


Beatriz de Medeiros Ribeiro1; Ivonise Follador2; Adilson Costa3; Fábio Francesconi4; Juliane Rocio Neves5; Luiz Maurício Costa Almeida6
Acne in adult women is defined as an acneic picture present in women from 25 years of age. It can onset in adolescence and continue into adulthood or appear in the latter phase. It has an impact on personal relationships and can lead to introspection and depression. It is predominantly characterized by inflammatory lesions located preferentially on the chin and neck. Its causes have not yet been fully elucidated. Its pathogenesis involves circulating androgens in combination with other factors such as heredity, stress, ultraviolet exposure, obesity, diet, smoking habits and the presence of associated endocrine disorders. Treatment includes the arsenal for treating acne vulgaris combined with other therapies.
Keywords: ACNE; HYPERANDROGENISM; PROPIONIBACTERIUM ACNES; HYPERINSULINISM
Acne vulgaris is a chronic inflammatory, multifactorial, and immune-mediated dermatosis that affects the pilosebaceous unit and is characterized by presenting with a varied clinical picture. 1
It is a very common condition with great epidemiological impact, affecting approximately 40 to 50 million individuals worldwide.2
It occurs mostly in adolescence, affecting about 85% of young people, with a peak rate of incidence between the ages of 12 and 24, however it can affect newborn babies, children, and adults.1, 2 Although considered typical in adolescence, an increased frequency in adults, especially in women, is observed. 3,4
Acne in adult women is defined as an acneic picture present in women from 25 years of age.5, 6 This dermatosis tends to become chronic, with periods of exacerbations and improvement.5, 6 It can have its onset in adolescence and continue into adulthood or emerge later on in this phase.6, 7 It occurs in all races, but is more common in Caucasian women and less common in those of Asian origin.
The current prevalence of this disease in adulthood is not well defined, although clinical trials suggest 12% of women and 3% of men will be affected.4 Epidemiological studies show a prevalence of about 41% in adult women.9 This statistic should be considered carefully, however it confirms that it is a common picture.9 There is controversy over whether the frequency has increased or if adult women in the world today are less tolerant to the disorder and better informed about medical treatments.6
Adult acne in women has a negative impact on personal and professional relationships, which can lead to introspection, social isolation, and depression.10 Patients report a loss of quality of life comparable to that caused by psoriasis vulgaris, and a significant association between acne and eating disorders - such as bulimia and anorexia nervosa - is observed.11 Studies show that roughly 40% of adults with acne will present some type of psychiatric disorder.12
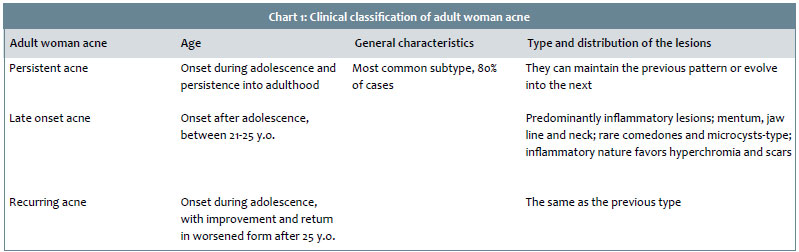
Acne in adult women is classified into three subtypes according to the time of onset:13
Persistent acne: has its onset in adolescence and continues into adulthood. It is the most common subtype, corresponding to 80% of cases.
Late-onset acne or late acne: onset is after adolescence, between 21 and 25 years of age.
Recurring acne: onset in adolescence, followed by a period of improvement of the symptoms and subsequent worsening after 25 years of age (Chart 1).
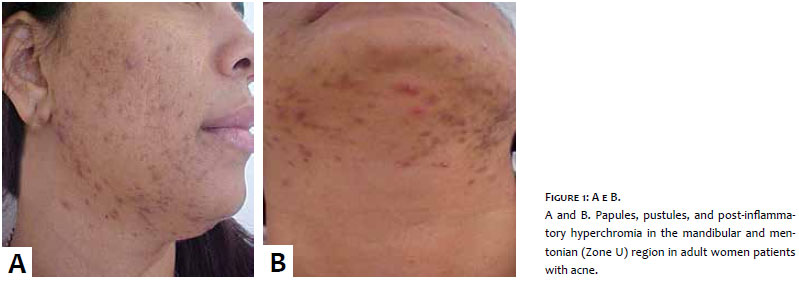
From a clinical point of view it is characterized by predominantly inflammatory lesions, mainly papules and pustules usually located in the mentum, mandible line and neck. 6 Lesions occur in the area described as the U zone, which is also called "the beard region" or "surgical mask".6 It tends to be mild or moderate and refractory to treatment.6 The nodular lesions may also be present and are located in the lower third of the face. They may occur in isolation, in the absence of other inflammatory lesions.14 When the rare presence of comedones is observed, they are rare and closed, resembling microcysts in appearance. 14 Due to the inflammatory nature, development with scars and hyperchromia is common. 14 (Figure 1)
To date and from a clinical point of view, adult woman acne was considered a distinct entity from adolescent acne, however a recent study published by Dréno et al. has been questioning this true clinical pattern in adult women with acne. 15 In this study, the clinical pattern was not maintained, and 90% of studied women had a global distribution of facial lesions and severity similar to those related to adolescents with inflammatory and non-inflammatory lesions. 15 About 90% of women had comedones, and only 6.4% had only inflammatory lesions. 15 Only 11.2% of women had only mandibular lesions and the related worsening of the picture to periods of stress. 15 The adult woman with inflammatory acne in the mandibular region stereotype was not found in the study. 15
The causes of acne in adulthood have not been fully elucidated.
