stimulate the production of sebum.11 Sebum hypersecretion can occur due to increased production (ovarian, adrenal, or peripheral) of androgens, increased availability of free androgens, decreased sex hormone binding globulin (SHBG) or an increased sebaceous gland response to a hormonal stimulation.20 The increase in sebum production can occur with normal or elevated androgen levels.21 The elevation of androgens is observed in polycystic ovary syndrome, in the androgens producing tumors, and in congenital adrenal hyperplasia.21 There is also the possibility of exogenous administration of anabolic-androgenic steroids, found in patients who consume these products in order to increase muscle mass.16
Neuroendocrine effects in sebum production have been reported and could explain some psychogenic or stress-induced effects in the pathogenesis of acne.19 Among others, the neuropeptides, corticotropin-releasing hormone and α-melanocortin induce the in vitro synthesis of serum lipids in sebocytes.19 Acne patients have an increased expression of the substance P neuropeptide and neural endopeptidase around the sebaceous glands.19
Bacterial colonization
The main microorganisms found on the skin are P. acnes, Staphylococcus epidermidis and Malassezia spp.22 The main bacteria involved in the pathogenesis of acne is the Propionibacterium acnes (P. acnes).22 There is no conclusive experimental evidence for the pathogenetic relevance of acne linked to other microorganisms.
P. acnes are the dominant bacteria in hair follicles. They prefer anaerobic or microaerophilic conditions, they are gram-positive diphtheroids of the Corynebacterium genus, preferably colonizing regions with high sebum production. They produce porphyrins, in special coproporphyrin III, fluorescing under the Wood's lamp.1
Recent data confirm that P. acnes has a strong pro-inflammatory activity directed by the molecules of innate cutaneous immunity, keratinocytes, and sebaceous glands of the pilosebaceous follicle, in addition to the fact that it participates in the formation of the comedo.16 It is able to rupture the comedo based on the action of their enzymes: lipases, proteases, hyaluronidases, and others recently described - such as endoglycoceramidase, sialidase/neuraminidase, proteases and Camp 5 factors, which contribute to tissue degradation and stimulate the inflammatory response.16
P. acnes acts on the innate immunity by stimulating the activation of toll-like receptors (TLRs).23 Toll-like receptors are part of the first system of defense against microorganisms. They are transmembrane proteins located in the cell membrane of various cells of epidermal embryonic lineage, such as keratinocytes, macrophages, Langerhans cells and lymphocytes T and B. When in contact with pathogen-associated molecular patterns (PAMPs), which can be gram-negative bacterial lipopolysaccharide, flagellin, and lipoteichoic acid from gram-positive bacteria, these receptors are activated and trigger an inflammatory cascade with the production of pro-inflammatory cytokines and metalloproteinases (1, 9, 13). The metalloproteinases degrade the extracellular matrix.23
Based on the recognition of P. acnes' structures, the activation of toll-like type-2 and pro-inflammatory receptors in addition the receptors located on the surface of the perifollicular monocytes, takes place.24 This culminates with the onset of an inflammatory process via TH1, with the production of chemotactic factors for neutrophils, monocytes and lymphocytes; the production of tumor necrosis alpha factor, interferon and interleukins IL-6, 8, 12 and 1-beta. Keratinocytes secrete IL-8, IL-10 and IL-1-alpha, which amplify the inflammatory response.24
The activation of toll-like receptors also leads to the release of antimicrobial peptides (AMP), forming a chemical barrier for the protection of the epithelium.15 These are defense peptides that are also part of the innate immunity process. They are proteins of high molecular weight with broad antimicrobial spectrum against bacteria, fungi and viruses. The AMPs are produced by keratinocytes, monocytes, mast cells, sebocytes, neutrophils and natural killer cells. There are three types of peptides that are noteworthy: cathelicidins, defensins, and granulysins.24 The cathelicidin LL-37 is produced by neutrophils and epithelial cells and influences the function of TLRs. The beta-defensin-2 protects the pilosebaceous unit from P. acnes invasion. The granulysins are found in cytotoxic granules of T-lymphocytes and natural killer cells, and have am antibacterial and anti-inflammatory action against P. acnes. It has been shown that P. acnes is capable of promoting the expression of cathelicidin and beta defensin-2 in the sebocytes.15, 24 During the inflammatory process, there is a release of anti-inflammatory peptides, such as be-ta-defensin type-2, which protects the pilosebaceous unit from P. acnes invasion.24
Dermal periglandular inflammation
A new theory proposes that the inflammatory process is present at all stages of the physiopathogenesis of acne, including before the formation of the comedo, with important participation of P. acnes and inflammatory mediators, such as cytokines, defensins, peptidases, and neuropeptides.24 This theory suggests acne should be classified as a chronic inflammatory and silent disorder.
