


Felipe Bochnia Cerci
Keywords: MOHS SURGERY; EAR CARTILAGE; SURGICAL FLAPS; NOSE NEOPLASMS; BASAL CELL CARCINOMA
The restoration of nasal shape and function after Mohs surgery requires adequate surgical planning. Extensive and deep nasal defects, especially those located in the nasal ala, may require a cartilage graft to help restore function, anatomy, and nasal aesthetics.1,2 In dermatologic surgery, the most common donor site for a cartilage graft is the ear. When selecting the donor subunit - anti-helix/scaphoid fossa or concha - the differences in the cartilage of these locations, as well as the morbidity and ease of removal of the graft should be considered.3 Cartilage grafts are usually performed with interpolation flaps.1,2 However, they can also be associated with single stage flaps, skin grafts, and healing by secondary intention. 4-6 The main functions of the cartilage graft are to prevent tissue contraction and distortion, to support "heavy" flaps in order to avoid the collapse of the nasal ala, to keep the nasal valve open, and to provide support for a better contour. The purpose of the present study was to evaluate the usefulness of auricular cartilage grafts in nasal reconstruction after Mohs micrographic surgery, as well as to describe a cartilage graft harvesting technique.
Patients
A retrospective study was performed with 10 patients whose nasal defects resulting from Mohs micrographic surgery needed cartilage graft. The cases were selected from a public hospital, from August 2014 to March 2015.
Based on the review and analysis of medical records and extensive photographic documentation, the following demographic and surgical data were analyzed: age, gender, tumor characteristics, subunits involved, number of Mohs stages, additional measures for patient comfort, type of repair performed, cartilage donor area (auricular subunit and location of