This picture's pathogenesis involves circulating androgens in combination with other factors. 13 The four etiopathogenic processes included in the formation of acne vulgaris are also present in adulthood: follicle hyperkeratinization, sebaceous hypersecretion, bacterial colonization - mainly by Propionibacterium acnes (P. acnes), and periglandular dermal inflammation. 13
Several other factors have been postulated as causative, standing out among them heredity, stress, exposure to ultraviolet radiation, obesity, diet, smoking, and the presence of associated endocrine disorders. 6
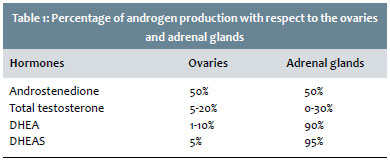
In women, a great part of androgens is produced in the adrenal gland and ovaries. 16 The peripheral production of these hormones is equally important and takes place in the pilosebaceous units. 16
The functioning of the axis hypothalamus-hypophysis-gonads and adrenal glands, as well as the peripheral hormonal activity, will regulate the hormone life of women. 16 There can be alterations in each of the involved organs or in the hormonal peripheral network, leading to clinical and/or laboratory disturbances. 16 The most common is that of women with clinical evidence of hyperandrogenism, with regular menstrual cycles, and entirely normal laboratory evaluation, characterizing the idiopathic or terminal sensitivity caused hyperandrogenism.16
The skin is an important target of androgen hormones and, therefore, the dermatologist is critical in the early diagnosis of endocrine disorders.17 The endocrine disorders should be considered in cases of adult women with acne.17 Nevertheless, they seem to constitute only a cofactor in this universe of signs and symptoms. 17 Of the endocrine disorders related to this axis, the most common is the polycystic ovary syndrome (PCOS) and, secondly, the fruste or secondary adrenal hyperplasia, of late onset.17-19
The hypophysis hormones, luteinizing or luteotrophic hormone (LH) and the follicle-stimulating hormone (FSH) are drivers of the ovarian synthesis of androgens and estrogen. 16 Testosterone is a major circulating androgen, originating from the adrenal glands (30%), ovaries (20%), and from the peripheral skin conversion from other hormones (50%), such as dehydroepiandrostenedione sulfate (DHEAS) and androstenedione. 16 DHEAS is a relevant precursor of testosterone (T) and 90% of it is produced by the suprarenal glands. 16 Androstenedione, also produced in the ovaries, adrenals and peripherally, in turn is a significant androgen, and is also a precursor to dihydrotestosterone (DHT), which is a powerful androgen 17 (Table 1).
The 17-hydroxyprogesterone (17-oh) is used for screening of congenital adrenal hyperplasia, the non-classical form (CAH-NC) due to impairment in the 21-hydroxylase. 17 Testing of this hormone must be requested, especially if DHEAS levels are high or due to specific conditions. 17 Its alteration is rarely found in PCOS. 17 After PCOS, the CAH-NC is the second most frequently detected disorder in this group of women with acne. In these cases, 17-oh levels are increased, as they are in cases of hyperprolactinemia. 17 Between 25-50% of cases of PCOS, with variations in the literature, course with some functional adrenal hyperandrogenism. 17
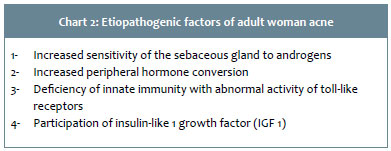
Regarding acne in adult women, four etiopathogenic factors stand out:
Increased sensitivity of the sebaceous gland to androgens:20 hypersensitivity of the receptors found in sebocytes and keratinocytes to circulating androgens can be observed. 20 This hypothesis is based on clinical analysis, such as the worsening of the acneic picture during the premenstrual and premenopausal periods, pregnancy, and during the use of contraceptive progesterone therapy. 21 In these periods an increase of the hormones with more androgenic activity, relative to estradiol, takes place.20, 21
Increased peripheral hormone conversion: hyperactivity and abnormal activity of enzymes related to androgenic hormone metabolism, such as 5-alpha-reductase, 3-beta-hydroxysteroid-dehydrogenase and 17-hydroxysteroid-dehydrogenase, with increased peripheral conversion of pre-hormones (DHEAS, androstenedione and testosterone) into more potent androgens (testosterone and DHT). 21
Innate immune deficiency with abnormal activity of the toll-like receptors or defensins, which induce a reduction in the resistance to P. acnes and chronic inflammation of the sebaceous glands.22 Deficiency of innate immunity is genetically determined, and this may explain the familial occurrence of the acne's clinical picture.22
Insulin-like growth factor 1 (IGF 1) participation as a stimulator of ovarian androgen hormone production and cofactor in the availability of circulating hormones, based on its action as a reducer of hepatic production of the sex hormone-binding globulin (SHBG) 13 (Chart 2).