Although the four processes described are present, there would not be a defined sequence among them and the inflammatory process would already be observed in the initial phase of acne formation.25 The presence of T CD4+ lymphocytes, macrophages and an increase in interleukin 1 (IL-1) in pilosebaceous follicles have shown that inflammation precedes the hyperkeratinization process, with the participation of P. acnes at the beginning of the formation of the comedo.26
Thus, the fact that the micro-comedo is actually the initial lesion and the precursor of other lesions is questionable.24 The inflammatory process arises as the protagonist at all stages of acne formation - from the comedogenesis up until the formation of scars.25 Recent studies show an inflammatory infiltrate in 77% of atrophic scars.26
Acne begins when the adrenocorticotropic hormone (ACTH) acts on the adrenal gland, causing the release of dehydroepiandrosterone sulfate (DHEAS), which stimulates the production of androgens.15 In addition to ACTH and DHEAS, the growth hormone (GH), acting on the liver, stimulates the production of insulin-like growth factor 1 (IGF-1), with the latter also being capable of stimulating the production of DHEAS by the adrenal gland, increasing the production of androgens and, consequently, the production of sebum.15 IGF-1 also acts on the homeostasis of the epidermal barrier, increases the proliferation, and reduces the differentiation of keratinocytes, interfering in the keratinization process. It is also capable of activating the transcription of genes involved in the synthesis of fatty acids, stimulating lipogenesis, which culminates in increased production of sebum.15
With the hypersecretion of sebum there is a reduction in the concentration of its components, especially the linoleic acid, 11 with resulting changes in the function of the epidermal barrier. The "rupture" of the skin barrier leads to the release of IL-1 alpha (this cytokine is present in the early stages of acne formation) and to the penetration of microorganisms and pro-inflammatory fatty acid in the dermis, leading to infection and inflammation. In this phase, P. acnes already stimulates the release of proinflammatory cytokines, such as IL-1-beta, by keratinocytes, macrophages, and sebocytes. The rupture of the skin barrier also leads to an increased population of T CD4+ lymphocytes and other inflammatory mediators in the skin, such as tumor necrosis factor alpha.13
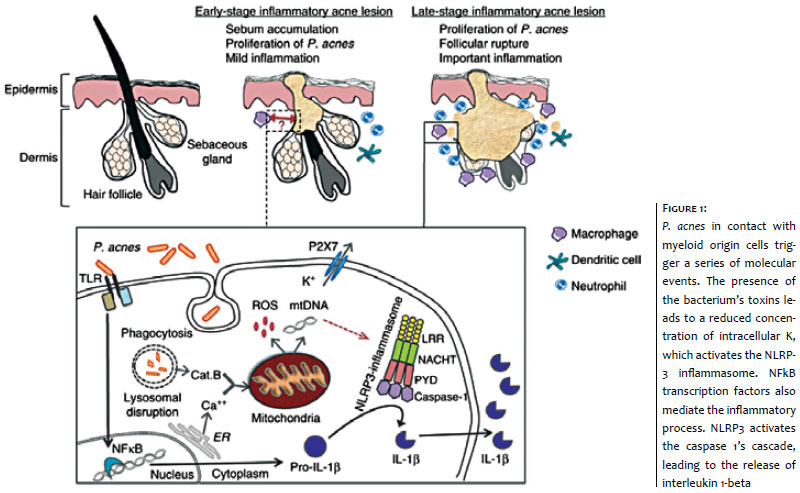
The presence of P. acnes leading to inflammation is presently considered the main pathogenesis of acne vulgaris.27 The monocytes are stimulated by the presence of P. acnes, with an increased expression of caspase 1 genes and secretion of pro-inflammatory cytokines, such as interleukin 1-beta (IL1-beta) via the inflammasomes NLRP-3.7 (Figure 1)
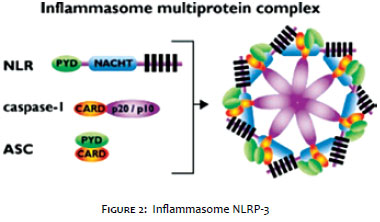
The inflammasome is a multiprotein complex composed of caspase 1, Pycard, Nalp and, sometimes, caspase 5. It is expressed in myeloid cells and is a component of innate immunity. It is responsible for the activation of the inflammatory process through the release of proinflammatory cytokines, such as interleukin 1-beta and interleukin 18.28 (Figure 2)
The first form of defense is the innate immunity through standard antigen recognition receptors located on the cell membrane, toll-like receptors (TLRs), and c-type lectin receptors (CLRs); and nod-like receptors (RLNs) and RIG-I-like receptors (RLRs) in the cytoplasm. Two subtypes NRLs - NLRP1 and NLRP3 - are able to activate the caspase 1's cascade and lead to the production of cytokines (interleukin 1-beta and 18). These two subtypes of NRLs are called inflammasomes NLRP-1 and NLRP-3. 29