incision), use of anticoagulants, smoking habits, complications, follow-up and results. Before or after surgery, all patients signed a free and informed term of consent authorizing the publication of the photographs in scientific journals. All procedures (Mohs surgery to remove the tumor and subsequent reconstruction) were performed under local anesthesia. Local nerve blocks supplemented local anesthesia in some cases. Patients received oral benzodiazepines for comfort when required, before or during the procedure. All patients were restored with interpolated flaps, with a second stage being necessary three to four weeks after the first surgery.
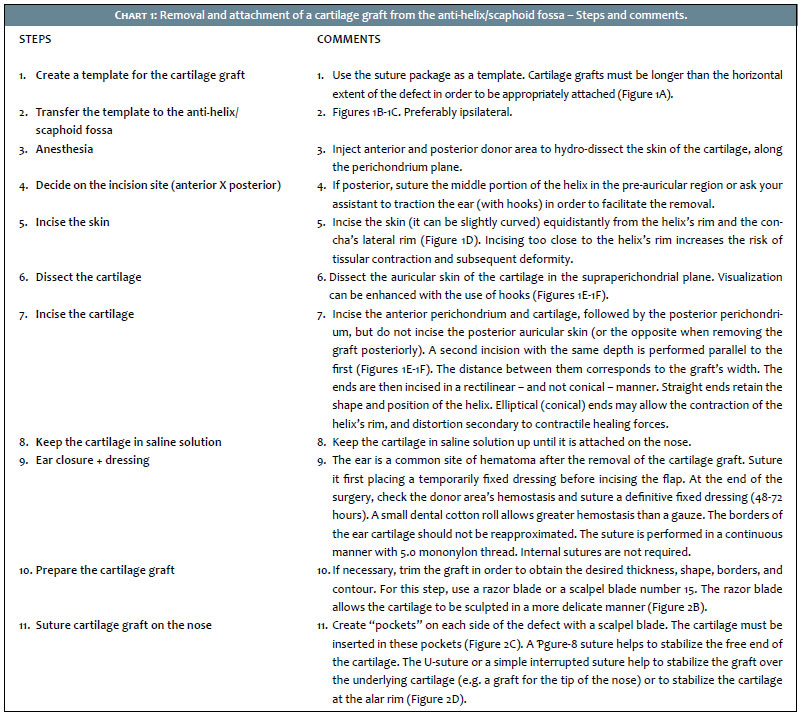
Harvesting technique
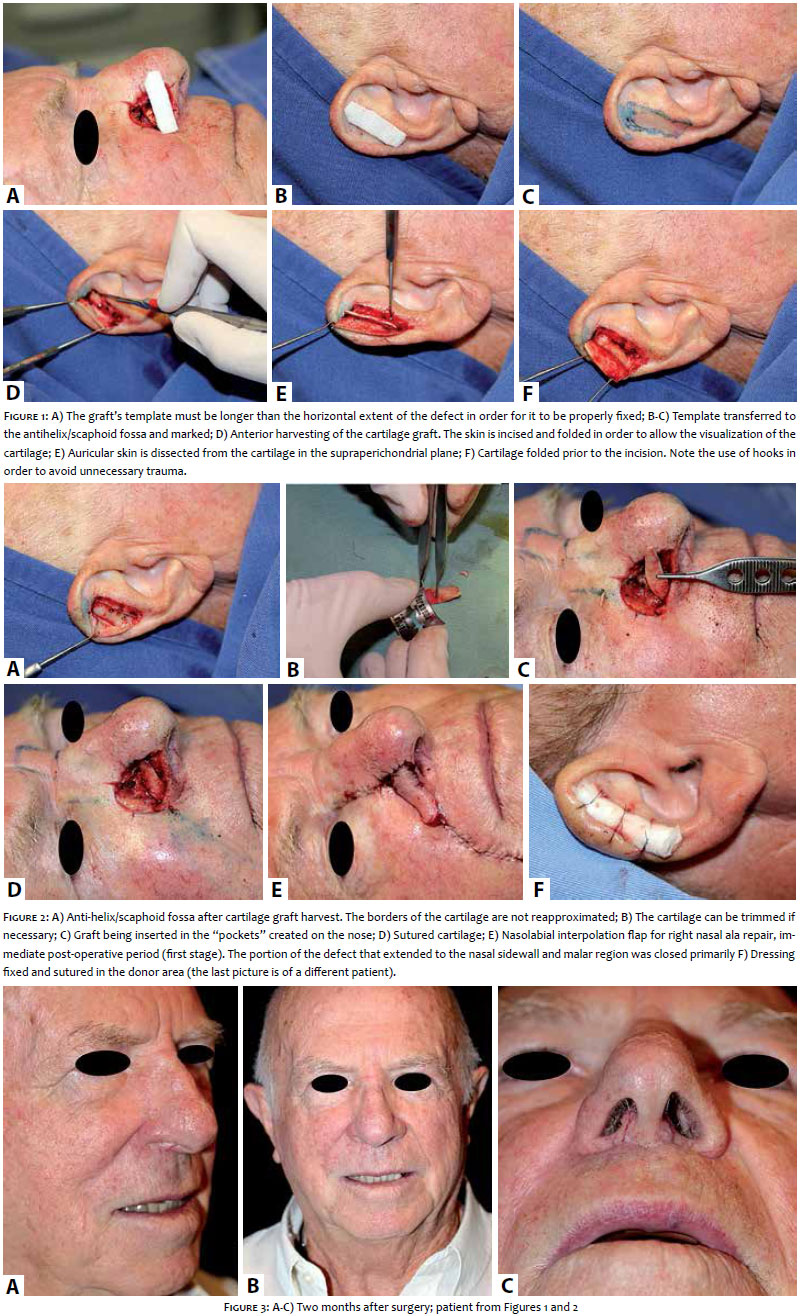
Chart 1 describes step-by-step how to perform the removal and attachment/fixation of the anti-helix/scaphoid fossa cartilage graft. If harvesting from the conchal bowl, technique is similar. The entire concha can be removed without significant risk of auricular distortion. However, removing the graft too close to the ear canal should be avoided due to the risk of late post-operative retraction. (Figures 1-3)
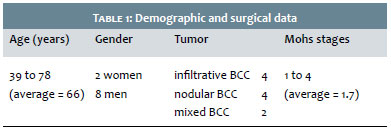
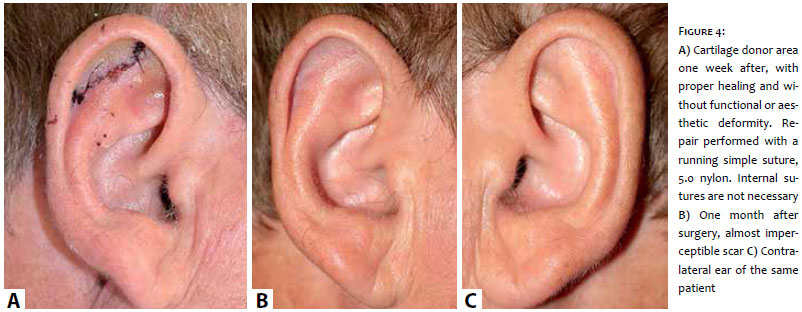
Ten patients were included in the study. Demographic and surgical data are shown in Table 1. The patients' ages ranged from 39 to 78 years (mean = 66 years) and most were men (eight men and two women). All tumors were basal cell carcinoma and the most common subtypes were infiltrative (n = 4) and nodular (n = 4). The remaining patients had mixed basal cell carcinoma, with infiltrating and nodular components. The number of Mohs surgery stages needed to obtain free margins ranged from 1 to 4 (mean = 1.7). Regarding additional measures for patient comfort, 3 (30%) received oral benzodiazepines (0.5 mg to 1.0 mg lorazepam) as adjuvants for local