Currently, several other factors have been associated with the onset of acne in adult women, lending a multifactorial nature to this picture:
Genetic predisposition has been shown to be an important predisposing factor influencing the number, size, and activity of sebaceous glands. 22 Its influence on the hormonal control and the process of follicular hyperkeratinization is also observed. 22
Certain drugs, such as benzodiazepines, lithium, cyclosporin, corticosteroids, ramipril, isoniazid, vitamin B complexes, and progesterone contraception therapy, are associated with the development of acne. 23 First generation progesterones such as norgestrel have an androgenic effect similar to that of the testosterone.13
A diet dominated by foods with a high glycemic index, resistance to insulin, the use of occlusive cosmetics, emotional stress, and early puberty are other important factors in the development of acne.24
The association of acne with the use of dietary supplements rich in branched chain amino acids is also observed in the daily practice.25 Whey protein type amino acids used for gaining muscle,25 are composed of amino acids derived from whey.25
A study with 30 participants who used whey protein showed that after two months of use, 100% of users developed inflammatory acne grade III or had a worsening of some pre-existing picture.25 An MSc thesis conducted with adult women bearing acne showed that these food supplement users are seven times more likely to develop acne. 26 Amino acids such as lysine, arginine, leucine, iso-leucine, and casein are capable of stimulating sebocytes, and some of these supplements contain growth factors that may be related to the emergence of acne.25, 26
Chronic stress has also been deemed a possible cause of acne in adult women.27 The sebaceous gland is a neuroendocrine organ and is modulated by neuropeptides, such as substance P, which stimulates its activity.28 Stress stimulates the release of pro-inflammatory cytokines and corticotropin-releasing hormones, leading to increased levels of cortisol.28 Goulden et al. have reported that 71% of patients described stress as a major factor in a worsening of the picture.3
Recent studies show a close relationship between smoking and the onset of acne in adult women,29, 30 pointing to tobacco as the main factor responsible for the appearance of non-inflammatory acne at that stage.29, 30 A significant difference between acne in smoking and nonsmoking women is observed, with a predominance of the comedonian form in smokers, which led authors to describe the clinical presentation as "smoker's face", characterized by the presence of micro and macro comedones, and few inflammatory lesions.30 The sebaceous gland is sensitive to acetylcholine, which is stimulated by nicotine. 30 Acetylcholine leads to modulation and differentiation and influences the sebum production and composition, also promoting the reduction of antioxidants and increasing the peroxidation of sebum components such as squalene.30
Studies have shown that between 60-70% of women report a worsening of the picture during the premenstrual period. 31 This is due to the relative increase in progesterone levels during the luteal phase of the menstrual cycle.28
The presence of acne in an endocrinopathy is normally associated with other clinical signs of hyperandrogenism, such as hirsutism, seborrhea, alopecia, menstrual disorders, ovulatory dysfunction, infertility, precocious puberty, metabolic syndrome, (MS) and virilization.17, 32 The intensity and extent of these clinical manifestations depend on several factors, and there is no strict correlation between the intensity of the clinical picture and the biochemical alterations.17 The main endocrine disorders that course with female hyperandrogenism are PCOS, fruste or late congenital adrenal hyperplasia and, more rarely, ovarian, adrenal, hypophysis, and hypothalamic tumors.17
PCOS is considered the leading cause of hyperandrogenism in women and has a prevalence of 5-10% in the general population.18 The first study conducted in Brazil and South America aimed at estimating the prevalence of PCOS in a randomized population, and confirmed that figure, with an 8.5% prevalence in the studied population.33 According to the consensus of Rotterdam 2004, diagnosis is carried out based on the presence of clinical criteria.18
The presence of two of the following three criteria reported below defines the diagnosis: amenorrhea or oligomenorrhea, clinical or biochemical alteration of hyperandrogenism, and ultrasonographic documentation showing an increased count of follicles (> 12) or of follicular volume (> 10cm3) per ovary.18 Acne is a common cutaneous sign in cases of PCOS, but often is associated with other clinical signs of hyperandrogenism, such as hirsutism (most common and present clinical sign in a percentage ranging from 65-73% of cases), alopecia, seborrhea, and acanthosis nigricans. 18
An increase in the value of the LH/FSH ratio may occur in PCOS. Some authors report a 3:1 rate, others 2:1. This is no longer a diagnostic criteria, although it is information that may provide valuable assistance during diagnostic evaluation. 17