The participation of NLRP-3 inflammasome has particular importance in the pathogenesis of acne: it mediates immune responses through interaction with transcription factors (NFKB), activates the caspase 1's cascade and leads to the release of pro-inflammatory cytokines IL 1-beta and 18 (Figure 1). This inflammasome is activated by the reduction in the intracellular K concentration that occurs in the presence of bacterial toxins. Inflammasomes NLRP-3 and caspase 1 are found in acne lesions around the pilosebaceous follicles.30
Currently, other cytokines have been described as participants in the inflammatory process that leads to the formation of acne: interleukin 6-572C, interleukin 1A-889T and interleukin 17. 31 The presence of T CD4+ lymphocytes and interleukin 17 in the perifollicular region suggests that P. acnes stimulates the inflammatory response via Th1 and also via Th17. 32
In sum, the patient's immune response appears to be decisive in the inflammatory response triggered by P. acnes. 33 On the other hand, the same mechanism can be responsible for producing protective responses against P. acnes. The balance between immune, innate, and adaptive responses triggered by P. acnes probably determine when a patient will have clinically active lesions.33
Other factors
Other factors have been postulated as being important in acne formation.
Genetics
Genetic predisposition has been shown to be an important predisposing factor influencing the number, size, and activity of the sebaceous gland.34
The concordance rate for identical twins is quite high, and probably many genes are involved in the predisposition to acne.35 People with XYY karyotype often show severe course of acne. It is possible to notice its influence on the hormonal control and the process of follicular hyperkeratinization.35
Medications
Certain medications, such as benzodiazepines, lithium, cyclosporine, corticosteroids, ramipril, isoniazid, and vitamin B complexes, are associated with the development of this disorder.36
Diet
A diet rich in foods with high glycemic load, insulin resistance, the use of occlusive cosmetics, emotional stress, and early puberty are other important factors in the development of acne.37
For a long time diets were dismissed from the etiological point of view due to past studies that were poorly designed from a scientific standard. In recent years, however, this field has been revised, and several studies have come to relate acne to the adoption of westernized eating habits.38
In a study that evaluated more than 1,200 individuals of two non-westernized societies (Kitavan islanders of Papua New Guinea and the Ache people of Paraguay), the absence of acne in the populations is attributed to their eating habits. In their diets there is a substantially low glycemic index as compared to Western diets.39
In epidemiological studies of the population of Inuit Eskimos, it was found that its members did not have acne up until the introduction of Westernized eating habits.40
In 2012, Kwon showed that a diet with an intake of highly glycemic foods plays a fundamental role in the pathogenesis of acne, and the adoption of low-glycemic diets leads to the improvement of symptoms of this condition.41
It is suggested that the adoption of a diet with a high glycemic load leads to increased serum levels of insulin and IGF-1, and reduced SHBG.42 In the ovary, both IGF-1 and insulin are capable of stimulating the release of androgenic hormones that act on the sebaceous gland, stimulating sebum production, in addition to stimulating the release of pro-inflammatory cytokines and acting on the keratinization process.42
An exception to the evidence of the high-glycemic index diet is the intake of dairy products. Despite their low glycemic index, they paradoxically induce an increase of IGF-1 levels, favoring the appearance and/or aggravation of acne - which is particularly higher when skimmed milk is ingested. This demonstrates that the association is not due to the milk's fat content, reinforcing the IGF-1 level theory.43, 44 In addition to the IGF-1's acnegenic capacity, milk contains estrogen, progesterone, androgen precursors (such as androstenedione and dehydroepiandrosterone sulfate) and steroid-5α-reductase dependents (such as 5α-androstenedione, 5α-pregnonadione and dihydrotestosterone), some of which are involved in the comedogenesis.45