anesthesia. Infraorbital nerve block was performed in 5 patients (50%). Seven patients (70%) had defects located mainly on the nasal ala, and were repaired with a nasolabial interpolation flap alone or combined with other closure methods. Three (30%) patients had more extensive defects affecting multiple nasal subunits and were repaired with paramedian forehead flaps. The cartilage graft was removed from the antihelix/scaphoid fossa (n = 6) or concha (n = 4). All cartilage antihelix/scaphoid fossa grafts were removed via anterior incision, while conchal grafts were removed via posterior incision. Three patients had full-thickness defects. In one of them, the nasal mucosa was recreated with a hinge flap from the nasal sidewall while in the other two, it was closed primarily due to the small size of the mucosal defect. Only one patient was a smoker. No patients were on anticoagulants. One of them, however, had post-operative bleeding and hematoma, which drained spontaneously. Excellent functional and aesthetic results were achieved in all patients. There was no infection, hypertrophic scarring, keloid, or distortion of the ear in any of the cases, and the donor area has become virtually unnoticeable after a few months. (Figure 4). The follow-up period ranged from two to nine months (average = seven months), without tumor recurrence.
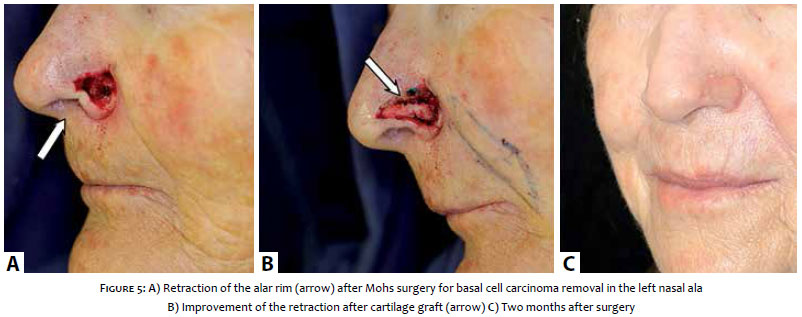
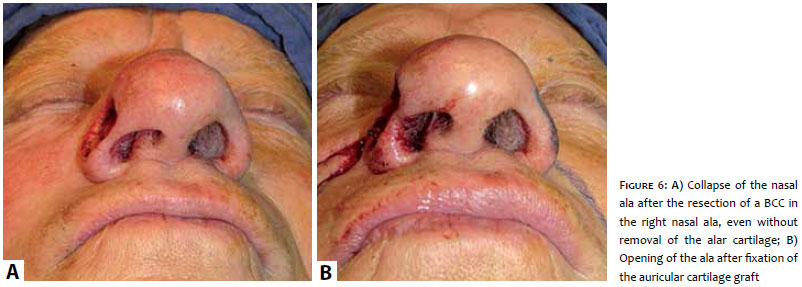
Many factors must be taken into consideration when planning a nasal reconstruction. In most patients, soft tissue restoration is sufficient to obtain optimal functional and aesthetic results. However, in certain cases an auricular cartilage graft can be necessary for the proper restoration of the nasal ala and valve. 