Hyperprolactinemia syndromes can lead to the alteration of androgens through this path or even through an undifferentiated stimulus of macro-receptors.17 Prolactin stimulates the secretion of dehydroepiandrosterone sulfate (DHEAS).17 SDHEA is produced almost exclusively by the adrenal glands, meaning that its value does not usually change in PCOS.17
The picture often associated with adult women with acne and PCOS includes hyperinsulinism and increased peripheral resistance to insulin (RI).17 It seems that hyperinsulinism is the most important biochemical alteration in PCOS.17 Insulin acts through connections to insulin receptors (belonging to the family of tyrosine-kinase receptors) that are distributed in the ovaries, as well as to IGF-1 receptors (also belonging to the tyrosine-kinase family), and to hybrids of the two types of receptors.17
Hyperinsulinemia leads to an increased production of androgens by the ovaries (mainly of androstenedione and testosterone) and of insulin-like growth factors I and II (IGFs) in the liver. 17 The increase in IGF-1 inhibits aromatase [o Volp não confirma a aromatase; favor confirmar] and prevents the conversion of testosterone into estrogen. 17 Within that hyperinsulinemia there is still a decrease in the hepatic production of SHBG, favoring an increase in the levels of free androgens, which is the active form.17 There are many obese women with an increased peripheral resistance to insulin who do not develop PCOS, probably due to genetic factors in insulin's post-receptor mechanisms of action.17
It is also important to evaluate the possibility of glucose intolerance in these adult women with acne and PCOS, for the latter is a risk factor that is more important than race or ethnicity in this situation.17 In PCOS, total cholesterol is increased at the expense of increased low-density lipoprotein fraction (LDL), however with a decrease in high-density lipoprotein (HDL).17 Triglycerides and the concentration of plasminogen activator inhibitor (PAI), also tend to be increased.17 These lipid changes in the PCOS, associated with increased PAI, favor high blood pressure, coronary heart disease, and thrombosis.17
In women with acne, obesity, and PCOS, the installation of the metabolic syndrome (MS) is very frequent. MS is characterized by:17
Abdominal obesity (waist circumference)> 88 cm;
Triglycerides > 150mg / dL;
HDL < 50mg / dL;
Blood pressure > 130 / > 85 mm Hg;
Rapid blood glucose test = 110-126mg / dL, and
Blood glucose test two hours after the glucose tolerance test = 140-199mg / dL.
Therefore, when assessing an adult woman with acne, it is important to carry out a detailed clinical and laboratory evaluation in search of other signs of hyperandrogenism, obesity, acanthosis nigricans, hypertension, diabetes, dyslipidemia, and insulinemia. In this way, dermatologists can collaborate in the diagnosis of a possible disease with greater base risk, such as PCOS, IR, and MS.17
From a laboratorial point of view, the studies related to the investigation of androgenic hormones in adult women with acne are not unanimous in reporting hyperandrogenism.3, 19, 20, 34 It is possible to observe that the onset of an acneic picture at this stage of life, without associated hormone linked disorders, is increasingly frequent. 19
This picture, devoid of laboratorial correspondence, is called idiopathic or due to terminal sensitivity. 20 Perhaps in the future it will be possible to detect and document more accurately alterations in receptors or enzymes linked to this metabolism.20
Clinical and laboratory evaluation
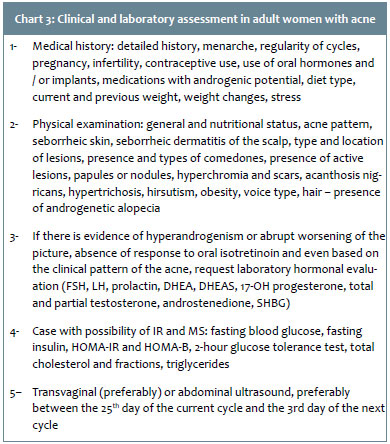
All acne-bearing adult women should undergo a detailed anamnesis that investigates the time of onset of the picture, menstrual irregularities, plans to become pregnant, and the causal factors listed above, such as the use of medicaments, cosmetics and dietary supplements, smoking habits, and stress.6 They should also undergo detailed physical examination in search of clinical signs of hyperandrogenism.13
Hormonal evaluation should be performed in women who present some sign or symptom of hyperandrogenism, virilization, menstrual irregularity, infertility, acne resistant to conventional therapies, a sudden worsening of the picture, and rapid recurrence after the completion of the treatment with oral isotretinoin. 13 It is important to investigate the history of contraceptive use--including type and duration of usage--as the onset or worsening of acne in adult woman is very common after contraceptive suspension.13 In women sensitive to androgens, the use of an intrauterine device with progestin can lead to the onset or worsening of acne, especially in the first year of use.35
Serum hormone dosage should be performed in the follicular phase of the menstrual cycle, with dosage of DHEAS, free and total testosterone, FSH, LH, prolactin and 17-hydroxy-progesterone. 13 Women should discontinue the use of oral contraceptive and hormone therapy for four to six weeks before laboratory evaluation13 (Chart 3).