Furthermore, in order to simulate the consistency of whole milk, whey proteins - especially α-lactalbumin - are added to the formula of low fat and skimmed milk, which also appears to play an important role in the comedogenesis.44, 45
It is known that the ingestion of iodine can exacerbate acne. Another argument that reinforces the hypothesis of the strong correlation between milk consumption and acne pictures is that the iodine contained in milk may be involved in the etiology of this dermatosis (iodine is contained in the dietary supplementation given to animals and in the iodine-based solutions used in milking equipment).45
In a recently published double-blind randomized study of the use of fatty acid supplementation of omega 3 and omega 6 types in 45 patients for 10 weeks, Jung concluded that both types of supplementation led to an improvement in acne vulgaris, with the reduction of inflammatory and non-inflammatory lesions, without serious adverse effects.46
The strong correlation of acne and the use of dietary supplements rich in branched chain amino acids is also observed in the daily practice. In order to gain muscle mass, many young people currently make use of whey protein type amino acids, which is composed of amino acids derived from whey.47 A study conducted with 30 participants in the northeast Brazilian city of João Pessoa all of whom were using whey protein, showed that 100% of users developed inflammatory acne grade III or had intensification of the pre-existing picture after two months of use.47 A dissertation focusing on adult women showed that those using supplementation were seven times more likely to develop acne. 48 Amino acids such as lysine, arginine, leucine, isoleucine, and casein are capable of stimulating sebocytes. Furthermore, some of these supplements have growth factors that can be correlated to the onset of acne.47, 48
The pathogenesis of acne vulgaris is a subject that involves old concepts associated with new concepts, especially regarding the inflammatory process.
Some new facts (such as: 1. acne vulgaris is not an infectious disorder; 2. acne vulgaris is a primarily inflammatory disorder; 3. the role of P. acnes is more inflammatory than infectious; 4. inflammation is present in all stages of acne formation, including that of scars) are already accepted.
This knowledge is important in the search for a better therapeutic approach. Its inflammatory, chronic, and multifactorial nature should always be taken into account.
1. Winston MH, Shalita AR. Acne vulgaris. Pathogenesis and treatment. Pediat Clin North Am. 1991;38(4):889-903.
2. Rea JN, Newhouse ML, Halil T. Skin disease in Lambeth. A community study of prevalence and use of medical care. Br J Prev Soc Med. 1976;30(2):107-14.
3. Wolkenstein P, Grob JJ, Bastuji-Garin S,Ruszczynskin S, Rouzeau JC, Revuz J, et al. French people and skin diseases: results of a survey using a representative sample. Arch Dermatol.2003;139(12):1614-9.
4. Johnson MT, Roberts J. Skin conditions and related need for medical care among persons 1-74 years. United States, 1971-1974. Vital Health Stat. 1978; 212:i-v, 1-72.
5. Law MPM, Chuh AAT, Molinari N, Lee A. Acne prevalence and beyond: acne disability and its predictive factors among Chinese late adolescents in Hong Kong. ClinExpDermatol.2010;35(1):16-21. [erratum in Clin Exp Dermatol. 2010;35(3):339].
6. Yahya H. Acne vulgaris in Nigerian adolescents: prevalence, severity, beliefs, perceptions, and practices. Int J Dermatol. 2009;48(5):498-505.
7. Rademaker M, Garioch JJ, Simpson NB. Acne in schoolchildren: no longer a concern for dermatologists. BMJ.1989;298:1217-19.