4 It is crucial to recognize those patients who will benefit from the cartilage graft. Signs that help to identify them include the spontaneous collapse of the nasal ala/valve or during the inspiration after the removal of the tumor, or retraction of the nasal rim. In some cases, even without retraction of the rim during surgery, it may occur later due to scarring. The precise location for the fixation of the graft, as well as its size and shape, will result in different benefits. If the objective is only to avoid or correct the retraction of the nasal rim, the cartilage graft can be smaller and should be inserted considerably close to the alar rim (Figure 5). If, however, there is a major collapse of the nasal valve/ala (Figure 6), the cartilage graft should be larger and be placed in the middle and upper thirds of the ala. For the projection of the nasal tip, the grafts should be directly placed on it. Cartilage grafts can be structural (native cartilage is present but there is a need for additional cartilage to support) or restorative (replacement of removed cartilage). Cartilage grafts for the nasal ala are usually structural and non-restorative, since there is no cartilage in most of the nasal ala, but only fibrofatty tissue. Structural functions of the cartilage include: 1) to prevent tissue contraction and distortion, 2) to support "heavy" flaps, 3) to maintain the nasal valve open, and 4) to provide support for the contour.7 Cartilage donor areas include the anti-helix/ scaphoid fossa and the auricular concha.4,8 Cartilage from the anti-helix/scaphoid fossa is ideal for long, flexible, and straight segments, while that of the concha is ideal for grafts that require more curvature, substance, and stiffness.
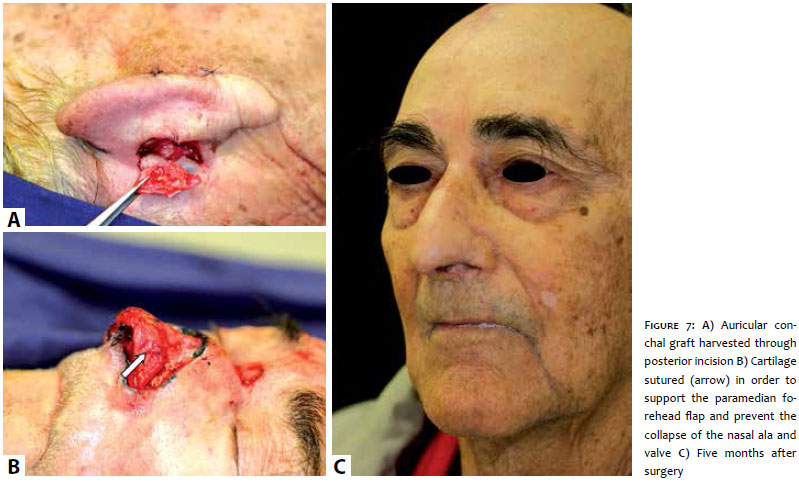
In the present study, 6 patients (60%) had a cartilage graft removed from the antihelix/scaphoid fossa, while 4 patients (40%) had it removed from the concha. Of these, 3 patients had large defects that were repaired with a paramedian forehead flap (Figure 7).