In cases where there is a suspicion of PCOS, a pelvic or transvaginal ultrasound examination should be requested, and patients should be instructed to undergo the examination between the 25th day of the current cycle and the 3rd of the next cycle.17
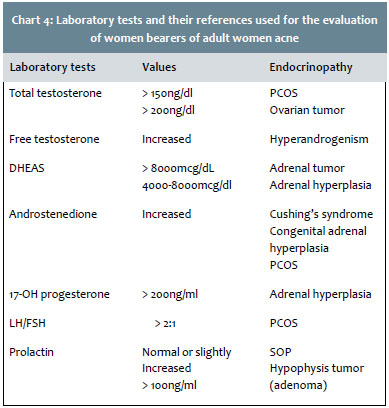
Most women will present normal results, however this does not exclude the benefit of hormone therapy due to what was explained above regarding etiopathogenesis, increased terminal sensitivity, and increased peripheral conversion. 6
When present, the laboratorial alterations may hint at the presence of endocrine diseases associated with the picture.13, 17 (Chart 4)
Treatment should generally follow the treatment algorithm of acne vulgaris. 36 In comedonian acne, the use of retinoids is prioritized, however in other grades, combinations with complementary mechanisms should be preferred and hormonal systemic therapies should be used.13
Topical treatment
It is an option in mild to moderate acne. 6
Due to the fact that it is a chronic picture that will require prolonged treatment, priority should be given to a simple, well-tolerated treatment, and preferably with a single daily application. This increases adherence to treatment as compared to those with two daily applications. 37 As the therapy alone is often not able to act during all stages of acne formation, combined topical therapies should be chosen. 37 Good alternatives are retinoids, benzoyl peroxide, and azelaic acid. 6
Retinoids
Recommended in comedonian acne and mild to moderate inflammatory acne. 38 They can be used as a monotherapy or with other topical substances, such as benzoyl peroxide, and oral treatments. 6
The various topical retinoids can be used with similar efficacy results in both inflammatory and non-inflammatory lesions. 39 Adapalene proved to be better tolerated. 39 All topical retinoids depend on the initial clarifying medical guidance in order for the patient to have an adequate adhesion and overcome the initial phase of possible irritation. 40 Studies show that its association with spironolactone may strengthen the effect of isolated topical treatment.40
Benzoyl peroxide
Due to its bactericidal, anti-inflammatory, and keratolytic properties, it is recommended as part of the combinations for nearly every topical treatment.41 Lower concentrations should be chosen as they have an action similar to that of the higher concentrations and cause less irritation.41
Due to the fact that it presents toxicity against P. acnes, it should be used in an attempt to reduce bacterial resistance. 41
Oral and topical antibiotics, such as monotherapy, should be avoided in the treatment of acne due to the chance of bacterial resistance.6
Azelaic acid
Azelaic acid has bactericide, anti-inflammatory, and keratolytic properties similar to those of benzoyl peroxide.42
It has better absorption in gel and presents an initial "pinching" side-effect, which can hinder patient adherence, in the absence of professional guidance.42 Except for this aspect, which can be overcome with the use of small amounts and sometimes associated with moisturizer, it has a good tolerance and also action on post-inflammatory hyperpigmentation due to its inhibitory action on tyrosinase.6
Systemic treatment
Indicated in moderate or severe extensive acne, associated with scarring and resistant to topical treatment.43
Antibiotics
The best options are lipophilic antibiotics, such as tetracyclines, lymecyclines, doxycycline, minocycline, clindamycin, trimethoprim, and macrolides. 43
Typically, a good response is observed, however they should not be used or maintained as a monotherapy due to the risk of bacterial resistance development. 43
They must be used in accordance with the same guidelines as acne vulgaris treatment. 43 In the case of topical use, they should be preferably associated with benzoyl peroxide or azelaic acid. 42 Oral use should not be concomitant with topical antibiotic, with the exception of benzoyl peroxide, azelaic acid, or even topical retinoid. 43 Topical retinoids are the best options regarding maintenance. 39
Isotretinoin
Isotretinoin is an oral retinoid indicated for the treatment of severe, recurrent, nodular acne that is not responsive to traditional therapies. 44 Indications are similar to those of acne vulgaris, with a probability of recurrence in 32% of adult women. 13
There are some signs that may indicate a greater chance of success of oral isotretinoin use in adult women: low body mass index, low glycemic index diet, absence of smoking habits, absence of precocious acne, and absence of cervical lesions. 44 Women often prefer the low dose schemes due to the lower chance of side effects. 13
Hormone therapy
Hormonal therapy includes three types of medications.45 i) Androgen receptor blockers (or anti-androgens); ii) Androgen and/or adrenal production inhibitors; iii) Androgen metabolizing enzyme inhibitors.45
It is indicated in women with clinical signs of hyperandrogenism, women diagnosed with adrenal or ovarian hyperandrogenism, those not responsive to traditional therapies, with a history of menstrual irregularity, or those who desire contraception.45
It can be used as a monotherapy, however it is usually associated with other systemic and topical therapies.43
Cyproterone acetate
The cyproterone acetate (CPA) is a potent blocker of androgen receptors and also an ovulation inhibitor. 46 It has progestinic action, therefore it is usually associated with ethinyl estradiol for contraception.46
It can be used in isolation at doses of 25 - 100 mg per day, from the 5th to the 14th day of the menstrual cycle, however the preference is for low doses (2 mg) combined with ethinyl estradiol (35µg).46 The use of this combination will result in the slow improvement of adult woman acne: an improvement rate of about 30% after three months of use, with excellent response rates (90%) after 12 months of use, and improvement of virtually 100% at the end of 36 months of use. 46 Isolated reports of hepatocellular carcinoma in mice have not been proven in humans in larger studies. 46 The use of contraceptives with CPA is approved in Europe, Canada, and Brazil, however not in the U.S. 46
Spironolactone