8. White GM. Recent findings in the epidemiologic evidence, classification, and subtypes of acne vulgaris. J Am Acad Dermatol. 1998;39(2 PT 3):S34-7.
9. Goulden V, Clarck S, Cunliffe W. Post-adolescent acne: a review of clinical features. Br J Dermatol.1997;136(1):66-70.
10. Degitz K, Placzek M, Borelli C, Plewig G. Pathophysiology of acne. J Dtsch Dermatol Ges. 2007;5(4):316-23.
11. Costa A, Alchorne MMA, Goldschmidt MCB. Fatores etiopatogênicos da acne vulgar. An Bras Dermatol.2008;83(5):112-15.
12. Kircik, LH. Evolving concepts in the pathogenesis of acne vulgaris. J Drugs Dermatol. 2014;13(6):56.
13. Beylot C, Auffret N, Poli F, Claudel JP, Leccia MT, Del Giudice P, et al. Propionibacterium acnes: an update on its role in the pathogenesis of acne. J Eur Acad Dermatol Venereol. 2013;28(3):271-8.
14. Cunliffe WJ, Holland DB, Clarck SM, Stables GI. Comedogenesis: some aetiological, clinical and therapeutic strategies. Dermatology. 2003;206(1):11-6.
15. Harvey A, Huynh TT. Inflammation and acne: putting the pieces together. J Drugs Dermatol. 2014;13(4):459-63.
16. Bellew S, Thiboutot D, DelRosso JQ. Pathogenesis of Acne vulgaris: What's New, What's Interesting and What may be clinically relevant. J Drugs Dermatol. 2011;10(6):582-5.
17. Jahns AC, Eilers H, Ganceviciene R, Alexeyev OA. Propionibacterium species and follicular keratinocyte activation in acneic and normal skin. Br J Dermatol. 2015;172(4):981-7
18. Degitz K, Placzek M, Arnold B, Plewig G. EndokrinologischeAspektebeiAkne. In: Plewig G, Degitz K, (Hrsg): Fortschritte der praktischenDermatologie und Venerologie. Berlin: Springer, 2001. p. 72-179.
19. Zouboulis CC, Böhm M. Neuroendocrine regulation of sebocytes - a pathogenetic link between stress and acne. Exp Dermatol. 2004;13(Suppl. 4):31-5.
20. Thiboutot D, Gilliland K, Light J, Lookingbill D. Androgen metabolism in sebaceous glands from subjects with and without acne. Arch Dermatol. 1999;135(9):1041-5.
21. Kamangar F, Shinkai K. Acne in adult female patient: a practical approach. Int J Dermatol. 2012;51(10):1162-74.
22. Till AE, Goulden V, Cunliffe WJ, Holland KT. The cutaneous microflora of adolescent, persistent and late onset acne patients does not differ. Br J Dermatol. 2000;142(5):885-92.
23. Kim J, Ochoa MT, Krutzik SR,Takenchi O, Vematsu S, Legaspi AJ, et al. Activation of toll-like receptor 2 in acne triggers inflammatory cytokine responses. J Immunol. 2002;169(3):1535-41.
24. Tanghetti EA.The role of inflammation in the pathology of acne. J Clin Aesthet Dermatol. 2013;6(9):27-35.
25. Jeremy AH, Holland BD, Roberts SG,Thomson KF, Cunliffe WJ. Inflammatory events are involved in acne lesions initiation. J Invest Dermatol. 2003;28(1):2-7.
26. Lee WJ, Jung HJ, Lim HJ, Jang YW, Lee SJ, Kim DW. Serial sections of atrophic acne scars help in the interpretation of microscopic findings and the selections of good therapeutic modalities. J Eur Acad Dermatol Venereol. 2011;27(5)1-4.
27. Qin M, Pirouz A, Kim J. Propionibacterium acnes induces IL-1beta secretion via the NLRP3 inflammasome in human monocytes. J invest Dermatol. 2014;134(2):381-8.
28. Franchi L. Sensing and reacting to microbes through the inflamassomes. Nat Immunol. 2012;13(4):325-32.
29. Martinon F, Burns K, Tschopp J. The inflammasome: a molecular platform triggering activation of inflammatory caspases and processing of pro IL-beta. Mol Cell. 2002;10(2):417-26.