The incisions for removing the cartilage can be performed anteriorly or posteriorly. Anterior incisions are easier to access, however they result in more visible scars.1,2 Although grafts from the antihelix/scaphoid fossa were removed anteriorly, the incision healed well and was hardly noticeable in all patients. It may be necessary to sculpt the graft to obtain the desired thickness, shape, borders, and contour. This must be done carefully, since the cartilage is a fragile structure and may fracture during the process. A scalpel blade 15 is traditionally used to carve, however a razor blade allows the graft's contours to be sculpted more gently. Cartilage grafts can be safely harvested under local anesthesia with low complication rates.1-3,9 Postoperative pain at the cartilage donor site can be significant, therefore adequate analgesia (non-steroidal anti-inflammatory/powerful analgesic) must be provided to all patients.1,2
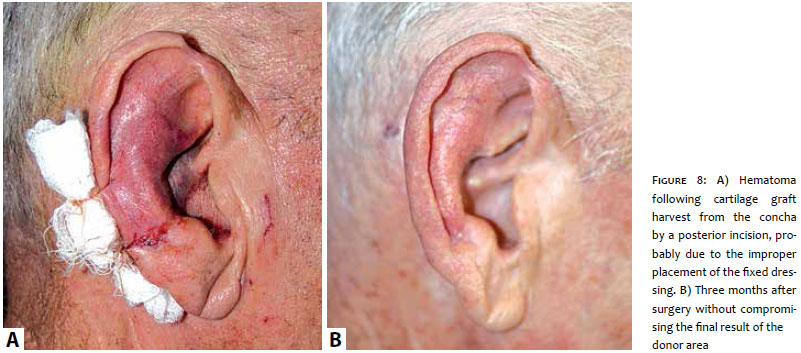
The primary disadvantage of the cartilage graft is the additional morbidity of creating a second surgical site. Although rare, hematoma, infection, non-infectious chondritis, and anatomical distortion can occur in the donor ear.10 Careful hemostasis and a bolster dressing placed for 48 to 72 hours help to prevent the formation of hematomas. The only patient who developed post-operative hematoma had the dressing placed inappropriately, too far from the real donor area. Therefore, bolster dressings should be placed in the precise location of the incision. If necessary, they can even be fixed anterior and posteriorly. None of the patients developed infection or non-infectious chondritis in the present study. However, all were given oral antibiotics post-operatively due to the length of the surgery, the performance of a cartilage graft and the location of the defect (nose) - though this recommendation is controversial. In a recent study by Sage et al.,3 the donor area's complication rate (3%) was lower than in the present study (10%, corresponding to one hematoma). The reduced number of cases in the present study, however, results in a single complication having a greater statistical impact. (Figure 8)
Ear cartilage grafts are a versatile, reliable, and predictable method of providing structural support in nasal reconstruction. They can be easily, quickly, and safely harvested, without harming the donor area. It is crucial to identify patients who can benefit from the technique. Through careful planning and proper execution, auricular cartilage grafts significantly improve the results of nasal reconstructions in selected cases.
1. Cerci FB, Nguyen TH. Paramedian forehead flap for complex nasal defects following Mohs micrographic surgery. Surg Cosmet Dermatol. 2014;6(1):17-24.
2. Cerci FB, Nguyen TH. Nasolabial interpolation flap for alar reconstruction after Mohs micrographic surgery. Surg Cosmet Dermatol. 2014;6(2):113-20.
3. Sage RJ, Leach BC, Cook J. Antihelical cartilage grafts for reconstruction of Mohs micrographic surgery defects. Dermatol Surg. 2012;38(12):1930-7.
4. Byrd DR, Otley CC, Nguyen TH. Alar batten cartilage grafting in nasal reconstruction: functional and cosmetic results. J Am Acad Dermatol.2000;43(5 Pt 1):833-6.
5. Zopf DA, Iams W, Kin JC, Baker SR, Moyer JS. Full-thickness skin graft overlying a separately harvested auricular cartilage graft for nasal alar reconstruction. JAMA Facial Plastic Surg. 2013;15(2):131-4.
6. Ibrahimi OA, Campbell T, Youker S, Sisein DB. Nonanatomic free cartilage batten grafting with second intention healing for defects on the distal nose. J Drugs Dermatol. 2012;11(1):46-50.
7. Nguyen TH. Staged interpolation flaps. In: Roher TE, Cook JL, Nguyen TH, Mellete Jr, JR, editors. Flaps and grafts in dermatologic surgery. New York: Elsevier; 2007. p. 91-105.
8. Ratner D, Skouge JW. Surgical pearl: the use of free cartilage grafts in nasal alar reconstruction. J Am Acad Dermatol. 1997;36(4):622-4.
9. Kaplan AL, Cook JL. The incidences of chondritis and perichondritis associated with the surgical manipulation of auricular cartilage. Dermatol Surg. 2004;30(1):58-62; discussion 62.
10. Adams DC, Ramsey ML. Grafts in dermatologic surgery: review and update on full- and split-thickness skin grafts, free cartilage grafts, and composite grafts. Dermatol Surg. 2005;31(8 Pt 2):1055-67.
This study was performed at Hospital Santa Casa de Curitiba - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}