Spironolactone is an antagonist of aldosterone and is used as a potassium-sparing diuretic, also acting as an androgen receptor blocker.45, 47
It has an inhibitory effect on 5-α-reductase enzyme and on 17-beta hydroxysteroid dehydrogenase (17β-HSD).46 Its dose ranges from 50 - 200 mg per day, and improvement is noticeable from the 3rd month.46 It has an oral absorption rate of 40 - 70% by hepatic metabolism. It should be started at low doses and progressive increases at intervals of 15 to 30 days.46
Its most common side effects are the diuresis, menstrual irregularities, breast pain, postural hypotension, hyperkalemia (rare).47 Ideally, spironolactone should be used concomitantly with a contraceptive in order to prevent conception or avoid intercyclic bleeding (spots).43 It has no association with malignancy and is the most widely used antiandrogen in the U.S.48
Flutamide
It is an antiandrogen used to treat prostate cancer, having been used as an off label treatment of disorders linked to hyperandrogenism in women, nevertheless this use was completely banned due to the increased risk of fulminant hepatitis.48
Finasteride
Finasteride is a 5-α-reductase inhibitory drug indicated for the treatment of prostate diseases and, in dermatology, for the treatment of male androgenetic alopecia (AGA) as well as some specific cases of female AAG as an off-label medicament.46 It does not have use in acne vulgaris or for adult women with acne.46
Gonadotropin release agonists
There are substances (buserlin, nafarelin and leuprolide) in injectable or nasal spray form that act similarly to gonadotropin-releasing hormone, blocking ovulation through the inhibition of the release of FSH and LH by the hypophysis gland.49 These drugs lead to the suppression of ovulation and could improve acne in adult women, however they also lead to symptoms such as hypoestrogenism, early menopause, migraine, loss of bone mass, and others, so their indication is very specific and restricted.49
Metformin
Metformin is not an antiandrogen, but one insulin-sensitizing agent (as is thiazolidinedione) that increases the sensitivity of tissues to insulin action.50 Metformin reduces hepatic gluconeogenesis and increases muscle sensitivity to insulin, lowering the concentration of serum insulin and therefore reducing the production of androgens by theca cells.50 It is not hypoglycemic, due to the fact it does not increase insulin secretion.50
Metformin decreases the concentration of total cholesterol, HDL and triglycerides, and increases the concentration of HDL.50 This drug apparently directly affects ovarian steroidogenesis by reducing the production of androgens.50 The recommended dose is 500mg or 850mg three times per day.50
Response to treatment with insulin sensitizing agents is directly proportional to BMI, fasting insulin, fasting glucose, HOMA, total and LDL cholesterol, and blood pressure.50 The use of metformin is indicated in cases of increased peripheral resistance to insulin and, associated with PCOS, in cases of adult woman acne.50 The most common side effects are diarrhea, nausea, vomiting, flatulence, and anorexia.50 The contraindications are: renal disease, metabolic acidosis, congestive heart failure, and hypersensitivity to metformin.50
Contraceptives
Oral contraceptives (OC) are normally two-component compounds: i) estrogen (usually ethinyl estradiol, at high doses of up to 100µ in the past, currently of 35µ, 30µ, 20µ and 15µ), and ii) progestogen. 51
Estrogen stimulates liver production of androgen binding protein (SHBG - sex hormone binding globulin), indirectly helping reduce free testosterone levels and thus its peripheral effects. 51 Estrogen inhibits the hypothalamic-hypophysis-gonads axis, also reducing the activity of 5-α-reductase.51
Progestins are derivatives of testosterone, with the older, first generation ones (norgestrel, levonorgestrel) being potentially androgenic, and can possibly trigger androgenic effects such as acne, hirsutism, alopecia, and lipid and glucose metabolic abnormalities and/or worsen adult woman acne.51 The newer, second or third generation progestins tend to be more antiandrogenic.51 There are reports of an increased risk of acute myocardial infarction in women under use of OC, especially in the obese and smokers.51 Women with this profile must avoid OC use.51
Oral contraceptives suppress hypophysis production of gonadotropins, block ovulation, and decrease ovarian production of androgens.52 The best associations for treatment of acne in adult women are those involving ethinyl estradiol and cyproterone acetate or second, third or last generation progestinic components, such as drospirenone or chlormadinone.52 Newer progestins are better tolerated, nonetheless they have a slightly smaller antiandrogenic efficacy than that of the cyproterone acetate.52
There are individual variations in responses, and therefore if a woman is in good health while taking a specific contraceptive, even an old generation one, there is no indication of change regarding the treatment of adult woman acne.52 The opposite also applies: if a woman using a contraceptive with good indication for acne for more than six months does not respond well, changing to another containing a different progestin class can be attempted.52 A good marker for the response to the contraceptive is the dosage of SHBG, which increases with the use of estrogen.52
Side effects of antiandrogens are weight gain, headache, gastric disturbances, depression, decreased libido, edema, feminization of male fetus, irritability, breast pain, melasma, uterine bleeding, and liver alterations.53
Contraindications to the use of antiandrogens are: cardiovascular disease, thromboembolic events, pregnancy, genital bleeding, and liver disorders.53
Acne is not a life-threatening condition, nevertheless it causes both physical and psychological alterations, due to the fact that it can leave scars on the face or trunk. This occurs in all age groups. However when dealing with 20-40 year-old women who are economically and socially active, this picture can bring a lack of self confidence, social inhibition, depression, and anxiety. The proper approach to adult woman acne - both investigative and therapeutic - by the dermatologist can have a significant positive physical and emotional impact on the lives of these women.