30. Das S, Reynolds RV. Recent advances in acne pathogenesis: implications for therapy. Am J Clin Dermatol.2014;15(6):479-88.
31. Younis S, Javed Q. The Interleukin 6 e Interleukin A gene promote polymorphism in associated with pathogenesis of acne vulgaris. Arch Dermatol Res. 2015;307(4):365-70.
32. Agak GW, Qin M, Kim MH, Krutzik SR, Tristan GR, Elashoff D, et al. Propionibacterium acnes induces an IL-17 response in acne vulgaris that is regulated by Vitamin A and Vitamin D. J Invest Dermatol. 2014;134(2):366-73.
33. Nakatsuji T, Liu Y-T, Huang C-P, Gallo RL, Huang C-M. Vaccination targeting a surface sialidase of P. acnes: implication for new treatment of acne vulgaris. PLoSOne. 2008;3(2):e1551.
34. Sobral Filho JF, Silva CNA, Rodrigues JC, Rodrigues JLTD, Aboui-Azouz M. Avaliação da herdabilidade e concordância da acne vulgar em gêmeos. An Bras Dermatol. 2007;72(5):225-8.
35. Herane MI, Ando I. Acne in infancy and acne genetics. Dermatology. 2003;206(1): 24-8.
36. Dessinioti C, Antoniou C, Katsambas A. Acneiform eruptions. Clin Dermatol. 2014;32(1):24-34.
37. Bhambri S, Delrosso J, Bhambri A. Pathogenesis of Acne Vulgaris: Recent Advances. J Drugs Dermatol. 2009;8(7):616-9.
38. Melnik BC, Schmitz G. Role if insulin, insulin-like growth factor 1 receptor signaling regulates skin development and inhibits skin keratinocyte differentiation. Mol Cell Biol. 2006;26(7):2675-87.
39. Cordain L, Lindeberg S, Hurtado M, Hill K, Eaton SB, Brand-Miller J. Acne vulgaris: a disease of Western civilization. Arch Dermatol. 2002;138(12):1584-90.
40. Costa A, Lage D, Moisés TA. Acne and diet: truth or myth? An Bras Dermatol. 2010;85(3):346-53.
41. Kwon HH, Youn JY, Homg JS. The clinical and histological effect of low glycemic load diet in the treatment of acne vulgaris in Korean patients. Acta Derm Venereol. 2012;92(3):241-6.
42. Yarak S, Bagatin, E Hassun KM, Parada MOAB, Talarico Filho S. Hiperandrogenismo e pele: síndrome do ovario policístico e resistência periférica a insulina. An Bras Dermatol 2005;80(4):395-410.
43. Adebamowo CA, Spiegelman D, Danby FW, Frazier AL, Willett WC, Holmes MD. High school dietary dairy intake and teenage acne. J Am Acad Dermatol. 2005;52(2):207-14.
44. Adebamowo CA, Spiegelman D, Berekey CS, Danby FW, Rockett HH, Colditz GA, et al. Milk consumption and acne in adolescents girls. Dermatol Online J. 2006;12(4):1.
45. Danby FW. Acne and milk, the diet myth, and beyond.J Am Acad Dermatol. 2005;52(2):360-2.
46. Jung JY, Kwon HH, Hong JS, Yoon JY, Park MS, Jang MY, et al. Effect of dietary supplementation with omega-3 fatty acid and gamma-linolenic acid on acne vulgaris: a randomised, double-blind, controlled trial. Acta Dermato-Venereologica. 2014;94(5):521-5.
47. Pontes TC, Fernandes Filho GMC, Trindade ASP, Sobral Filho JF. Incidência de acne vulgar em adultos jovens usuários de suplementos proteico-calóricos na cidade de João Pessoa-PB. Na Bras Dermatol. 2013;88(6):909-14.
48. Ribeiro, BM. Acne da mulher adulta: análise clínica, etiológica e de imagem. Brasília. Dissertação (Mestrado em Ciências da Saúde) - ESCS/FEPECS/SES/DF; 2014.
This study was carried out at the Dermatology Department, Faculdade de Ciências Médicas de Minas Gerais - Belo Horizonte (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}