1. Winston MH, Shalita AR. Acne vulgaris. Pathogenesis and treatment. Pediat Clin North Am.1991;38(4):889-903.
2. Yenter BA, Hick JR, Reese EL, Ulhas A, Feldman SR, Balkrishnan R. Acne vulgaris in the United States: a descriptive epidemiology. Cutis. 2010;86(2):94-9.
3. Goulden V, Clarck S, Cunliffe W. Post-adolescent acne: a review of clinical features. Br J Dermatol.1997;136(1):66-70.
4. Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. J Am Acad Dermatol.1999;41(4):577-80.
5. Jansen T, Janben OE, Plewig G. Acne tarda. Acne in adults. Hautarzt. 2013;64(4):241-51.
6. Dréno B, Layton A, Zouboulis CC, Lopez-Estebarans JL, Zalewska-Janowska A, Bagatin E, et al. Adult female acne: a new paradigm. J Eur Acad Dermatol Venereol. 2013;27(9):1063-70.
7. Holzmann R, Shakery K. Postadolescent acne in female. Skin Pharmacol Physiol. 2014;27(Suppl 1):3-8.
8. Perkins A, Cheng C, Hillebrand G, Miyamoto K, Kimball AB. Comparison of the epidemiology of acne vulgaris among Caucasian, Asian, Continental Indian and African American women. J Eur Acad Dermatol Venereol. 2011;25(9):1054-60.
9. Poli F, Dréno B, Verschoore M. An epidemiological study of acne in female adults: results of a survey conducted in France. J Eur Acad Dermatol Venereol. 2001;15(6):541-5.
10. Yazici K,BAZ K, Yzazici AE, Kokturk A, Tot S, Demirseren D, et al. Disease-specific quality of life is associated with anxiety and depression in patients with acne. J Eur Acad Dermatol Venereol. 2004;18(4):435-9.
11. Callender VD, Alexis AF, Daniels SR, Kawata AK, Burk CT, Wilcox TK, et al. Racial differences in clinical characteristics, perceptions and behaviors, and psychosocial impact of adult female acne. J Clin Aesthet Dermatol. 2014;7(7):19-31.
12. Zaraa I, Belghith I, Ben Alaya N, Trojjet S, Mokni M, Ben Osman A.Severity of acne and its impact on quality of life. Skinmed. 2013;11(3):148-53.
13. Zeichner J. Evaluating and treating the adult female patient with acne. J Drugs Dermatol. 2013;12(12):1418-27.
14. Kim GK, Michaels BD. Post-adolescent acne in women: more common and more clinical considerations. J Drugs Dermatol. 2012;11(6):708-13.
15. Dréno B, Thiboutot D, Layton AM, Berson D, Perez M, Kang S, et al. Large-scale international study enhances understanding of an emerging acne population: adult females. J Eur Acad Dermatol Venereol. 2014;29(6):1096-106.
16. Thiboutot D, Gilliland K, Light J, Lookingbill D. Androgen metabolism in sebaceous glands from subjects with and without acne. Arch Dermatol. 1999;135(9):1041.
17. Yarak S, Bagatin, E Hassun KM, Parada MOAB, Talarico Filho S. Hiperandrogenismo e pele: síndrome do ovario policístico e resistência periférica a insulina. An Bras Dermatol. 2005;80(4):395-410.
18. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19-25.
19. Kamangar F, Shinkai K. Acne in adult female patient: a practical approach. Int J Dermatol. 2012;51(10):1162-74.
20. Khunger N, Kumar C. A clinico-epidemiological study of adult acne: is it different from adolescent acne? Indian J Dermatol Venereol Leprol. 2012;78(3):335-41.
21. Dumont-Wallon G, Dréno B. Specificity of acne in women older than 25 years. Presse Med. 2008;37(1):585-91.
22. Sobral Filho JF, Silva CNA, Rodrigues JC, Rodrigues JLTD, Aboui-Azouz M. Avaliação da herdabilidade e concordância da acne vulgar em gêmeos. An Bras Dermatol. 2007;72(5):225-8.
23. Dessinioti C, Antoniou C, Katsambas A. Acneiformeruptions. Clin Dermatol. 2014;32(1):24-34.
24. Preneau S, Dreno B. Female acne – a diferente subtype of teenager acne? J Eur Acad Dermatol Venereol. 2012;26(3):277-82.
25. Pontes TC, Filho GMCF, Trindade ASP, Filho JFS. Incidência de acne vulgar em adultos jovens usuários de suplementos protéico-calóricos na cidade de João Pessoa – PB. An Bras Dermatol. 2013;88(6):909-14.
26. Ribeiro, BM. Acne da mulher adulta: análise clínica, etiológica e de imagem. Brasília. Dissertação (Mestrado em Ciências da Saúde) - ESCS/FEPECS/SES/DF; 2014.
27. Albuquerque RG, Rocha MA, Bagatin E, Tufik S, Andersen ML. Could adult female acne be associated with modern life? Arch Dermatol Res. 2014;306(8):683-8.
28. Emil AT, Ariane KK, Valerie DC. Understanding the burden of adult female acne. J Clin Aesthet Dermatol. 2014;7(2):22-30.
29. Capitanio B, Sinagra JL, Picardo M. Acne and smoking. Dermatoendocrinol. 2009;1(3):129-35.
30. Yang YS, Lim HK, Hong KK, Shin MK et al. Cigarette smoke-induced interleukin- 1 alpha may be involved in the pathogenesis of adult acne. Ann Dermatol. 2014;26(1):11-6.
31. Geller L, Rosen J, Frankel A, Goldenberg G. Perimenstrual flare of adult acne. J Clin Aesthet Dermatol. 2014;7(8):30-4.
32. Clark CM, Rudolph J, Gerber DA, Click S, Shalita AR, Lowenstein EJ. Dermatologic manifestation of hyperandrogenism: a retrospective chart review. Skinmed. 2014;12(2):84-8.
33. Gabrielli L, Aquino EML. Polycystic ovary syndrome in Salvador,Brazil: a prevalence study in primary healthcare. Reprod Biol Endocrinol. 2012;10:96.
34. Da Cunha MG, Fonseca FL, Machado CD. Androgenic hormone profile of adult women with acne. Dermatology. 2013;226(2):167-71.
35. Balem EMF, Dardes RCM, Carneiro ALB, Haidar MA. The effectiveness of the levonorgestrel-releasing intrauterine system for hormone replacement therapy in the peri and postmenopausal women. Femina. 2010;38(3):141-146.
36. Rzany B, Nast A. Acne treatment in the field: how guidelines and other sources can be included in daily practice. J Eur Acad Dermatol Venereol. 2013;27(Suppl 2):2-5.
37. Thomas B, Tan JKL. Adherence optimization in acne management. Skin Ther Lett. 2011;7(1):1-3.
38. Gollnick H, Cunliffe W, Berson D, Dreno B, Finlay A, Leyden JJ, et al. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49(1 Suppl):S1-37.
39. Berson D, Alexis A. Adapalene 0,3% for the treatment of acne in women. J Clin Aesthet Dermatol. 2013;6(10):32-5.
40. Lessner E, Fisher S, Kobrael K, Osleber M, Lessner R, Elliot L, et al. Spironolactone and topical retinoids in adult female cyclical acne. J Drugs Dermatol. 2014;13(2):126-9.
41. Sagransky M, Yentzel BA, Feldman SR. Benzoyl peroxide: a review of its current use in the treatment of acne vulgaris. Expert Opin Pharmacother. 2009;10(16):2555-2562.
42. Thiboutot D, Gollnick H, Bettoli V, Dréno B, et al.Global Alliance to Improve Outcomes in Acne. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009 May;60(5 Suppl):S1-50.
43. Sieber MA, Hegel JK. Azelaic acid: properties and mode of action. Skin Pharmacol Physiol. 2014;27(1):9-17.
44. Dréno B, Bettoli V, Ochsendorf F, Layton A, Mobacken H, Degreef H, et al. European recommendations on the use of oral antibiotics for acne. Eur J Dermatol. 2004;14(6):391-9.
45. Preneau S, Dessinioti C, Nguyen JM, Katsambas A, Dréno B. Predictive markers of response to isotretinoin in female acne. Eur J Dermatol. 2013;23(4):478-86.
46. Thiboutot D, Chen W. Update and future of hormonal therapy in acne. Dermatology. 2003;20(1):57-67.
47. Ramos e Silva M. Fundamentos da Dermatologia. Rio de Janeiro: Editora Atheneu; 2010.
48. Salavastru CM, Fritz K, TiplicaGS.Spironolactone in dermatological treatment. On and off label indications. Hautarzt. 2014;64(10):762-7.
49. Smith EV, Grindley DJ, Willians HC. What’s new in acne? An analysis of systematic reviews published in 2009-2010. Clin Exp Dermatol. 2011;36(2):119-22.
50. Meyer BH, Muller FO, de la Rey N, Luus HG, Rosenkranz B. The effects of buserelin microparticles on ovarian function in healthy women. S Afr Med J. 1995;85(8):766-77.
51. Johnson NP. Metformin use in women with polycystic ovary syndrome. Ann Transl Med. 2014;2(6):56.
52. Brynhildsen J. Combined hormonal contraceptives: prescribing patterns, compliance, and benefits versus risks. Ther Adv Drug Set. 2014;5(5):201-13.
53. Buzney E, Sheu J, Busney C, Reynolds RV. Polycystic ovary syndrome: a review for dermatologists. J Am Acad Dermatol. 2014;71(5):859.
54. Krausz A, Friedman AJ. Cutaneous hyperandrogenism: role of antiandrogen therapy in acne, hirsutism and androgenetic alopecia. J Drugs Dermatol. 2013;12(11):1297-300.
This study was carried out at the Dermatology Department, Faculdade de Ciências Médicas de Minas Gerais - Belo Horizonte (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}